Surgical Reconstruction of Combined High Median-Ulnar Nerve Palsy and Tetraplegia
Key Takeaway
The surgical reconstruction of the upper extremity in combined high median and ulnar nerve palsy, as well as tetraplegia, requires meticulous planning. Treatment focuses on restoring key pinch, grip, and elbow extension using available radially innervated or proximally intact musculature. Successful outcomes depend on resolving joint contractures, managing spasticity, and adhering to strict biomechanical principles during tendon transfers, tenodeses, and arthrodeses.
COMBINED HIGH MEDIAN AND ULNAR NERVE PALSY (ABOVE THE ELBOW)
The management of combined high median and ulnar nerve palsy represents one of the most formidable challenges in reconstructive hand surgery. In this devastating injury, the entire palmar surface of the hand is rendered anesthetic, with sensibility preserved only on the dorsal surface supplied by the superficial sensory branch of the radial nerve. Motor loss is profound: all intrinsic muscles of the hand, as well as the extrinsic flexors of the digits and wrist (excluding those innervated by the radial nerve), are paralyzed.
Consequently, the only motor units available for transfer are those innervated by the intact radial nerve. These include the brachioradialis (BR), extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), extensor carpi ulnaris (ECU), and extensor indicis proprius (EIP).
Preoperative Prerequisites and Soft Tissue Management
For any tendon transfer to be successful, the fundamental prerequisites of reconstructive surgery must be met. Tendon transfers cannot overcome fixed joint contractures.
Surgical Warning: Any contracture of the skin, web spaces, or joints must be corrected prior to, or concurrent with, tendon transfer surgery. Passive extension of the interphalangeal (IP) joints and passive flexion of the metacarpophalangeal (MCP) joints must be fully achievable.
If dynamic splinting fails to mobilize stiff joints, surgical release or arthrodesis (particularly of the proximal interphalangeal joints) must be considered. Furthermore, thumb web space contractures—a frequent sequela of combined median and ulnar nerve palsy due to unopposed extensor pull—must be released to allow for functional thumb opposition and adduction.
Comprehensive Surgical Reconstruction Strategy
The recommended surgical reconstruction for combined high median and ulnar nerve palsy is a multi-stage or extensive single-stage procedure designed to restore basic grasp and key pinch. The standard protocol includes the following components:
- Thumb Metacarpophalangeal Joint Arthrodesis: Stabilizing the thumb MCP joint is critical to prevent hyperextension during pinch, directing all transferred motor force to the interphalangeal and carpometacarpal joints.
- Zancolli Capsulodesis and Flexor Sheath Release: To prevent clawing and allow the extrinsic radial nerve-innervated extensors to extend the IP joints, a Zancolli volar capsulodesis of the MCP joints of all four fingers is performed. This is often combined with the release of the flexor tendon sheaths to optimize the excursion of the transferred tendons.
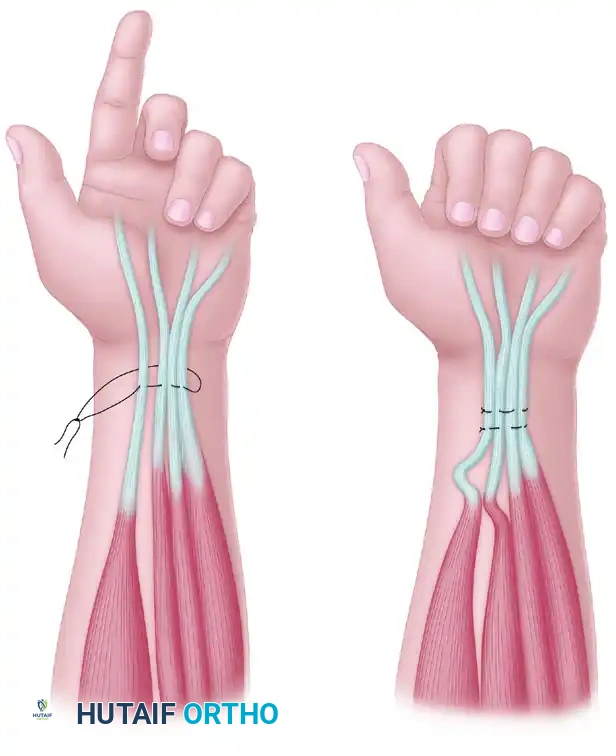
- Restoration of Finger Flexion (ECRL to FDP): The ECRL is detached from its insertion on the base of the second metacarpal, mobilized proximally, and routed around the radial border of the forearm. It is then woven into the flexor digitorum profundus (FDP) tendons.
Surgical Technique Pearl: In high median nerve palsy, the distal segments of the profundus tendons of the index and middle fingers are tightened, and the tendons are sutured to the intact profundus tendons of the ring and little fingers. This unified tendon mass is then strengthened further by the transfer of the ECRL to insert as an additional motor unit.
- Restoration of Thumb Flexion (BR to FPL): The brachioradialis is an excellent motor for the flexor pollicis longus (FPL) due to its strength and excursion. The BR must be mobilized extensively, freeing it from its fascial attachments up to the elbow to ensure adequate excursion (typically 30 mm is required).
- Restoration of Thumb Opposition/Adduction (ECU to EPB): The extensor carpi ulnaris is detached, prolonged with a free tendon graft (such as the palmaris longus or plantaris), and routed around the ulnar border of the forearm to insert into the extensor pollicis brevis (EPB) or the base of the proximal phalanx of the thumb.
Clinical Pearl: In extreme cases where local tissue conditions are poor or multiple transfers fail, amputating the index finger and its metacarpal, and folding the radially innervated dorsal skin flap into the palm, has been suggested as a salvage procedure to provide a sensate gripping surface.
SEVERE PARALYSIS FROM CERVICAL SPINAL CORD DAMAGE (TETRAPLEGIA)
Improved acute management and advanced long-term care for victims of motor vehicle accidents, falls, and sports injuries have dramatically increased the life expectancy of patients with tetraplegia. Consequently, there is a profound emphasis on the surgical rehabilitation of the upper extremities.
Most survivors of cervical spinal cord injuries are young males with decades of life remaining. Nearly two-thirds of these patients retain C6 root level function. Subjectively, the restoration of hand and upper extremity function is consistently ranked by tetraplegic patients as their highest priority—often prioritized above the restoration of lower extremity, bowel, bladder, or sexual function.
International Classification for Surgery of the Hand in Tetraplegia
To standardize treatment and facilitate outcome comparisons, the International Classification for Surgery of the Hand in Tetraplegia (Edinburgh 1978, modified in Giens 1984) is utilized. This system evaluates both sensory afferent and motor efferent status.
Sensory Classification:
* O (Ocular): The patient lacks functional cutaneous sensibility (greater than 10-mm two-point discrimination) and must rely entirely on visual feedback to control the hand.
* Cu (Cutaneous): The patient retains at least 10-mm two-point discrimination in the thumb and index finger, allowing for proprioceptive and tactile feedback during grip.
Motor Classification (Groups 0-9):
The motor grouping is determined by the lowest level of muscle function grading at Medical Research Council (MRC) Grade 4 or better.
* Group 0: No muscle below the elbow suitable for transfer.
* Group 1: Brachioradialis (BR) available.
* Group 2: Extensor carpi radialis longus (ECRL) available.
* Group 3: Extensor carpi radialis brevis (ECRB) available. (Note: It is clinically difficult to separate ECRL and ECRB strength without surgical exposure).
* Group 4: Pronator teres (PT) available.
* Group 5: Flexor carpi radialis (FCR) available.
* Group 6: Finger extensors available.
* Group 7: Thumb extensor available.
* Group 8: Partial digital flexors available.
* Group 9: Lacks only intrinsic hand function.
* Group X: Exceptions (asymmetrical or skip lesions).
Principles of Management and Patient Selection
Careful analysis of the motor and sensory status is paramount. Cervical spine injuries at the same vertebral level can yield vastly different physical findings due to skip lesions or asymmetrical cord damage.
Pitfall: Many patients are extremely hesitant to undergo surgery for fear of losing their remaining, hard-earned function. The surgeon must observe the patient performing activities of daily living (ADLs) to determine precisely which functional upgrade will yield the greatest independence.
Core Principles (McDowell, Moberg, and House):
1. Timing: Neurological recovery must have completely plateaued. A minimum of 12 months should elapse post-injury before any reconstructive surgery is undertaken.
2. Spasticity: Uncontrolled spasticity in a potential donor muscle, regardless of its MRC grade, strictly precludes its use in a tendon transfer.
3. Pain: Severe, painful paresthesias in a hand prohibit reconstructive surgery on that extremity.
4. Tenodesis Effect: Wrist mobility and the natural tenodesis effect (finger flexion upon wrist extension) must be meticulously preserved, as this is often the patient's primary method of grasping.
If cutaneous sensibility (Cu) is absent and the patient relies on ocular (O) feedback, reconstructive surgery should be limited to only one upper extremity. Operating on both hands in an "Ocular" patient splits their visual attention, rendering bilateral reconstructed hands functionally useless simultaneously.
Phased Protocol for the Management of Tetraplegia
Murphy and Chuinard developed a highly effective, phased protocol for managing the upper extremity in tetraplegia:
1. Acute Phase:
* Stabilize the cervical spine to preserve remaining neurological function.
* Aggressively manage associated upper extremity trauma.
* Institute immediate occupational therapy to prevent joint contractures and maintain passive mobility.
2. Subacute Phase:
* Begin aggressive systemic rehabilitation.
* Manage associated complications (decubitus ulcers, autonomic dysreflexia, bladder care).
* Perform serial neurological examinations at 3-month intervals to track recovery plateaus.
3. Reconstructive Phase:
* Ensure the patient is psychologically adjusted and at least 12 months post-injury.
* Begin reconstruction on the side with the most intact function. If equal, begin on the dominant extremity.
* Keep the surgical plan simple. The goal is key pinch and basic grasp, not complex independent finger dexterity.
* Priority: Restoration of active elbow extension (Moberg deltoid-to-triceps) must precede hand reconstruction.
SPECIFIC SURGICAL RECONSTRUCTIONS IN TETRAPLEGIA
Restoration of Elbow Extension
Elbow extension is lost in approximately 70% of tetraplegic patients. Without active elbow extension, the patient cannot reach objects above their head, push a manual wheelchair efficiently, or perform pressure relief lifts to prevent ischial decubitus ulcers. Regaining elbow extension is the absolute first priority in upper extremity reconstruction.
Posterior Deltoid-to-Triceps Transfer (Moberg Procedure):
This is the gold standard for restoring elbow extension. The posterior third of the deltoid is mobilized and transferred to the triceps aponeurosis. Because the deltoid lacks sufficient length to reach the olecranon directly, an intercalated tendon graft is required. While toe extensors were historically used, modern techniques favor the use of the tibialis anterior tendon or fascia lata grafts for superior strength.
* Postoperative Care: The elbow is immobilized in extension for 4 to 6 weeks, followed by a graduated hinged brace to slowly regain flexion while protecting the transfer.
Biceps-to-Triceps Transfer (Friedenberg and Zancolli):
This transfer routes the biceps tendon posteriorly to the terminal insertion of the triceps.
* Indication: This can only be performed if the supinator muscle is fully active and strong enough to independently supinate the forearm against resistance. If the supinator is weak, transferring the biceps will result in a devastating loss of forearm supination.
Restoration of Forearm Pronation
Patients in Group 3 or lower typically lack active forearm pronation. This results in a fixed or dynamic supination deformity, driven by the intact biceps, which prevents the hand from being positioned functionally over a keyboard, table, or wheelchair rim.
Biceps Rerouting (Zancolli Procedure):
To correct this, the biceps tendon is detached from the radial tuberosity, rerouted around the lateral aspect of the proximal radius, and reattached. This biomechanically converts the biceps from a primary supinator into a pronator. If the interosseous membrane is severely contracted, it must be surgically released concurrently to allow for full pronation.
Restoration of Wrist Extension
Active wrist extension is the cornerstone of the tetraplegic hand, as it drives the tenodesis grasp. In Group 1 patients, the only available motor is the brachioradialis.
Brachioradialis to Extensor Carpi Radialis Brevis (BR to ECRB):
The BR is transferred to the ECRB to restore strong, central wrist extension.
* Biomechanical Rationale: The transfer must be routed to the ECRB rather than the ECRL. Transferring to the ECRL produces excessive radial deviation during extension, which weakens the tenodesis effect and destabilizes the radiocarpal joint over time. Transfer into the ECU is contraindicated, as the ECU acts as a wrist extensor only when the forearm is fully supinated; in pronation, it acts primarily as an ulnar deviator.
Restoration of Key Pinch and Grip
For most tetraplegic patients, the ultimate surgical objective is to obtain a strong "key pinch" (lateral pinch between the thumb pulp and the radial aspect of the index finger middle phalanx). Key pinch provides a broader, stronger gripping surface and is biomechanically easier to achieve than a three-jaw chuck pinch.
Moberg Key Pinch Procedure:
In lower-level tetraplegia (Groups 1 and 2), active motors for finger flexion are absent. The Moberg procedure relies on tenodesis.
1. FPL Tenodesis: The flexor pollicis longus is sectioned proximally and anchored securely to the distal radius. As the patient actively extends the wrist (using the BR to ECRB transfer), the tethered FPL passively pulls the thumb into flexion against the index finger.
2. Thumb CMC Arthrodesis: To ensure the thumb does not collapse into retropulsion during pinch, the carpometacarpal joint is often pinned or arthrodesed in a functional position of slight palmar abduction.
3. EPL Rerouting: The extensor pollicis longus can be rerouted volar to the wrist axis to act as an additional tenodesis tether, aiding in thumb opening when the wrist is flexed.
Advanced Considerations: Functional Electrical Stimulation (FES)
In high-level tetraplegia (Group 0) where no expendable motor units are available for transfer, implanted electrical stimulation systems represent the frontier of rehabilitation. Intact lower motor neuron units that simply lack cortical efferent control can be stimulated by micro-electrodes directed along intact neural pathways. By programming combinations of stimuli to different neuromuscular units, concerted activities such as grasp and release can be artificially synthesized, offering profound improvements in quality of life for the most severely paralyzed patients.
You Might Also Like

