Two-Stage Reconstruction for Digital Flexion and Key Pinch in Tetraplegia
Key Takeaway
The House two-stage reconstruction is a foundational surgical strategy for restoring digital flexion and key pinch in patients with cervical spinal cord injuries. Stage one establishes a stable extensor tenodesis, while stage two utilizes active tendon transfers—specifically the extensor carpi radialis longus to the flexor digitorum profundus, and the pronator teres to the flexor pollicis longus—to restore functional grasp and pinch biomechanics.
Introduction to Tetraplegic Hand Reconstruction
The restoration of hand function in patients with cervical spinal cord injuries (tetraplegia) represents one of the most profound interventions in reconstructive orthopedic surgery. For patients with mid-cervical lesions (typically C6 or C7), the preservation of wrist extension provides a critical biomechanical foundation for restoring grasp and pinch through the tenodesis effect.
The House two-stage reconstruction is an internationally recognized, highly structured surgical protocol designed to restore digital flexion and key pinch. By dividing the reconstruction into an "extensor phase" (Stage 1) and a "flexor phase" (Stage 2), the surgeon can precisely set the tension required for a functional tenodesis grasp without the conflicting forces that often compromise single-stage, multidirectional tendon transfers.
Clinical Pearl: The fundamental prerequisite for any tendon transfer in the tetraplegic hand is the presence of supple, contracture-free joints. Preoperative passive range of motion must be optimized through rigorous hand therapy before surgical intervention is considered.
Preoperative Evaluation and Biomechanical Principles
Patient Selection and Classification
Patient selection is guided by the International Classification for Surgery of the Hand in Tetraplegia (ICSHT). The House two-stage technique is primarily indicated for patients in ICSHT Groups 4 and 5, who possess strong brachioradialis (BR), extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), and pronator teres (PT) function, but lack active digital flexion and intrinsic muscle function.
The Tenodesis Effect
The entire reconstruction relies on the biomechanics of wrist-driven tenodesis. Active wrist extension must passively drive the digits into flexion (for grasp) and the thumb into adduction (for key pinch). Conversely, wrist flexion must passively extend the digits to allow for the release of objects. The two-stage approach ensures that the extensor tenodesis (release) is fully healed and stable before the flexor transfers (grasp) are introduced.
Stage 1: The Extensor Phase
The primary objective of the first stage is to establish a reliable mechanism for digital and thumb extension when the wrist is flexed, while simultaneously preventing metacarpophalangeal (MCP) joint hyperextension.
Surgical Approach and Extensor Tenodesis
The extensor digitorum communis (EDC) tendons are isolated and prepared for tenodesis to the distal radius.
- Tendon Routing: The EDC tendons are mobilized and routed to the dorsal radius.
- Tensioning: The EDC tendons are secured to the radius (often using suture anchors or transosseous tunnels) so that the MCP joints are held in full extension.
- Intraoperative Verification: A heavy nonabsorbable suture is woven into the tendon and delivered through the osseous fixation points. The surgeon must pull the sutures firmly and check the tenodesis effect: full MCP extension must be achieved when the wrist is passively flexed to 40 degrees. Crucially, full passive flexion of the fingers must still be obtainable when the wrist is extended to 40 degrees.
Thumb Extensor and Abductor Tenodesis
In a similar fashion, the abductor pollicis longus (APL) and extensor pollicis longus (EPL) tendons are rerouted and fixed to the radius.
* Tensioning Parameters: With 40 degrees of wrist flexion, the thumb interphalangeal (IP) joint must be extended to 0 degrees, and the thumb metacarpal must rest in the plane of the hand, radially abducted 30 to 40 degrees.
* After securing the tenodesis, the surgeon must verify that wrist extension allows acceptable passive thumb motion, preparing the thumb for the flexor phase.
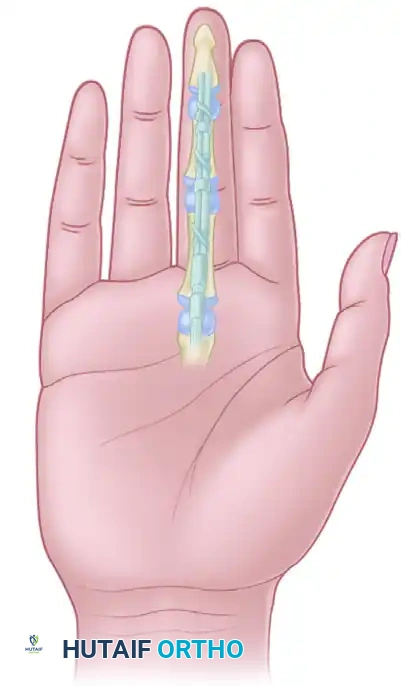
Intrinsic Tenodesis (House Modification)
To prevent the claw deformity (MCP hyperextension with IP flexion) inherent in intrinsic-minus hands, an intrinsic tenodesis is required. This can be achieved via transfer into the A2 pulley or the dorsal apparatus.
House et al. described a highly effective procedure utilizing a free tendon graft (often palmaris longus or a toe extensor).
* The graft is sutured into the central slip and lateral tendon of the extensor apparatus.
* It is then routed volarly through the lumbrical canals and passed around the dorsum of the metacarpal necks of the index and middle fingers.
* Biomechanics: This construct acts as an "oblique retinacular ligament." When the proximal interphalangeal (PIP) joint is flexed, it forces concomitant MCP flexion and acts as a robust checkrein against MCP hyperextension.
Postoperative Care for Stage 1
The wrist is immobilized in 40 to 45 degrees of extension. The thumb and MCP joints are held in 40 degrees of flexion, with the IP joints in full extension. This immobilization is maintained for exactly 4 weeks to allow the tenodesis to heal solidly, after which carefully guided active and passive motion is initiated. If a thumb carpometacarpal (CMC) joint arthrodesis was performed concurrently to stabilize the thumb ray, the thumb is protected until radiographic fusion is confirmed.
Stage 2: The Flexor Phase
The flexor phase is performed 2 to 6 months after the extensor phase, once the extensor tenodesis is stable and the patient has regained full, supple passive motion of the digits. The goal is to restore active digital flexion and thumb key pinch.
Surgical Approach and Tendon Harvest
Access to the ECRL and PT for transfer into the flexor digitorum profundus (FDP) and flexor pollicis longus (FPL) requires a meticulously planned three-incision approach.
- Volar Forearm Incision: Make a volar longitudinal incision extending from the proximal wrist flexion crease, just radial to the flexor carpi radialis (FCR) tendon, extending proximally to the midshaft of the radius.
- Tendon Isolation: Isolate the FPL, the PT, and the FDP tendons proximal to their musculotendinous junctions.
- ECRL Release: Make a short transverse incision over the base of the second metacarpal. Identify and divide the ECRL at its insertion.
- ECRL Retrieval: Withdraw the ECRL tendon proximally to the level of the APL tendon in the middle third of the forearm. This is often facilitated by utilizing the proximal limb of the incision from the Stage 1 reconstruction.
Surgical Warning: Do not inadvertently harvest the Extensor Carpi Radialis Brevis (ECRB). The ECRB is the primary, central wrist extensor. Sacrificing the ECRB will result in a devastating loss of wrist extension power and a severe radial deviation deformity. Always verify tendon insertion before division.
Surgical Technique 71-23: Tendon Transfers and Weaving
The core of the flexor phase involves transferring the ECRL to the FDP (for finger flexion) and the PT to the FPL (for thumb flexion/pinch).
- Preparation of the ECRL: Free the ECRL tendon from its surrounding fascial attachments proximally into the forearm to ensure maximum, unimpeded excursion.
- Harvest of the Pronator Teres: Detach the PT tendon from its insertion on the midshaft of the radius.
- Technical Pearl: Harvest the PT with a generous strip of its periosteal attachment. This extra length is critical for achieving a secure Pulvertaft weave into the FPL without excessive tension.
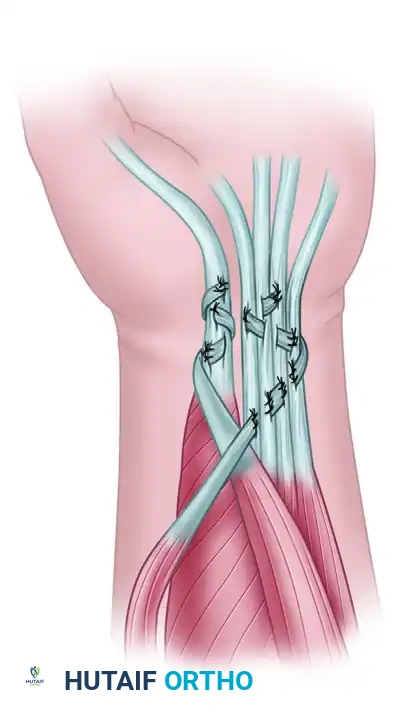
- The Tendon Weave: Perform a classic Pulvertaft weave. Weave the PT into the FPL, and the ECRL into the FDP mass.
Figure 71-41: House two-stage technique for reconstruction of digital flexion and key pinch—stage 2 (flexor phase). The Extensor carpi radialis longus is transferred to the flexor digitorum profundus, and the pronator teres is transferred to the flexor pollicis longus.
The Art of Tensioning
Tensioning is the most unforgiving aspect of tetraplegic hand reconstruction. The transfers must be set with the tenodesis effect in mind.
- PT to FPL Tension: Adjust the tension so that the thumb pulp rests firmly against the radial side of the index finger (key pinch position) when the wrist is passively held in 30 degrees of extension.
- ECRL to FDP Tension: The tension should allow for a reasonable, synchronous cascade of finger flexion when the wrist is brought into 40 degrees of extension. When the wrist is flexed to neutral or slight flexion, the fingers must be able to extend fully via the Stage 1 tenodesis to allow for object release.
Opponensplasty and Adductorplasty (Optional but Recommended)
If the brachioradialis (BR) was not utilized during the extensor phase, it serves as an excellent motor for an opponensplasty or adductorplasty to strengthen key pinch. This is essentially a modification of the Royle-Thompson transfer.
- FDS Harvest: Harvest the ring finger flexor digitorum sublimis (FDS) tendon, similar to the Zancolli lasso procedure. Bring the FDS tendon out through a small incision at the distal-ulnar margin of the transverse carpal ligament.
- Tendon Routing: Tunnel the FDS tendon, with its two slips, subcutaneously across the palm to the MCP region of the thumb.
- Distal Attachment: Suture one slip of the FDS into the EPL tendon distal to the MCP joint, and suture the other slip into the adductor pollicis tendon insertion.
- Proximal Motor Weave: Weave the free end of the mobilized BR tendon into the intact proximal portion of the ring FDS.
- Tensioning the Opponensplasty: Set the tension so that when the wrist is in a neutral position, the thumb rests naturally against the radial side of the index finger.
Postoperative Care and Rehabilitation for Stage 2
The success of the flexor phase is heavily dependent on strict adherence to postoperative immobilization and subsequent phased rehabilitation.
Initial Immobilization
Immediately postoperatively, the upper extremity is placed in a well-padded, rigid orthosis or cast.
* Wrist: Immobilized in 25 to 30 degrees of extension to remove tension from the ECRL-FDP and PT-FPL transfers.
* MCP Joints: Immobilized in 40 to 50 degrees of flexion to protect the intrinsic tenodesis and prevent collateral ligament contracture.
* IP Joints: Left free or lightly supported in extension, depending on the stability of the intrinsic reconstruction.
* Thumb: Positioned in functional key pinch against the index finger.
Rehabilitation Protocol
Immobilization is strictly maintained for 3.5 to 4 weeks.
- Phase I (Weeks 4-6): The cast is removed, and a custom thermoplastic splint is fabricated in the same protective position. Gentle, active-assisted range of motion is initiated. The patient is taught to use active wrist extension to drive digital flexion (practicing the tenodesis grasp). Passive stretching of the transfers is strictly prohibited.
- Phase II (Weeks 6-8): Splint wear is gradually reduced during the day. Active motion is progressed. The patient begins light functional tasks, focusing on grasping lightweight, bulky objects (e.g., foam blocks) to train the new motor pathways.
- Phase III (Weeks 8-12): Progressive strengthening begins. The patient works on refining key pinch strength and dexterity. Heavy lifting and forceful passive stretching remain contraindicated until at least 12 weeks postoperatively.
Pitfall: Aggressive early passive stretching of the digits with the wrist in extension will inevitably stretch out the tendon weaves, leading to a catastrophic loss of the tenodesis grasp. Rehabilitation must focus on active motor re-education rather than passive flexibility.
Conclusion
The House two-stage reconstruction remains a gold-standard surgical pathway for restoring independence in patients with mid-cervical tetraplegia. By meticulously separating the extensor and flexor phases, the surgeon can achieve precise tensioning, mitigate the risk of joint contractures, and reliably restore the critical functions of digital flexion and key pinch. Mastery of the biomechanical principles, meticulous surgical handling of the tendon transfers, and a rigorous, phased postoperative rehabilitation protocol are essential for achieving optimal clinical outcomes.
You Might Also Like