Mastering Carpal Tunnel Release: Mini-Palm, Open, and Endoscopic Techniques
Key Takeaway
The "mini-palm" open carpal tunnel release offers a reliable, minimally invasive approach to median nerve decompression. By utilizing a precise 3.0 cm incision in line with the third web space, surgeons can effectively divide the transverse carpal ligament while minimizing risk to the palmar cutaneous branch. This guide details the step-by-step surgical technique, anatomical considerations, and postoperative protocols essential for optimal patient outcomes.
Introduction to Median Nerve Decompression
Carpal tunnel syndrome (CTS) remains the most prevalent compression neuropathy in the upper extremity, necessitating surgical intervention when conservative measures—such as splinting, corticosteroid injections, and ergonomic modifications—fail to provide durable relief. The primary objective of surgical intervention is the complete division of the flexor retinaculum to decompress the median nerve, thereby restoring normal intraneural microcirculation and preventing irreversible axonal degradation.
While the traditional open carpal tunnel release has long been the gold standard, advancements in surgical technique have popularized the “Mini-Palm” Open Carpal Tunnel Release and Endoscopic Carpal Tunnel Release (ECTR). These modern iterations aim to minimize iatrogenic trauma to the palmar fascia, reduce postoperative "pillar pain," and accelerate the patient's return to occupational activities, all while maintaining the safety and efficacy of the classic open approach.
This comprehensive guide delineates the precise surgical anatomy, biomechanical considerations, and step-by-step operative techniques for the mini-palm, standard open, and endoscopic carpal tunnel releases.
Surgical Anatomy and Biomechanics
A profound three-dimensional understanding of the carpal tunnel and its surrounding neurovascular structures is paramount to executing a safe and effective release. The carpal tunnel is a fibro-osseous canal bounded dorsally by the carpal bones and volarly by the flexor retinaculum.
The Flexor Retinaculum Complex
The flexor retinaculum is not a single discrete band but rather a continuous fascial complex comprising three distinct segments:
1. Proximal Segment: The distal deep investing fascia of the forearm.
2. Central Segment: The transverse carpal ligament (TCL) proper, which attaches radially to the scaphoid tuberosity and trapezium crest, and ulnarly to the pisiform and hook of the hamate.
3. Distal Segment: The aponeurosis between the thenar and hypothenar musculature.
Surgical Warning: A successful carpal tunnel release requires the complete division of all three components of the flexor retinaculum. Incomplete release, particularly of the distal aponeurotic fibers, is the leading cause of recurrent or persistent CTS.
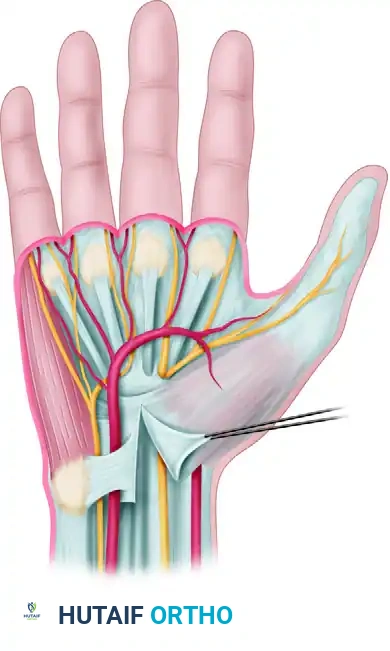
Anatomical relationships of the deep transverse carpal ligament, highlighting the proximity of the median nerve, ulnar nerve, and superficial palmar arterial arch.
The Median Nerve and Its Branches
The median nerve traverses the carpal tunnel alongside nine flexor tendons (four flexor digitorum superficialis, four flexor digitorum profundus, and the flexor pollicis longus). Two critical branches of the median nerve demand meticulous attention during surgery:
1. The Palmar Cutaneous Branch of the Median Nerve (PCBMN):
The PCBMN arises approximately 5 cm proximal to the wrist crease, traveling in the interval between the palmaris longus (PL) and the flexor carpi radialis (FCR) tendons. It provides sensation to the base of the thenar eminence.

Care must be taken in any wrist incision to avoid cutting the palmar cutaneous branch of the median nerve, which lies in the vulnerable interval between the PL and FCR.
Clinical Pearl: Iatrogenic transection of the PCBMN frequently results in a highly morbid, painful neuroma. If this nerve is inadvertently severed during exposure, do not attempt primary repair; instead, section it sharply at its origin and allow it to retract into healthy proximal muscle belly to minimize neuroma symptoms.
2. The Recurrent Motor Branch (Thenar Branch):
The recurrent motor branch supplies the thenar musculature (abductor pollicis brevis, opponens pollicis, and the superficial head of the flexor pollicis brevis). Its anatomical course is highly variable, making it susceptible to injury if the TCL is divided blindly or too radially. The variations include:
* Extraligamentous (46%): Arises distal to the TCL and recurrently enters the thenar musculature.
* Subligamentous (31%): Arises within the carpal tunnel and travels deep to the TCL before entering the muscle.
* Transligamentous (23%): Pierces directly through the fibers of the TCL.

Extraligamentous course of the thenar branch (46% incidence).

Subligamentous course of the thenar branch (31% incidence).

Transligamentous course of the thenar branch (23% incidence).
The Superficial Palmar Arterial Arch
The superficial palmar arch crosses the palm transversely, typically located 5 to 8 mm distal to the distal margin of the transverse carpal ligament. Dissection extending too far distally beyond the TCL places this critical vascular structure at severe risk.
Surgical Technique 1: The “Mini-Palm” Open Carpal Tunnel Release
The "mini-palm" technique provides excellent visualization of the transverse carpal ligament while minimizing the length of the palmar incision, thereby reducing postoperative scarring and pillar pain.
Step 1: Incision Planning and Marking
Proper incision placement is the most critical step in avoiding the PCBMN and the recurrent motor branch.
* Mark the planned surgical incision with a sterile skin pen.
* The longitudinal incision should begin just distal to the distal wrist flexion crease.
* Position the incision slightly ulnar to the midline of the wrist (using a center dot reference point).
* Extend the incision distally for exactly 3.0 cm, keeping it strictly in line with the third web space (the axis of the ring finger).
Surgical Note: Only rarely is it necessary to extend the incision proximally into the distal forearm. If proximal extension is required, angle the incision ulnarly to avoid crossing the wrist flexion creases at a right angle and to stay clear of the PCBMN.
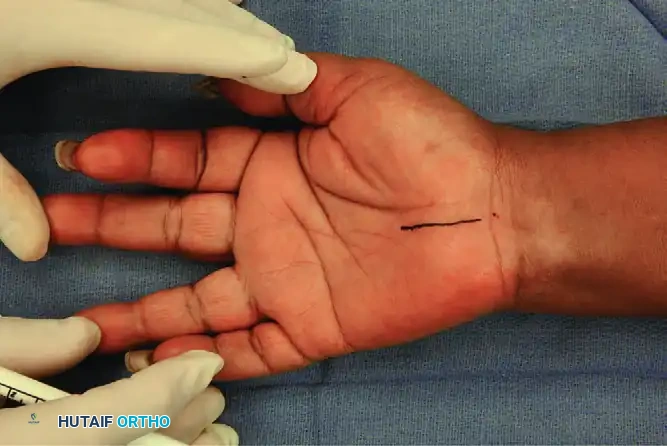
The incision is marked with a skin pen, extending 3.0 cm distally in line with the third web space.
Step 2: Superficial Dissection and Exposure
- Incise the skin and subcutaneous tissue sharply.
- Identify the palmar fascia. Using subcutaneous blunt dissection, retract the parallel palmar fascia fibers and the hypothenar fat pad to expose the underlying transverse carpal ligament (TCL).
- Self-retaining retractors (e.g., a Weitlaner or specialized hand retractors) are placed to maintain a clear visual field.
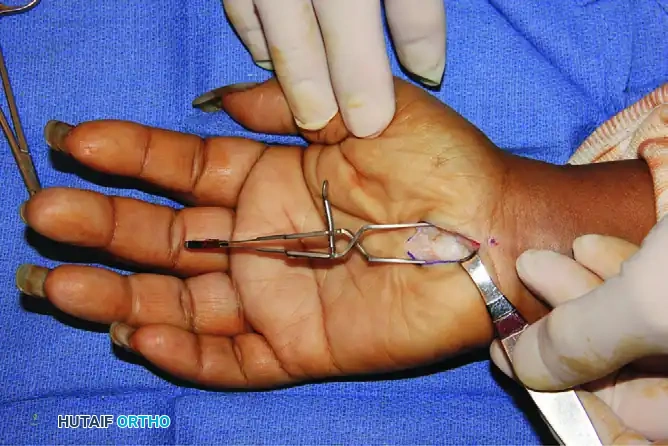
Exposure of the transverse carpal ligament (TCL) following the retraction of parallel palmar fascia fibers and hypothenar fat.
Step 3: Division of the Transverse Carpal Ligament
- Identify the proximal and distal extents of the TCL.
- Carefully divide the TCL longitudinally, staying strictly to the ulnar side of the median nerve to avoid the recurrent motor branch.
- Once the TCL is completely divided, use Metzenbaum scissors to divide the distal 2.0 cm of the antebrachial fascia proximally beneath the wrist crease.
- Verify that the distal aponeurotic fibers between the thenar and hypothenar muscles are completely released.
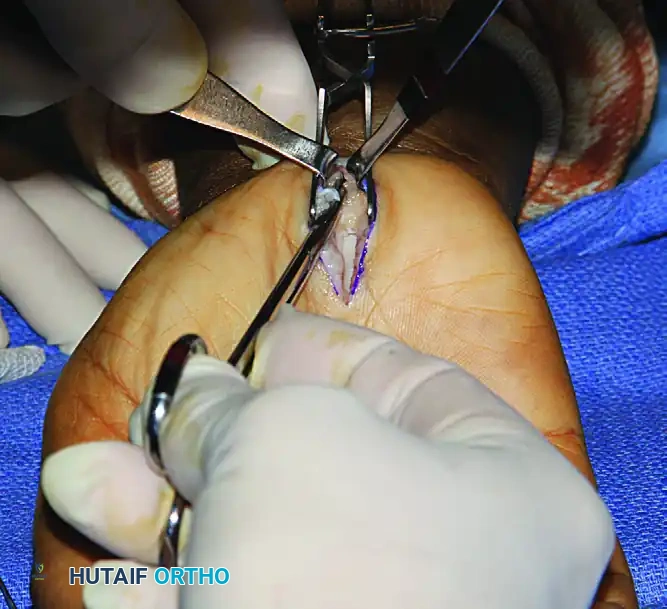
After the division of the TCL, the distal 2.0 cm of the antebrachial fascia is divided proximally with Metzenbaum scissors.
Step 4: Nerve Inspection and Neurolysis
- Inspect the median nerve. It should appear hyperemic (the "blush" sign) once decompressed.
- If the median nerve is found to be densely adherent to the divided radial leaf of the TCL, a careful external neurolysis may be indicated to free the nerve and prevent postoperative tethering.
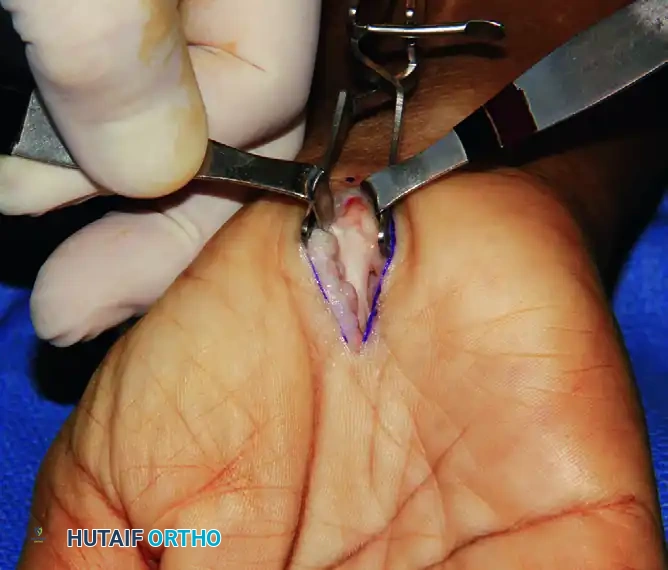
In this patient, the median nerve was found adherent to the divided radial TCL leaf and subsequently required external neurolysis.
Step 5: Closure and Dressing Application
- Deflate the tourniquet and achieve meticulous hemostasis. Bipolar electrocautery should be used sparingly and far from the nerve.
- Close the skin in a routine fashion using non-absorbable interrupted sutures (e.g., 4-0 or 5-0 Nylon). Do not close the deep fascial layers, as this will recreate the compression.
- Apply a sterile, bulky compressive dressing to minimize postoperative hematoma formation.

The palmar incision is closed meticulously with interrupted sutures.

Application of the initial sterile gauze over the closed incision.

A soft, bulky compressive dressing is applied to the hand and wrist.

Final appearance of the compressive dressing, allowing for digital mobility while protecting the surgical site.
Surgical Technique 2: Standard Open Carpal Tunnel Release
While the mini-palm technique is preferred for routine cases, a standard open approach is necessary for complex presentations, revision surgeries, or when extensive tenosynovectomy is required.
Incision and Approach
- The thenar crease takes a variable course. Palmar incisions must be placed well ulnar to the thenar crease to avoid the PCBMN.
- Pitfall: A curved incision that runs ulnar and strictly parallel to the thenar crease is not advisable, as the proximal portion of the PCBMN may be placed at severe risk of transection.
- Maintain a longitudinal orientation so that the incision remains generally to the ulnar side of the long finger axis, or along the radial border of the fourth ray.
- If proximal extension is required, angle the incision toward the ulnar side of the wrist to avoid crossing the flexor creases at a right angle.
Deep Dissection and Decompression
- Incise and reflect the skin and subcutaneous tissue.
- Identify the palmar fascia from the wrist flexion crease distally and the distal forearm antebrachial fascia proximally via subcutaneous blunt dissection.
- Split the palmar fascia to expose the underlying TCL.
- Identify the TCL and carefully divide it. Always cut under direct vision, protecting the median nerve beneath it.
- Be acutely aware that fibers of the TCL can extend distally farther than expected. Ensure the release is complete up to the superficial palmar arterial arch, taking care not to injure the arch (located 5 to 8 mm distal to the TCL margin).
Managing Anatomical Anomalies
During an open release, the surgeon must remain vigilant for potential anatomical anomalies within the carpal canal, which may include:
* Anomalous connections between the flexor pollicis longus (FPL) and the index flexor digitorum profundus (FDP) tendons (Linburg-Comstock anomaly).
* Anomalous muscle bellies of the flexor digitorum superficialis (FDS), palmaris longus, or lumbricals extending proximally into the tunnel.
* Aberrant median and ulnar nerve branches or interconnections (e.g., Martin-Gruber or Riche-Cannieu anastomoses).
Tenosynovectomy
- Inspect the flexor tenosynovium. In patients with severe rheumatoid arthritis, amyloidosis, or chronic non-specific tenosynovitis, a formal tenosynovectomy may be indicated to adequately reduce the volume of the carpal tunnel contents.
Endoscopic Carpal Tunnel Release (ECTR)
Endoscopic techniques have gained significant traction due to their potential for reduced palmar scarring, decreased ulnar "pillar" pain, and a more rapid return to work and activities (often 2 weeks sooner than open release). However, long-term studies comparing open and endoscopic releases demonstrate no significant differences in final functional outcomes. The primary benefits of ECTR—improved grip strength and pain relief—are most pronounced within the first 12 weeks postoperatively.
Risks and Complications of ECTR
ECTR is a technically demanding procedure with a steep learning curve. Cadaveric studies highlight the perilous proximity of the median and ulnar nerves, the superficial palmar arterial arch, and the flexor tendons to the endoscopic blade.
Inherent problems related to ECTR include:
1. A highly technically demanding procedure requiring specialized training.
2. A limited visual field that prevents the inspection of other structures (e.g., anomalous muscles, tumors).
3. High vulnerability of the median nerve, flexor tendons, and superficial palmar arch to iatrogenic injury.
4. Inability to easily control intraoperative bleeding.
5. Limitations imposed by mechanical or visual failure of the endoscopic equipment.
Agee’s 10 Guidelines for Endoscopic Release
Agee, McCarroll, and North developed the following 10 strict
📚 Medical References
- carpal tunnel release, J Hand Surg 18A:438, 1993.
- Incisions Anson JB, Maddock WG: Callander’s surgical anatomy, 3rd ed, Philadelphia, 1952, Saunders. Brunner JM: Incisions for plastic reconstructive (nonseptic) surgery of the hand, Br J Plast Surg 4:48, 1951.
- Bunnell S: Contractures of the hand from infections and injury, J Bone Joint Surg 14:27, 1932.
- Jobe MT, Caviale P, Milford LW: The digital palmar oblique incision, J Hand Surg 18A:525, 1993.
- Skin Closure Burm JS, Chung CH, Oh SJ: Fist position for skin grafting on the dorsal hand: 1. Analysis of length of the dorsal hand surgery in hand positions, Plast Reconstr Surg 104:1350, 1999.
- Da-Yuan C: Mathematical principle of planar Z-plasty, Plast Reconstr Surg 105:105, 2000.
- Fraulin FO, Thomson HG: First web space deepening: comparing the four-fl ap and fi ve-fl ap Z-plasty: which gives the most gain? Plast Reconstr Surg 104:120, 1999.
- McGregor IA: The Z-plasty in hand surgery, J Bone Joint Surg 49B:448, 1967.
- Peker F, Celebiler O: Y-V advancement with Z-plasty: an effective combined model for release of post-burn fl exion contractures of the fi ngers, Burns 29:479, 2003.
- Seyhan A: Mini Z in Z to relieve the tension on the transverse closure after Z-plasty transposition, Plast Reconstr Surg 101:1635, 1998.
- Shinya K: Dancing girl fl ap: a new fl ap suitable for web release, Ann Plast Surg 43:618, 1999.
- Sinha S, Naik M, Wright V, et al: A single blind, prospective, randomized trial comparing N-butyl 2-cyanoacrylate tissue adhesive (Indermil) and sutures for skin closure in hand surgery, J Hand Surg 26B:264, 2001.
- Suzuki S, Um SC, Kim BM, et al: Versatility of modifi ed planimetric Z-plasties in the treatment of scar contracture, Br J Plast Surg 51:363, 1998.
- Postoperative Management Bruner JM: Problems of postoperative position and motion in surgery of the hand, J Bone Joint Surg 35A:355, 1953.
- Fagan DJ, Evans A, Ghandour A, et al: A controlled clinical trial of postoperative hand elevation at home following day-case surgery, J Hand Surg 29B:458, 2004.
- Sai S, Fujii K, Hiranuma K, et al: Preoperative ampiroxicam reduces postoperative pain after hand surgery, J Hand Surg 26B:377, 2001.
- Tourniquet Boiko M, Roffman M: Evaluation of a novel tourniquet device of bloodless surgery of the hand, J Hand Surg 29B:185, 2004.
- Bolton CF, McFarlane RM: Human pneumatic tourniquet paralysis, Neurology 28:787, 1978.
- Delgado-Martinez AD, Marchal JM, Blanco F, et al: Distal forearm tourniquet for hand surgery, Int Orthop 28:267, 2004.
- Edwards SA, Harper GD, Giddins GE: Effi cacy of forearm versus upper arm tourniquet for local anaesthetic surgery of the hand, J Hand Surg 25B:573, 2000.
- Flatt AE: Tourniquet time in hand surgery, Arch Surg 104:190, 1972.
- Guirguis EM, Bell MSG: The wrist tourniquet: an alternative technique in hand surgery, J Hand Surg 15A:516, 1990.
- Hutchinson DT, McClinton MA: Upper-extremity tourniquet tolerance, J Hand Surg 18A:206, 1993.
- Klenerman L, Biswas M, Hulands GH: Systemic and local effects of the application of a tourniquet, J Bone Joint Surg 62B:385, 1980.
- Miller SH, Lung RJ, Graham WP, et al: The acute effects of tourniquet ischemia on tissue and blood gas tensions in the primate limb, J Hand Surg 3:11, 1978.
- Miller SH, Price G, Buck D, et al: Effects of tourniquet ischemia and postischemic edema on muscle metabolism, J Hand Surg 4:547, 1979.
- Moore MR, Garfi n SR, Hargens AR: Wide tourniquets eliminate blood fl ow at low infl ation pressures, J Hand Surg 12A:1006, 1987.
- Neimkin RJ, Smith RJ: Double tourniquet with linked mercury manometers for hand surgery, J Hand Surg 8A:938, 1983.
- Ogufere WE, Giddins GE, Thom JS: Upper arm tourniquet pain in local anaesthetic surgery, J Hand Surg 20B:413, 1995.
- Patterson S, Klenerman L: The effect of pneumatic tourniquets on the ultrastructure of skeletal muscle, J Bone Joint Surg 61B:178, 1979.
- Pedowitz RA, Gershuni DH, Schindt AH, et al: Muscle injury induced beneath and distal to a pneumatic tourniquet: a quantitative animal study of effects of tourniquet pressure and duration, J Hand Surg 16A:610, 1991.
- Reid HS, Camp RA, Jacob WH: Tourniquet hemostasis: a clinical study, Clin Orthop Relat Res 177:230, 1983.
- Rorabeck CH: Tourniquet-induced nerve ischemia: an experimental investigation, J Trauma 20:280, 1980.
- Tountas CP, Bergman RA: Tourniquet ischemia: ultrastructural and histochemical observations of ischemic human muscle and of monkey muscle and nerve, J Hand Surg 2A:31, 1977.
- Tzarnas CD: Carpal tunnel release without a tourniquet, J Hand Surg 18A:1041, 1993.
- Wilgis EFS: Observations on the effects of tourniquet ischemia, J Bone Joint Surg 53A:1343, 1971.
- Splinting Benaglia PG, Sartorio F, Franchignoni F: A new thermoplastic splint for proximal interphalangeal joint fl exion contractures, J Sports Med Phys Fitness 39:249, 1999.
- Fess EE, McCollum M: The infl uence of splinting on healing tissues, J Hand Ther 11:157, 1998.
- Fess RE, Philips C: Hand splinting: principles and methods, 2nd ed, St Louis, 1986, Mosby. Ip WY, Chow SP: Results of dynamic splintage following
You Might Also Like

