Flexor Pollicis Longus Tendon Repair: A Comprehensive Surgical Guide

Key Takeaway
The repair of the flexor pollicis longus (FPL) tendon requires a precise understanding of thumb flexor zones. Surgical management is dictated by the zone of injury, timing, and tissue viability. Techniques range from direct end-to-end repair to tendon advancement and free tendon grafting. Successful outcomes depend on meticulous atraumatic tissue handling, preservation of the fibroosseous pulleys, and adherence to early active mobilization protocols to prevent adhesions and restore optimal thumb kinematics.
INTRODUCTION TO FLEXOR POLLICIS LONGUS REPAIR
The flexor pollicis longus (FPL) is a uniquely specialized musculotendinous unit, providing the solitary flexor force to the interphalangeal (IP) joint of the thumb. Its integrity is paramount for pinch strength, grasp, and overall hand dexterity. Lacerations or ruptures of the FPL tendon present unique surgical challenges due to its distinct anatomical course, its relationship with the thenar musculature, and its specific pulley system.
Unlike the flexor tendons of the triphalangeal digits, the FPL tendon lacks a robust vinculum system throughout much of its course. This anatomical idiosyncrasy allows for significant tendon advancement without compromising its intrinsic blood supply, a principle that heavily influences surgical decision-making. Successful restoration of FPL function demands a rigorous understanding of thumb flexor zones, meticulous tissue handling, precise suture techniques, and a highly structured postoperative rehabilitation protocol.
ANATOMICAL ZONES OF THE FLEXOR POLLICIS LONGUS
To standardize treatment algorithms and predict surgical outcomes, the thumb is arbitrarily divided into five distinct anatomical zones based on the specific structures that influence the type of repair chosen for the FPL.
Zone I: Distal to the Interphalangeal Joint
Zone I encompasses the area at the interphalangeal (IP) joint and extends distally to the insertion of the FPL at the base of the distal phalanx. Injuries in this zone typically leave a very short distal stump.
Zone II: The Fibroosseous Sheath
Zone II includes the critical fibroosseous sheath, extending from just proximal to the metacarpal head down to the metacarpophalangeal (MCP) joint. This is the anatomical equivalent of "no man's land" in the fingers. The FPL is constrained here by the A1 pulley, the critical oblique pulley, and the A2 pulley.
Zone III: The Thenar Eminence
Zone III corresponds to the area of the first metacarpal beneath the bulky thenar intrinsic muscles (abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis). Lacerations here often result in the proximal tendon stump retracting significantly due to muscle contraction.
Zone IV: The Carpal Tunnel
Zone IV corresponds to the carpal tunnel. The FPL tendon traverses this tight anatomical bottleneck alongside the median nerve and the nine flexor tendons of the fingers.

Zone V: The Distal Forearm
Zone V encompasses the distal forearm, just proximal to the wrist crease and the transverse carpal ligament. The musculotendinous junction of the FPL is frequently located within this zone.
PREOPERATIVE EVALUATION AND TIMING OF REPAIR
The timing of surgical intervention and the condition of the soft tissue envelope dictate the reconstructive options. Urbaniak proposed a highly organized, evidence-based system for selecting repair methods for the FPL, categorizing injuries by zone, timing (primary vs. secondary), and the degree of tissue scarring or tendon loss.
Clinical Pearl: Primary repair (within the first 72 hours) or delayed primary repair (within 1 to 2 weeks) yields the most predictable functional outcomes. After 1 month, secondary changes such as muscle contracture, tendon end swelling, and sheath scarring make direct repair exceedingly difficult, often necessitating tendon grafting or transfer.
Urbaniak’s Classification for FPL Repair
Zone I:
* Sharp Cut: Direct repair or advancement.
* Tendon Loss / Minimal Scar: Advancement (or direct repair).
* Severe Scar: Advancement.
Zone II:
* Sharp Cut: Direct repair.
* Tendon Loss / Minimal Scar: Advancement and lengthening.
* Severe Scar: Advancement and lengthening.
Zone III:
* Sharp Cut: Direct repair.
* Tendon Loss / Minimal Scar: Advancement and lengthening.
* Severe Scar: Advancement and lengthening.
Zone IV:
* Sharp Cut: Direct repair.
* Tendon Loss / Minimal Scar: Free tendon graft.
* Severe Scar: Two-stage free tendon graft.
Zone V:
* Sharp Cut: Direct repair.
* Tendon Loss / Minimal Scar: Tendon transfer (or bridge graft).
* Severe Scar: Tendon transfer.
GENERAL SURGICAL PRINCIPLES AND EXPOSURE
Anesthesia and Positioning
Surgery is typically performed under regional anesthesia (axillary or supraclavicular brachial plexus block) or general anesthesia. The patient is positioned supine with the arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, which is critical for identifying retracted tendon ends and preserving neurovascular bundles.
Surgical Incisions
To locate and mobilize the FPL, extensile exposures are often required.
* Thumb Exposure: Volar Brunner (zigzag) incisions are utilized over the volar aspect of the thumb. The apices of the flaps should end at the midaxial lines to prevent flexion contractures.
* Thenar and Wrist Exposure: Linear or gently curved incisions in the region of the thenar crease and at the distal wrist crease may be required to retrieve a retracted proximal stump.
Surgical Warning: When dissecting in Zone III (thenar eminence), meticulous care must be taken to identify and protect the recurrent motor branch of the median nerve, which lies in close proximity to the FPL sheath.
ZONE-SPECIFIC SURGICAL TECHNIQUES
Repair in Zone I
When the FPL tendon is divided within 1 cm of its insertion at the distal phalanx, direct end-to-end repair is often impossible due to the inadequate length of the distal stump.
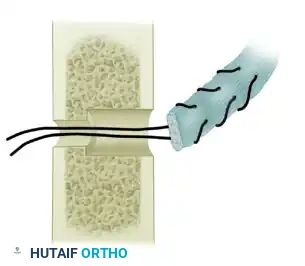
* Advancement: The proximal stump can be advanced and sutured directly into the bone using a suture anchor or a pull-out button technique over the nail plate.
* Sheath Management: A portion of the distal flexor sheath (A2 pulley) may require partial division to accommodate the advanced tendon.
* Proximal Lacerations (>1 cm from insertion): If the tendon is transected more than 1 cm from its insertion, advancing it directly to the bone will cause a severe flexion contracture of the IP joint. In these cases, the tendon must be advanced, but it requires a compensatory Z-plasty lengthening at the musculotendinous junction just proximal to the wrist.
Biomechanics Note: The FPL is unique among flexor tendons. Because it lacks a restrictive vinculum system in its proximal course, it can be advanced distally without compromising its intrinsic blood supply. This makes tendon advancement highly preferable to tendon grafting, as it significantly reduces the risk of paratendinous adhesions.
Repair in Zone II (The Critical Pulley Area)
Zone II repairs are historically fraught with complications due to the tight tolerance between the healing tendon and the fibroosseous sheath.
* Pulley Management: A portion of the A1 pulley can be excised to lessen the possibility of the repair site adhering to the sheath. However, the oblique pulley must be meticulously preserved to prevent bowstringing of the FPL, which would severely degrade pinch kinematics.
* Direct Repair: Modern multi-strand core sutures (e.g., 4-strand or 6-strand cruciate or modified Kessler) combined with a running epitendinous suture provide sufficient strength for early active motion. Results after end-to-end repair within the flexor digital sheath are now reported to be as good as, if not better than, delayed tendon reconstruction.
* Advancement Alternative: If the surgeon is less experienced, or if the tendon ends are frayed, the tendon can be advanced distally and sutured to a shortened distal stump. This strategically moves the bulky repair site distally, out from beneath the critical oblique pulley. This technique frequently requires a Z-plasty lengthening at the wrist. Urbaniak recommends an end-weave repair at the site of lengthening just proximal to the wrist to ensure robust healing.
Repair in Zone III
Lacerations in Zone III almost universally result in the proximal tendon end retracting into the carpal tunnel or distal forearm due to the unopposed pull of the FPL muscle belly.
* Retrieval: The proximal end can often be retrieved by flexing the wrist and milking the forearm distally. Atraumatic grasping forceps should be used.
* Separate Wrist Incision: If the tendon cannot be easily coaxed into the thumb wound, blind and persistent probing must be strictly avoided to prevent iatrogenic trauma to the median nerve or the tendon itself. Instead, a separate incision is made at the wrist, between the radial artery and the flexor carpi radialis (FCR).
* Rethreading the Tendon: Once identified at the wrist, the tendon must be carefully rethreaded through its normal anatomical route beneath the thenar muscles. This is best accomplished by passing a 22-gauge wire loop, a pediatric feeding tube, or a specialized tendon carrier retrograde through the sheath from the distal wound to the proximal wound. The tendon is sutured to the carrier and gently pulled distally into the thumb. Primary repair is then performed.
Repair in Zone IV
The FPL is rarely isolated in Zone IV injuries; lacerations here are typically associated with major volar wrist trauma involving the median nerve and multiple finger flexors. The FPL is somewhat protected deep within the carpal tunnel by the overhanging shelf of the radiocarpal bones.
* Technique: There is no contraindication to primary repair at this level, provided the technique is atraumatic.
* Median Nerve Protection: The most critical consideration in Zone IV is the volume of the repair. The creation of a bulky lump of suture material must be avoided, as postoperative swelling within the rigid confines of the closed carpal tunnel can precipitate acute median nerve compression (acute carpal tunnel syndrome). A low-profile core suture with a meticulous epitendinous repair is mandatory.
Repair in Zone V
In the distal forearm, primary repair of the FPL is universally indicated. The tendon ends are usually easy to locate, and the excursion space is generous. End-to-end repair is straightforward. If there is segmental tendon loss due to severe trauma, a tendon transfer (e.g., using the brachioradialis or flexor digitorum superficialis of the ring finger) or a bridge graft can be performed.
SECONDARY REPAIR AND TENDON GRAFTING
When primary repair is missed or fails, secondary reconstruction is required. However, stringent physiological requirements must be met before any secondary tendon surgery is undertaken:
- Tissue Equilibrium: Wound erythema, induration, and swelling must be minimal.
- Soft Tissue Envelope: Skin coverage must be adequate and pliable.
- Scar Bed: The tissues through which the tendon or graft is expected to glide must be relatively free of dense, unyielding scar.
- Skeletal Stability: Bone alignment must be satisfactory, and any fractures must be completely healed or rigidly fixed.
- Joint Suppleness: The MCP and IP joints must possess a useful, near-normal range of passive motion. Tendon surgery cannot overcome a stiff joint.
- Neurological Integrity: Sensation in the involved digit must be undamaged, previously restored, or capable of being repaired (directly or via nerve grafts) concurrently with the tendon repair.
Single-Stage vs. Two-Stage Grafting
- Single-Stage Grafting: If the delay is greater than 1 month, delivering the swollen FPL tendon through the collapsed fibroosseous sheath is often impossible. If the sheath is relatively unscarred and the pulleys are intact, a traditional single-stage free flexor tendon graft (using the palmaris longus or plantaris tendon) can be performed.
- Two-Stage Grafting (Hunter Rod Technique): In the presence of extensive destruction of the flexor sheath, compromised pulleys, severe scarring, or joint contractures, a two-stage reconstruction is mandatory.
- Stage 1: The scarred tendon is excised, the critical pulleys are reconstructed (using tendon slips or extensor retinaculum), and a flexible silicone rubber temporary prosthesis (Hunter and Salisbury rod) is inserted. This implant induces the formation of a smooth, biologically inert pseudosheath.
- Stage 2: After 3 to 4 months, once the soft tissues are supple and the pseudosheath has matured, the silicone rod is removed and replaced with a free autologous tendon graft.
SUPPLEMENTARY CONSIDERATIONS: FLEXOR TENDONS OF THE FINGERS
While the primary focus remains the FPL, the principles of flexor tendon management extend to the triphalangeal digits, particularly in Zones I and II.
Finger Zone I (Distal Half of Finger)
If the flexor digitorum profundus (FDP) tendon is lacerated or avulsed (Jersey finger), it must be reattached within a few days before it retracts irreversibly into the palm and before the vincula are destroyed.
* Early Treatment: An avulsed FDP can be advanced a maximum of 1 cm and reattached to the distal phalanx.
* Delayed Treatment: After a few days, the proximal tendon end swells significantly. Attempting to forcefully thread a swollen FDP through the tight bifurcation of the intact flexor digitorum superficialis (FDS) (Camper's chiasm) is contraindicated, as it will jeopardize proximal interphalangeal (PIP) joint movement and risk tethering the intact FDS.
* Grafting: Profundus function can be restored by a tendon graft, but this is highly unpredictable when routed through an intact FDS. Preoperative counseling is vital. Grafting through an intact FDS is generally reserved for children, young adults, or patients with specific occupational requirements (e.g., stringed instrument musicians, artisans) where distal interphalangeal (DIP) joint active flexion is critical.
Finger Zone II (Critical Area of Pulleys)
When the FDS tendon alone is divided in Zone II, secondary repair is generally unnecessary. The intact FDP tendon provides satisfactory global finger flexion. Attempts to repair an isolated FDS in Zone II carry a high risk of creating adhesions that will tether the functional FDP, resulting in a stiff finger. Occasionally, if a severe PIP joint hyperextension deformity (swan neck) develops due to the loss of the FDS volar stabilizing force, a superficialis tenodesis may be required.
POSTOPERATIVE REHABILITATION PROTOCOL
The success of an FPL repair is as dependent on the postoperative rehabilitation as it is on the surgical execution. The goal is to apply enough controlled stress to the healing tendon to promote intrinsic healing and prevent restrictive adhesions, without applying excessive force that could cause gap formation or rupture.
An early mobilization routine, similar to those used for finger flexors (e.g., modified Duran or Kleinert protocols), is highly recommended.
Phase I: Immobilization and Early Motion (0 to 3 Weeks)
- Splinting: Immediately postoperatively, a dorsal blocking splint is applied. The wrist is positioned in 30 to 45 degrees of flexion. The thumb MCP and IP joints are positioned in slight extension (neutral to 15 degrees). This posture maximally relaxes the FPL musculotendinous unit.
- Motion: The splint is left intact for approximately 3 weeks. Depending on the strength of the core suture, controlled passive flexion and active extension within the constraints of the dorsal block may be initiated under the strict supervision of a certified hand therapist.
Phase II: Intermediate Motion (3 to 6 Weeks)
- Transition: At 3 weeks, the static dorsal blocking splint is transitioned to a removable splint.
- Protection: The removable splint is worn between exercise sessions for an additional 3 weeks to protect the wrist and thumb against sudden, excessive hyperextension.
- Active Motion: Gentle, unresisted active flexion of the thumb is initiated. Place-and-hold exercises are highly effective during this phase to encourage tendon glide while minimizing tension across the repair site.
Phase III: Strengthening and Return to Function (8 to 12 Weeks)
- Passive Extension: Gentle passive extension exercises are introduced to treat any residual flexion contractures.
- Strengthening: At 8 weeks, progressive resistance exercises (e.g., putty squeezing, grip strengthening) are commenced.
- Vigorous Activity: Unrestricted, heavy manual labor and vigorous sports activities are generally delayed until 10 to 12 weeks postoperatively, allowing the tendon to achieve maximal tensile strength through collagen remodeling.
📚 Medical References
- Flexor pollicis longus tendon injuries in children, Ann R Coll Surg Engl 77:135, 1995.
- Havenhill TG, Birnie R: Pediatric fl exor tendon injuries, Hand Clin 21:253, 2005.
- O’Connell SJ, Moore MM, Strickland JW, et al: Results of zone I and zone II fl exor tendon repairs in children, J Hand Surg 19A:48, 1994.
- Stahl S, Kaufman T, Bialik V: Partial lacerations of fl exor tendons in children: primary repair versus conservative treatment, J Hand Surg 22B:377, 1997.
- Valenti P, Gilbert A: Two-stage fl exor tendon grafting in children, Hand Clin 16:573, 2000.
- Wagner CJ: Delayed advancement in repair of lacerated fl exor profundus tendon, J Bone Joint Surg 40A:1241, 1958.
- Flexor Tendons Al-Qattan MM: Conservative management of zone II partial fl exor tendon lacerations greater than half the width of the tendon, J Hand Surg 25A:1118, 2000.
- Athwal GS, Wolfe SW: Treatment of acute fl exor tendon injury: zones III-V, Hand Clin 21:181, 2005.
- Becker H, Davidoff M: Eliminating the gap in fl exor tendon surgery: a new method of suture, Hand 9:306, 1977.
- Bircan C, El O, Akalin E, et al: Functional outcome in patients with zone V fl exor tendon injuries, Arch Orthop Trauma Surg 125:405, 2005.
- Birnie RH, Idler RS:
You Might Also Like