Surgical Management of Peroneal and Sciatic Nerve Injuries
Key Takeaway
The common peroneal nerve is highly susceptible to injury due to its superficial course around the fibular neck. This comprehensive guide details the surgical anatomy, clinical evaluation, and operative techniques for managing peroneal and sciatic nerve lesions. It covers indications for neurolysis, primary neurorrhaphy, and autogenous nerve grafting, alongside rigorous postoperative immobilization protocols to optimize functional recovery and mitigate footdrop.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of the neuroanatomy of the lower extremity is paramount for the orthopaedic surgeon, particularly when navigating the complex topography of the sciatic nerve and its distal arborizations: the common, superficial, and deep peroneal nerves.
The Sciatic Nerve Complex
The sciatic nerve is the largest nerve in the human body, originating from the ventral rami of L4, L5, S1, S2, and S3. It exits the pelvis through the greater sciatic foramen, typically emerging inferior to the piriformis muscle. The nerve is composed of two distinct trunks—the tibial and the common peroneal—enclosed within a common epineurial sheath.
Clinical Pearl: The common peroneal division of the sciatic nerve is uniquely vulnerable to injury, even when it is still bundled within the proximal sciatic nerve sheath in the gluteal region or posterior thigh. This susceptibility is attributed to its lateral position, larger fascicles with less protective connective tissue, and its relatively tethered course.
The Common Peroneal Nerve
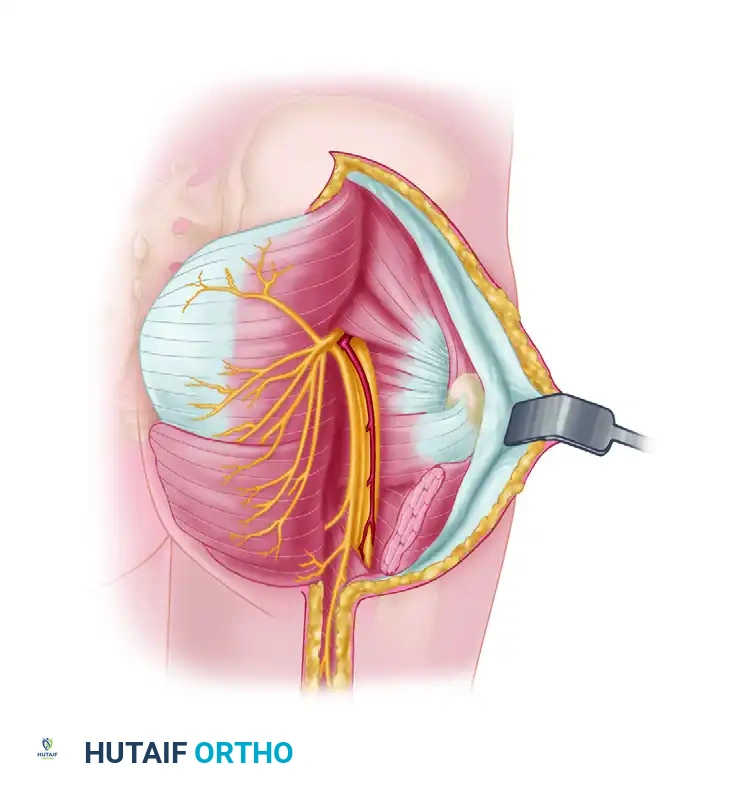
Near the proximal angle of the popliteal fossa, the sciatic nerve bifurcates. The common peroneal nerve (composed of fibers from L4, L5, S1, and S2) is significantly smaller than the tibial nerve. It deviates laterally within the popliteal fossa, tracking along the medial border of the biceps femoris tendon. It then arches around the posterior aspect of the fibular head and tightly encircles the fibular neck before piercing the peroneus longus muscle.
The common peroneal nerve itself is relatively short and possesses no direct motor branches. It provides two critical sensory branches:
* Lateral Sural Cutaneous Nerve: Supplies sensation to the skin along the lateral aspect of the knee and the proximal third of the calf.
* Peroneal Anastomotic Branch: Joins the tibial anastomotic branch to form the sural nerve, which provides sensory innervation to the posterolateral calf, lateral malleolus, lateral aspect of the foot, and the fourth and fifth toes.
The Superficial and Deep Peroneal Nerves
At or just inferior to the fibular neck, the common peroneal nerve divides into its two major terminal branches.

Superficial Peroneal Nerve:
This nerve courses distally in the lateral compartment of the leg, situated between the peroneus longus and extensor digitorum longus muscles, adjacent to the intermuscular septum.
* Motor Innervation: It provides motor branches to the peroneus longus and peroneus brevis muscles, governing foot eversion.
* Sensory Innervation: In the distal third of the leg, it pierces the deep crural fascia, dividing into two cutaneous branches (medial and intermediate dorsal cutaneous nerves). These supply the skin on the anterior and lateral aspects of the leg and the vast majority of the dorsum of the foot, excluding the first web space.
Deep Peroneal Nerve:
The deep peroneal nerve dives into the anterior compartment, passing obliquely and distally along the interosseous membrane, deep to the extensor digitorum longus and alongside the anterior tibial artery.
* Motor Innervation: It supplies the primary dorsiflexors of the foot and ankle: the tibialis anterior, extensor digitorum longus, extensor hallucis longus, peroneus tertius, extensor digitorum brevis, and the first dorsal interosseous.
* Sensory Innervation: Its terminal branch divides into dorsal digital cutaneous nerves that supply the highly specific wedge-shaped area of the first web space (between the great and second toes).
MECHANISMS OF INJURY AND PATHOANATOMY
The common peroneal nerve is injured far more frequently than the tibial nerve. Its superficial and tethered course around the unyielding fibular neck makes it highly susceptible to both direct trauma and indirect traction.
Traumatic and Iatrogenic Causes
- Knee Trauma: High-energy trauma around the knee, including multiligamentous knee injuries (particularly ruptures of the fibular collateral ligament and posterolateral corner), knee dislocations, and fractures or dislocations of the fibular head.
- Compression Neuropathy: Iatrogenic compression from improperly padded casts, tight surgical positioning, or even habitual leg crossing can induce ischemic neuropraxia or axonotmesis.
- Entrapment Syndromes: Bony entrapment of the superficial peroneal nerve can occur following fibular fractures. Additionally, entrapment by the margins of a deep fascial defect during strenuous exercise (exertional compartment syndrome or fascial herniation) is a well-documented cause of dynamic compression.
Surgical Warning: Release of compressing structures (neurolysis and fasciotomy) usually relieves painful symptoms and restores function if performed before irreversible Wallerian degeneration occurs. Delayed intervention significantly worsens the prognosis.
CLINICAL EVALUATION AND DIAGNOSIS
Motor and Sensory Examination
The hallmark of a high peroneal nerve lesion is footdrop, characterized by an inability to dorsiflex the ankle or extend the toes. This deficit cannot be overcome or disguised by any supplementary or "trick" movements, leading to a compensatory high-stepping (steppage) gait to prevent the toes from dragging. Eversion of the foot will also be weak or absent due to superficial peroneal nerve involvement.
Sensory examination must be meticulous. While the superficial peroneal nerve supplies a broad area over the dorsum of the foot, the deep peroneal nerve's sensory territory is restricted. Testing the autonomous zone is critical for localizing the lesion.

Clinical Pearl: The autonomous zone of the deep peroneal nerve (the first dorsal web space) varies in extent but is highly specific. Complete anesthesia in this web space, combined with footdrop, strongly indicates a lesion proximal to the bifurcation or a combined anterior compartment injury. The nerve may also be easily stimulated in situ at the head of the fibula to assess distal conduction.
SURGICAL INDICATIONS AND DECISION MAKING
Surgical exploration is indicated for open injuries with suspected nerve transection, closed injuries that fail to show clinical or electromyographic (EMG) improvement after 3 to 6 months, or cases of progressive compression neuropathy.
The Role of Bone Shortening vs. Nerve Grafting
Historically, in cases of massive sciatic or peroneal nerve defects, extensive mobilization and even bone shortening were considered to achieve a tension-free primary repair.
* Concomitant Fractures: If a femoral fracture is already present, judicious shortening of the femur during fracture fixation may be justified to help close a sciatic nerve gap.
* Intact Bone: In the absence of a fracture, the femur or tibia should not be shortened solely to facilitate nerve repair.
* Modern Paradigm: Autogenous interfascicular nerve grafting (typically utilizing the sural nerve) is the standard of care and a highly reasonable alternative, especially in young patients with robust regenerative capacity.
OPERATIVE TECHNIQUES
Approach to the Sciatic and Peroneal Nerves
- Positioning: The patient is placed in the prone position. The entire affected lower extremity, from the iliac crest to the toes, is prepped and draped free to allow for intraoperative manipulation of the hip and knee joints.
- Incision: For the common peroneal nerve, a curvilinear incision is made starting posterior to the biceps femoris tendon, extending distally across the fibular neck, and curving anteriorly over the lateral compartment.
- Dissection: The deep fascia is incised. The common peroneal nerve is identified proximally in the popliteal fossa where it is surrounded by fat. It is traced distally using vessel loops for gentle retraction.
- Decompression: The fibrous arch of the peroneus longus is divided to decompress the nerve as it winds around the fibular neck.
Neurolysis and Neurorrhaphy
- Neurolysis: If the nerve is in continuity but encased in scar tissue, an external neurolysis is performed under loupe or microscopic magnification. The epineurium is freed from surrounding adhesions.
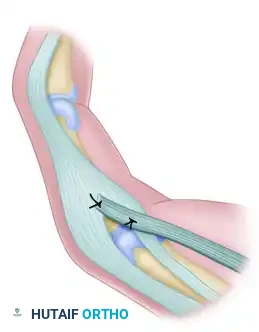
- Primary Repair: If the nerve is transected, the neuromatous ends are resected back to healthy, bleeding fascicles. If the gap is small (< 2 cm) and can be closed without tension (with the knee flexed), a primary epineurial repair is performed using 8-0 or 9-0 non-absorbable monofilament sutures.
- Interfascicular Grafting: For larger gaps, sural nerve cables are harvested. The grafts are reversed to prevent axonal loss down sensory branches and are sutured between the proximal and distal fascicular groups using microsurgical techniques. Fibrin glue may be used to augment the repair.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative immobilization strategy is critical to protect the neurorrhaphy from catastrophic tension, particularly in sciatic nerve repairs.
Immobilization Strategy for Sciatic Nerve Repair
After any primary neurorrhaphy of the sciatic nerve, tension must be absolutely minimized.
* Double Spica Cast: The limb should be immobilized in a double spica cast extending from the nipple line to the toes on the affected side, and to above the knee on the contralateral side.
* Positioning: On the affected side, the knee is flexed and the hip is extended to introduce maximum slack into the sciatic nerve complex.
* Wound Care: The cast is windowed over the surgical site to allow for the removal of sutures at approximately 10 to 14 days postoperatively.
Rehabilitation Timeline
- 0 to 6 Weeks: The patient remains in the spica cast.
- 6 Weeks: The cast is removed. A long-leg brace with an adjustable knee hinge is applied. The knee is extended gradually (e.g., 10 to 15 degrees per week) over the next 6 weeks to slowly stretch the regenerating nerve without causing traction injury.
- Physical Therapy: Aggressive physical therapy is initiated to restore passive and active range of motion to the joints and prevent soft tissue contractures.
- Orthotic Support: Once extension of the knee is complete, an appropriate brace (such as an Ankle-Foot Orthosis, AFO) is applied to compensate for the paralysis of the leg (footdrop) while awaiting nerve regeneration.
Surgical Pearl - Grafting Exception: When autogenous grafting has been used to repair the sciatic or peroneal nerve, the repair is inherently tension-free. While a spica cast or rigid splint is still necessary to protect the surgical site, maintaining the hip and knee in extreme, awkward positions is usually unnecessary. Furthermore, the cast can be removed earlier (when sutures are removed), and gentle, protected motion of the joints can be initiated sooner.
OUTCOMES AND PROGNOSIS
The prognosis following nerve repair in the lower extremity depends heavily on the level of the lesion, the age of the patient, and the mechanism of injury.
Results of Sciatic Nerve Suture
According to Sunderland's extensive observations, the overall functional results of primary suture of the sciatic nerve are historically poor, particularly in distally innervated muscles (such as those controlling the foot and ankle). This is due to several compounding factors:
1. Retrograde Neuronal Degeneration: Severe proximal cell body death following high lesions.
2. Intraneural Intermixing: As regenerating fibers cross the repair site, motor and sensory axons frequently misdirect into incorrect fascicular tubes, leading to a loss of precise fiber localization.
3. Target Organ Atrophy: Degenerative changes occur in the distal muscles (e.g., tibialis anterior) because they must remain denervated for a prolonged period while the axons regenerate down the length of the thigh and leg (at a rate of approximately 1 mm per day).
Usually, significant and functional motor recovery can only be expected in the proximally innervated muscles, especially the hamstring and proximal calf muscles. If sensation returns to the foot, it is usually only of a protective nature, though this is highly valuable for preventing neuropathic ulceration.
In contemporary series, such as those reported by Delaria et al., surgical intervention remains critical. In their cohort of 22 sciatic lesions treated surgically, 13 required neurolysis only (yielding the best functional outcomes), whereas the remainder required complex reconstruction. Ultimately, early diagnosis, meticulous microsurgical technique, and rigorous postoperative bracing remain the cornerstones of managing these challenging orthopaedic injuries.
You Might Also Like