Mastering Surgical Approaches to the Radial and Ulnar Nerves
Key Takeaway
Mastering the surgical approaches to the radial and ulnar nerves requires profound anatomical knowledge and meticulous technique. This guide provides an evidence-based, step-by-step framework for exposing the radial nerve from the axilla to the posterior interosseous branch, alongside comprehensive protocols for managing ulnar nerve pathology. Key principles include strategic mobilization, interfascicular grafting for defect closure, and precise clinical evaluation to optimize postoperative motor and sensory recovery in complex peripheral nerve injuries.
SURGICAL ANATOMY AND BIOMECHANICS OF THE RADIAL NERVE
The radial nerve, the largest terminal branch of the posterior cord of the brachial plexus (C5-T1), is highly susceptible to injury due to its intimate relationship with the humeral shaft. Its anatomical course dictates the surgical approach required for exploration, neurolysis, or repair. Originating in the axilla, it courses posterior to the brachial artery, passing anterior to the tendons of the latissimus dorsi and teres major. It then enters the spiral groove (radial sulcus) of the humerus, descending obliquely between the lateral and medial heads of the triceps brachii.
Biomechanically, the radial nerve undergoes significant excursion during elbow flexion and extension. Tethering at the lateral intermuscular septum—where it pierces the septum to enter the anterior compartment of the arm—makes it particularly vulnerable to traction injuries and entrapment, especially in the context of Holstein-Lewis fractures (distal third humeral shaft fractures).
Surgical Warning: The radial nerve is relatively fixed as it pierces the lateral intermuscular septum. Aggressive retraction during humeral plating or failure to adequately release the septum during nerve transposition can lead to devastating iatrogenic palsies.
INDICATIONS FOR SURGICAL INTERVENTION
Surgical exploration of the radial nerve is indicated in several clinical scenarios:
* Open Fractures: Immediate exploration is warranted for open humeral shaft fractures with an associated radial nerve deficit.
* Penetrating Trauma: Sharp lacerations or high-velocity missile wounds traversing the nerve's path.
* Secondary Palsy: A radial nerve palsy that develops after closed reduction of a humeral fracture strongly suggests nerve entrapment within the fracture site.
* Failure of Conservative Management: Lack of clinical or electromyographic (EMG) recovery 3 to 4 months following a closed injury.
* Compressive Neuropathies: Radial tunnel syndrome or posterior interosseous nerve (PIN) entrapment at the arcade of Frohse.
APPROACH TO THE RADIAL NERVE: STEP-BY-STEP TECHNIQUE
Exposure in the Axilla and Proximal Third of the Arm
To expose the radial nerve in the axilla and the proximal third of the arm, utilize the standard extensile incision for the distal brachial plexus.
- Incision: Begin at the coracoid process, extending distally along the deltopectoral groove, and curve into the medial bicipital groove. Carry this incision distally in the arm, positioning it slightly more posteriorly than is necessary for exposing the ulnar and median nerves.
- Fascial Dissection: Incise the deep brachial fascia over the neurovascular bundle.
- Nerve Identification: Expose the neurovascular bundle between the triceps posteriorly and the biceps, brachialis, and coracobrachialis anteriorly. Expose and retract the more superficial structures laterally—specifically the ulnar nerve, the brachial artery and vein, and the median nerve.
- Tracing the Nerve: Deep to these structures, identify the radial nerve. Carefully isolate it and trace its proximal branches, first to the long head and then to the medial head of the triceps. Trace the nerve distally to the point where it winds around the posterior aspect of the humerus into the spiral groove.
Exposure in the Middle and Distal Thirds of the Arm
For lesions involving the mid-to-distal humeral shaft, a posterior or lateral approach is required.
Figure 62-27 A: The skin incision begins at the posterior margin of the deltoid muscle and extends distally in the midline, curving laterally and anteriorly to end at the interval between the brachioradialis and brachialis.
- Incision: To expose the nerve on the posterior and lateral aspects of the humeral shaft, begin the incision along the posterior border of the distal third of the deltoid, between the deltoid and the long head of the triceps. Curve it distalward along the lateral aspect of the arm.
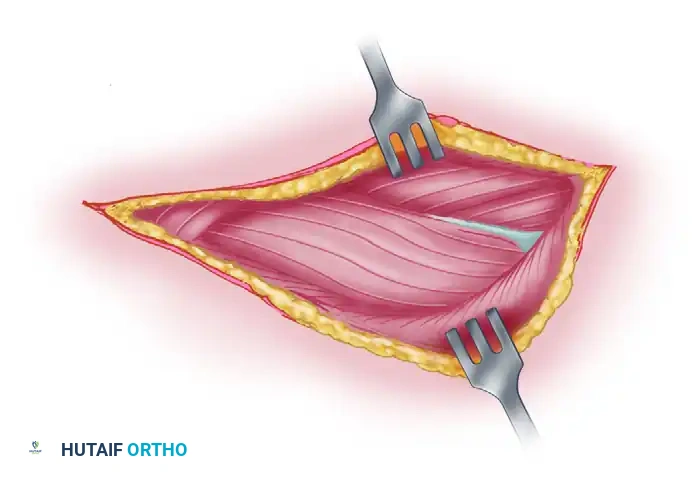
Figure 62-27 B: The posterior skin flap is dissected and retracted. The deep fascia is incised in line with the skin incision. The dotted line indicates the planned incision in the triceps muscle between the long and lateral heads.
- Triceps Interval: Develop the interval between the long and lateral heads of the triceps.
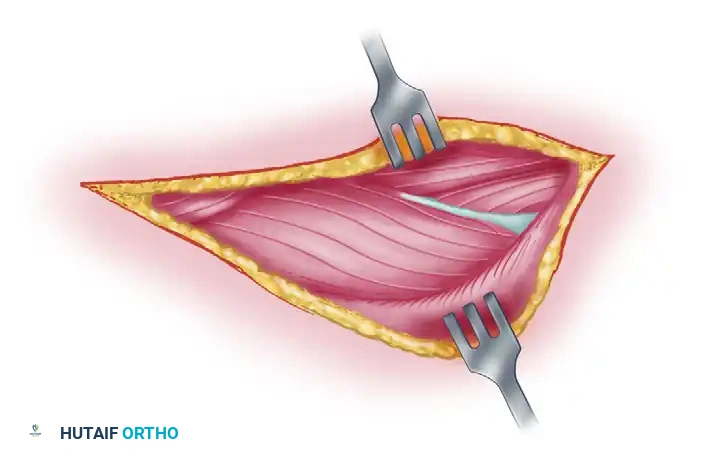
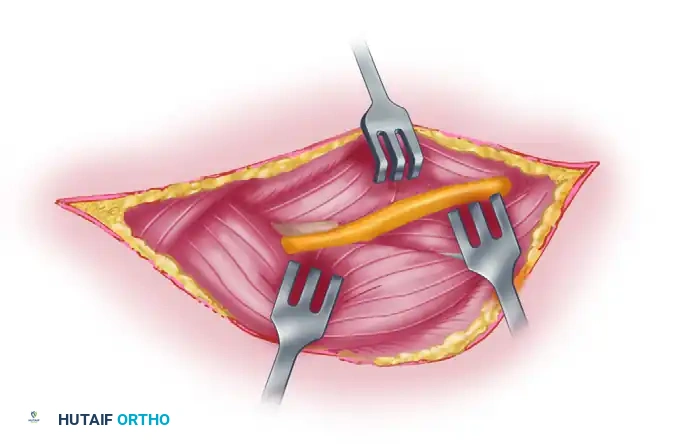
Figure 62-27 C: The radial nerve and accompanying profunda brachii vascular bundle are exposed by retracting the two heads of the triceps muscle. The nerve is dissected to the point where it passes beneath the lateral head of the triceps.
- Anterolateral Dissection: Curve the incision anteriorly along the medial aspect of the brachioradialis. If necessary, extend it laterally at the elbow across the belly of this muscle and the extensor carpi radialis longus (ECRL).
Figure 62-27 D: The arm is externally rotated. The interval between the proximal end of the brachioradialis and brachialis is dissected, exposing the radial nerve along the anterolateral aspect of the humerus.
- Superficial Identification: In the incision proximal to the elbow, expose the nerve at its most superficial position by incising the fascia between the brachialis and brachioradialis. Identify the nerve by retracting the brachioradialis laterally.
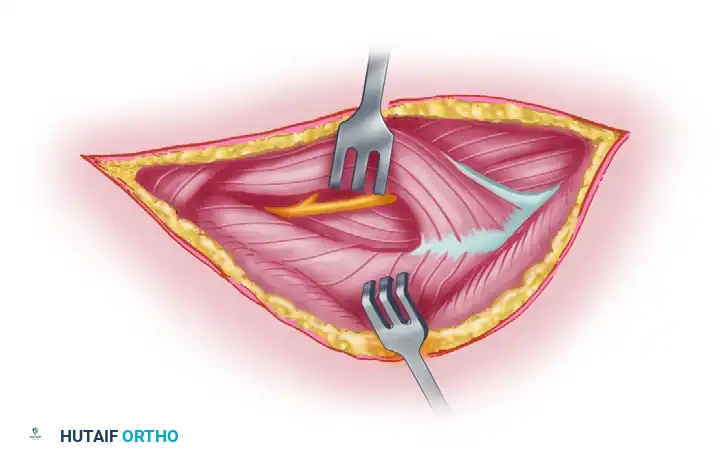
Figure 62-27 E: The dotted line indicates the incision through which the lateral head of the triceps is mobilized from the underlying bone, facilitating exposure of the radial nerve deep to it.
- Deep Exposure: The nerve can be exposed proximally by incising the fascia and retracting the lateral head of the triceps laterally to the point where the nerve winds around the humerus.
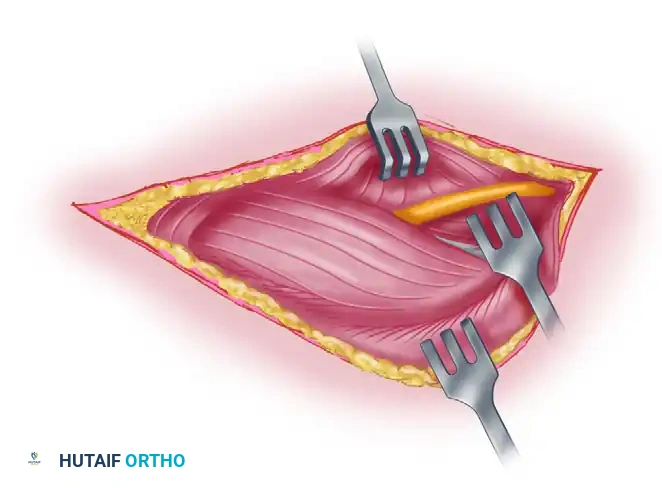
Figure 62-27 F: Final exposure of the radial nerve following mobilization of the lateral triceps head.
Exposure of the Posterior Interosseous Nerve (PIN)
At the elbow, the radial nerve divides into the superficial radial nerve (entirely sensory, which must be protected to avoid painful neuromas) and the deep radial nerve (posterior interosseous nerve), which is frequently injured and highly disabling.

Figure 62-28 A: Line of incision for PIN exposure. The forearm is prone, and the elbow is flexed.
- Distal Extension: If the deep radial nerve is to be explored, carry the incision distally on the dorsum of the forearm along the radial side of the extensor digitorum communis. Begin 8 to 10 cm proximal to the elbow and continue to the middle of the dorsum of the forearm.
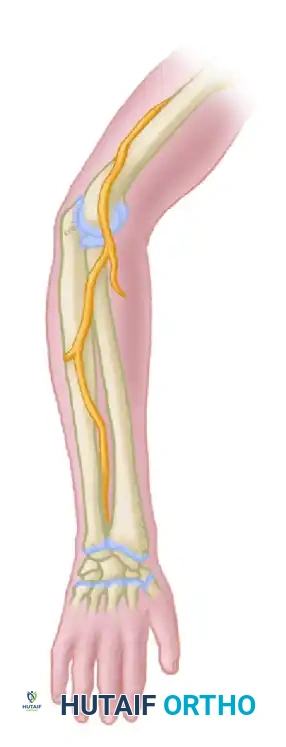
Figure 62-28 B: The posterior interosseous nerve is exposed as it enters the supinator muscle.
- Supinator Dissection: Follow the nerve beneath the brachioradialis into the supinator muscle. If the injury is at this point or more distal, expose the nerve distal to the supinator by incising the fascia between the ECRL/ECRB and the extensor digitorum communis, developing this plane of cleavage.

Figure 62-28 C: Diagrammatic representation of the course of the radial nerve and its bifurcation into the superficial sensory branch and the posterior interosseous nerve.
- Arcade of Frohse: Follow the nerve proximally to the distal border of the supinator where numerous branches are given off. After identifying these branches, incise the superficial part of the supinator at a right angle to the direction of its fibers to complete the exposure of the entire deep radial nerve.
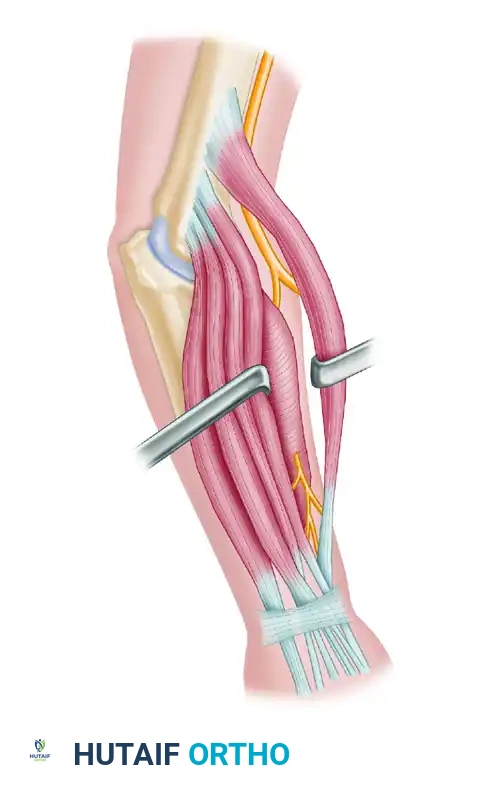
Figure 62-28 D: Alternative line of incision with the elbow extended.
METHODS OF CLOSING GAPS IN THE RADIAL NERVE
Interfascicular nerve grafting is the gold standard and preferred method for bridging gaps, although extensive mobilization techniques remain relevant for smaller defects.
- Proximal Defects: In the axilla and proximal arm, closing a gap of more than 6 to 7 cm is exceedingly difficult without sacrificing the motor branches to the triceps—a maneuver that is rarely justifiable. Resecting the humerus to gain length is almost never feasible at this level.
- Mid-Arm Defects: In the middle third of the arm, defects of 10 to 12 cm can occasionally be closed by aggressive mobilization. This involves mobilizing the nerve from the elbow to the clavicle, widely stripping the branches, flexing the elbow, and externally rotating and strongly adducting the arm across the chest. If necessary, the branch to the brachioradialis may be sacrificed (provided the biceps is functioning).
- Anterior Transposition: Transposing the nerve beneath the biceps anterior to the humerus adds variable length and is occasionally worthwhile.
- Bone Resection: In the presence of a nonunited fracture of the humerus, 3 to 4 cm of the bone can be resected. However, resecting part of a normal humerus should almost never be necessary.
Clinical Pearl: Before extreme dissection, awkward postoperative positioning, or bone shortening is attempted, serious consideration must be given to autologous interfascicular nerve grafting (e.g., using the sural nerve). Tension-free neurorrhaphy is paramount; excessive tension guarantees failure.
RESULTS OF SUTURE AND CRITICAL LIMITS OF DELAY
Only motor recovery is functionally critical in the suture of the radial nerve. The prognosis for radial nerve repair is generally the most favorable among major peripheral nerves because it primarily supplies large, proximal muscle groups rather than intrinsic hand muscles requiring fine motor control.
- Recovery Statistics: Among patients undergoing radial nerve neurorrhaphy, 89% obtain recovery of proximal muscles, 63% regain useful function of all muscles supplied by the radial nerve, and 36% regain some fine control of the extensors of the fingers and thumb. Under optimal conditions, more than 75% of patients recover useful function.
- Grafting Outcomes: Lee et al. reported good to excellent motor recovery in patients with high radial nerve palsy treated with 9 to 11 cm of interfascicular nerve grafting, recommending nerve reconstruction before resorting to tendon transfers.
- Primary Repair Warning: Primary repair of transected radial nerves associated with open humeral fractures is generally not recommended due to poor recovery rates associated with the zone of injury; delayed repair or grafting is preferred.
- Critical Limit of Delay: Return of motor function should not be expected when suture has been delayed for more than 15 months. For the posterior interosseous nerve, Zachary found that return of function is highly unlikely if the delay exceeds 9 months.
SURGICAL ANATOMY AND PATHOLOGY OF THE ULNAR NERVE
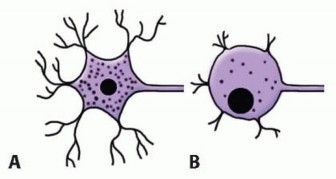
The ulnar nerve is composed of fibers from C8 and T1, originating from the medial cord of the brachial plexus. It is the primary motor nerve to the intrinsic muscles of the hand, making its preservation and repair critical for fine motor function and grip strength.
Mechanisms of Injury
The ulnar nerve may be divided at any point along its course by missile wounds or lacerations.
* Upper Arm: When injured in the upper arm, adjacent structures such as the median nerve or brachial artery are frequently compromised due to their anatomical proximity.
* Middle Arm: In the middle of the arm, the ulnar nerve is relatively protected by the medial intermuscular septum.
* Elbow and Distal Arm: At the elbow, it is highly susceptible to injury from elbow dislocations, supracondylar fractures, and condylar fractures. Deficits here may be caused by the initial trauma, repeated manipulations, or delayed scar formation.
* Wrist and Forearm: The nerve is injured most commonly in the distal forearm and wrist, predominantly by civilian lacerations (e.g., glass injuries).
Compressive Neuropathies and Tardy Ulnar Palsy
Tardy ulnar nerve palsy frequently develops after malunited fractures of the lateral humeral condyle in children (leading to cubitus valgus), displaced medial epicondyle fractures, or recurrent subluxation. In cubitus valgus, the ulnar nerve is gradually stretched and can become incompletely paralyzed.
Cubital Tunnel Syndrome: Coined by Feindel and Stratford in 1958, this describes compression neuropathy of the ulnar nerve around the elbow without antecedent trauma. The nerve is bordered by the medial epicondyle anteriorly, the elbow joint
Associated Surgical & Radiographic Imaging

You Might Also Like