Mastering Flexor Tendon Pulley Reconstruction and Two-Stage Grafting
Key Takeaway
Reconstruction of the flexor tendon pulley system is critical for restoring digital biomechanics and preventing bowstringing. This surgical guide details the indications, operative techniques, and staged protocols for flexor pulley reconstruction and two-stage tendon grafting. Emphasizing the preservation of the A2 and A4 pulleys, it covers graft selection, Silastic rod placement, and precise postoperative rehabilitation to optimize functional outcomes in severely traumatized digits.
SURGICAL ANATOMY AND BIOMECHANICS OF THE FLEXOR PULLEY SYSTEM
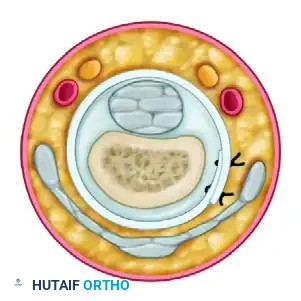
The digital flexor sheath is a highly specialized fibro-osseous tunnel lined by synovium, designed to provide a low-friction gliding environment for the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons. Mechanically, the pulley system maintains the tendons in close apposition to the phalangeal axis, optimizing the moment arm and translating linear muscle excursion into angular joint rotation.
The system comprises five annular (A1-A5) and three cruciate (C1-C3) pulleys. From a reconstructive standpoint, the A2 pulley (located over the proximal half of the proximal phalanx) and the A4 pulley (located over the middle third of the middle phalanx) are the most biomechanically critical. Loss of these pulleys results in "bowstringing" of the flexor tendons during active flexion. Bowstringing increases the moment arm, which paradoxically increases the mechanical advantage but severely depletes the available tendon excursion, resulting in a profound loss of active distal interphalangeal (DIP) and proximal interphalangeal (PIP) joint flexion.
Clinical Pearl: While the A2 and A4 pulleys are indispensable, preserving or reconstructing the A1 and A3 pulleys can provide supplementary mechanical support, particularly in cases of severe trauma. However, reconstructing a pulley directly over the PIP joint must be avoided, as it will mechanically restrict joint motion and lead to intractable stiffness.
INDICATIONS FOR RECONSTRUCTION
Primary repair of flexor tendons is always preferred; however, in the setting of delayed presentation, severe crush injuries, extensive fibro-osseous scarring, or failed primary repairs, the native tendon bed is often obliterated.
A two-stage tendon reconstruction utilizing a passive gliding silicone implant (Hunter rod) is indicated for patients with:
* Excessive scarring of the flexor tendon sheath (Zone II "No Man's Land").
* Concomitant joint stiffness requiring intensive therapy prior to tendon grafting.
* Severe digital trauma necessitating staged reconstruction of neurovascular bundles or soft tissue coverage.
Surgical Warning: A patient with a severely contracted, scarred digit—especially in the presence of significant neurovascular insufficiency—may be better served by arthrodesis or amputation. Two-stage tendon reconstruction demands immense patient compliance, requiring a minimum of two surgeries and months of rigorous rehabilitation.
SURGICAL TECHNIQUE: STAGE I – PULLEY RECONSTRUCTION AND IMPLANT PLACEMENT
The primary objective of the first stage is to excise the scarred tendon, perform a radical tenosynovectomy, reconstruct the critical A2 and A4 pulleys, and insert a Dacron-impregnated silicone rod to generate a biologically active, pseudo-synovial sheath.
Incision and Exposure
- Surgical Approach: Utilize a Bruner zigzag, midlateral, or volar oblique incision to expose the volar aspect of the digit. The exposure must be extensile, providing visualization of the entire flexor pulley system from the distal phalanx to the palm.
- Sheath Evaluation: Carefully evaluate the fibro-osseous sheath. Retain any portion of the sheath that remains unscarred and pliable. Preservation of the native A1 pulley in the palm and the distal sheath near the DIP joint is highly advantageous.
- Tendon Excision: Excise the scarred FDS and FDP tendons along with surrounding fibrotic tissue.
- Proximal Release: Bring the proximal tendon stumps out through an additional palmar or distal forearm incision to complete their excision. Leave the proximal FDP tendon attached to the lumbrical muscle to prevent proximal retraction and maintain its resting length for the second stage.
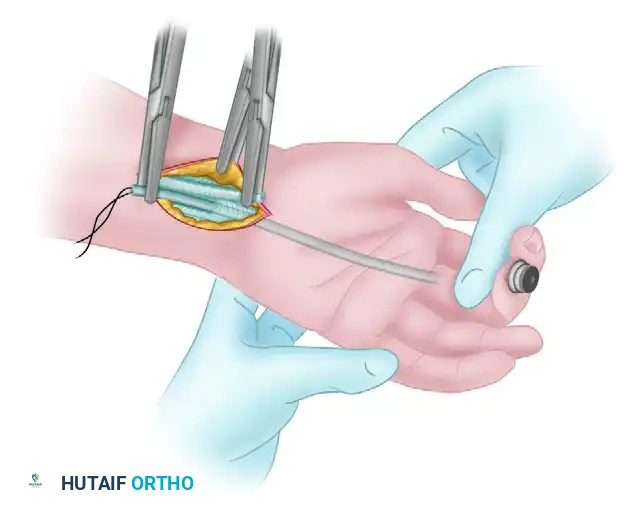
Insertion of the Silastic Implant (Hunter Rod)
- Select a Dacron-impregnated silicone rod (Hunter prosthesis) of appropriate diameter. The rod must glide passively within the reconstructed sheath without buckling or excessive friction.
- Distal Fixation: Attach the rod distally. This can be achieved by suturing it to the remaining distal stump of the profundus tendon or securing it directly to the distal phalanx using a small bone screw or suture anchor.
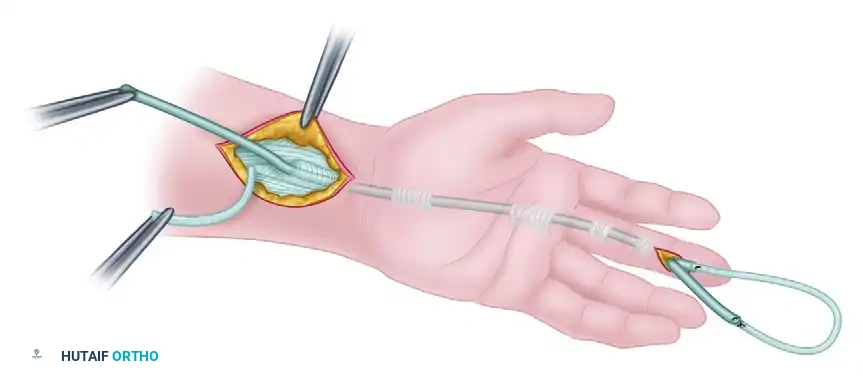
- Proximal Placement: Pass the rod proximally through the palm and into the distal forearm. The proximal end should rest in a healthy, scar-free soft-tissue bed approximately 5 cm proximal to the wrist crease. This allows the new pseudo-sheath to extend into the forearm, facilitating the proximal anastomosis during Stage II.
Techniques for Pulley Reconstruction
If the native A2 and A4 pulleys are incompetent or destroyed, they must be reconstructed over the silicone rod. Several techniques are available, typically utilizing a free tendon graft (e.g., palmaris longus, plantaris, or a strip of the excised FDS) measuring at least 6 cm in length and 0.25 cm in width.
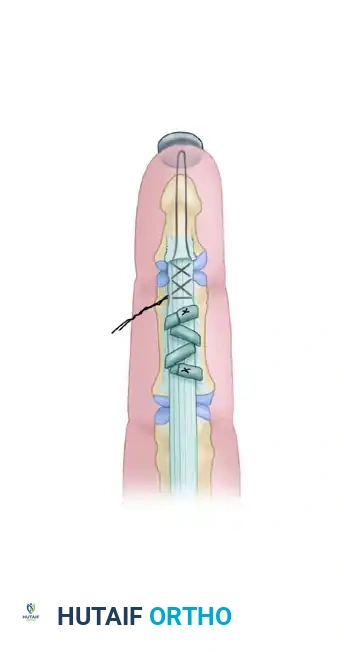
Technique A: Weaving Through an Intact Fibro-osseous Rim
If the original fibro-osseous rim of the flexor sheath remains robustly attached to the periosteum, the tendon graft can be woven directly through this rim.
* Pass the graft through the native rim on one side, over the silicone rod, and through the rim on the contralateral side.
* Secure the weave with non-absorbable mattress sutures.
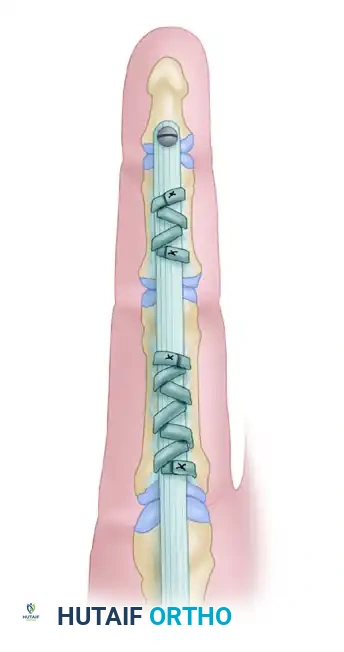
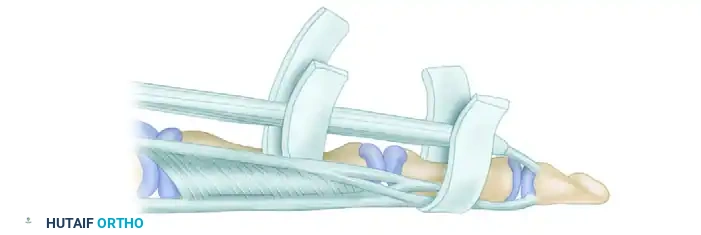
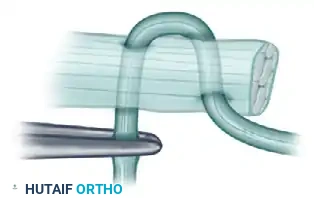
Technique B: Circumferential Phalangeal Reconstruction
If the fibro-osseous rim is insufficient or avulsed, the tendon graft must be passed circumferentially around the phalanx.
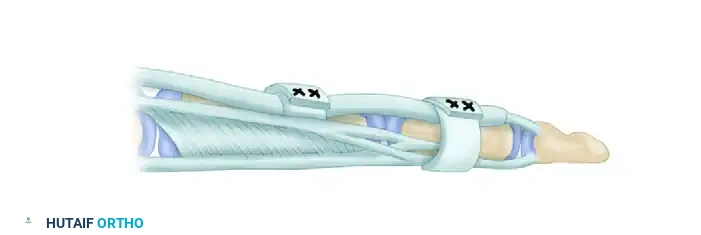
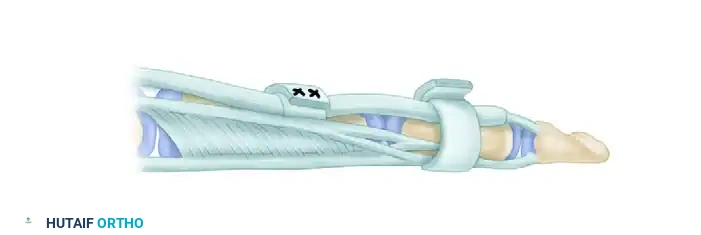
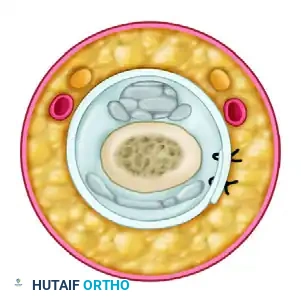
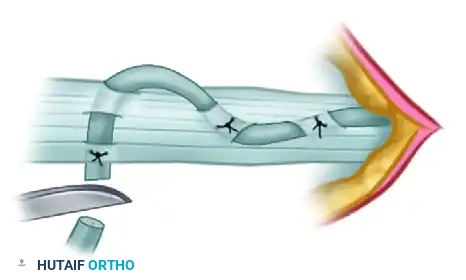
- A2 Pulley Reconstruction (Proximal Phalanx): Pass the tendon graft over the silicone rod and circumferentially around the proximal phalanx. Crucially, the graft must pass deep to the extensor tendon mechanism to avoid tethering extensor excursion.
- A4 Pulley Reconstruction (Middle Phalanx): Pass the tendon graft over the silicone rod and circumferentially around the middle phalanx. At this level, the graft is passed superficial to the extensor tendon (lateral bands), as passing it deep would interfere with the delicate distal extensor mechanism.
Surgical Pitfall: The suture line represents the weakest point of the reconstructed pulley. After securing the graft to itself with multiple mattress sutures, rotate the reconstructed pulley so that the suture knot lies along the lateral aspect of the digit, away from the direct volar gliding surface of the rod.
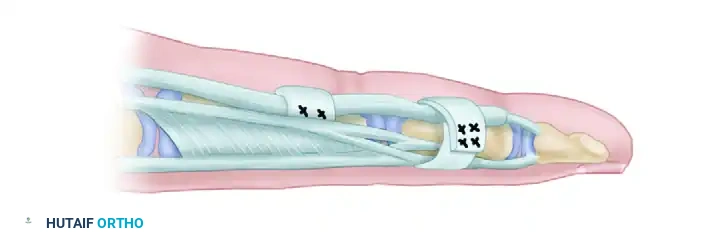
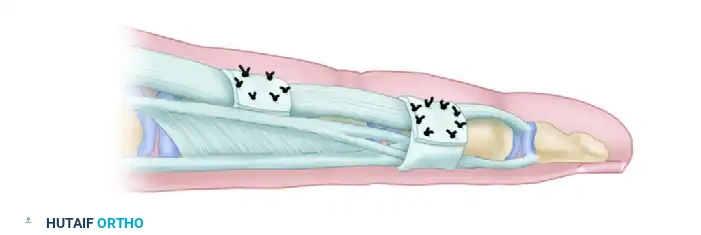
Technique C: Extensor Retinaculum Graft (Lister's Technique)
Alternatively, a strip of extensor retinaculum harvested from the wrist can be utilized. The retinaculum provides a smooth, pre-formed synovial gliding surface.
* Use a piece of heavy silk suture passed around the finger to accurately template the required length of the retinacular graft before harvesting.
* Wrap the retinaculum around the phalanx and secure it, ensuring the smooth synovial surface faces the silicone rod.
SURGICAL TECHNIQUE: STAGE II – TENDON GRAFTING
Stage II is performed approximately 3 months after Stage I. This delay allows for complete healing of the reconstructed pulleys, resolution of digital edema, and the maturation of a smooth, mesentery-like pseudo-synovial sheath around the silicone rod.
Implant Removal and Graft Passage
- Incision: Re-open the distal digital incision to expose the distal attachment of the rod. Open the proximal forearm incision to expose the proximal end of the rod.
- Graft Selection: Harvest a suitable autologous tendon graft (e.g., palmaris longus, plantaris, or long toe extensor).
- Graft Passage: Suture the proximal end of the tendon graft securely to the proximal end of the silicone prosthesis in the forearm.
- Apply gentle, steady traction to the distal end of the prosthesis in the finger. As the prosthesis is withdrawn distally, it seamlessly pulls the tendon graft through the newly formed pseudo-sheath and beneath the reconstructed pulleys.
Distal Anastomosis
The distal anastomosis must be robust enough to withstand early active motion protocols.
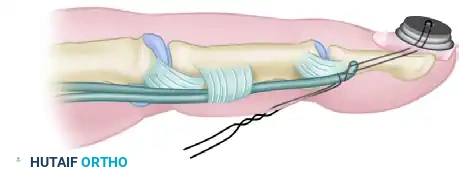
1. Secure the distal end of the tendon graft to the distal phalanx or the robust stump of the FDP.
2. A classic Bunnell pull-out suture technique is frequently employed. The suture is passed through the distal phalanx and tied over a button on the sterile matrix of the fingernail.
3. Reinforcing sutures are placed through the remaining stump of the profundus tendon to augment the repair.
Proximal Anastomosis and Tensioning
Setting the correct tension at the proximal anastomosis is the most technically demanding aspect of Stage II. Incorrect tensioning will result in either a severe flexion contracture or a profound lag in active flexion.
- Motor Selection: Identify the proximal motor tendon (usually the native FDP or FDS of the affected digit). Measure the excursion of the tendon graft and the amplitude of the motor muscle. If performed under wide-awake local anesthesia no tourniquet (WALANT), the true amplitude of active muscle contraction can be directly observed and tensioned dynamically.
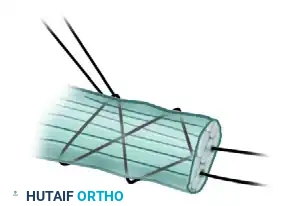
- Pulvertaft Weave: Utilize a Pulvertaft weave for the proximal anastomosis to provide maximum biomechanical strength.
- "Fish-mouth" the stump of the motor tendon.
- Thread the graft through the motor tendon two or three times at 90-degree angles.
- Tensioning: Adjust the tension so that the reconstructed digit rests in slightly more flexion than its normal position in the natural digital cascade. Place a single temporary holding suture.
- Assess the tenodesis effect by passively flexing and extending the wrist. If the tension is incorrect, remove the temporary suture, adjust the weave length, and reassess.
- Once optimal tension is achieved, complete the anastomosis with multiple non-absorbable mattress sutures.


POSTOPERATIVE REHABILITATION PROTOCOLS
The success of flexor tendon and pulley reconstruction is inextricably linked to the postoperative rehabilitation program. A delicate balance must be struck between protecting the reconstructed tissues and preventing restrictive adhesions.
Phase I: Post-Stage I (Pulley Reconstruction & Rod Placement)
- Immobilization: The hand is supported in a dorsal blocking splint with the wrist in 20° of flexion, MCP joints in 70° of flexion, and IP joints in full extension.
- Motion Protocol: Passive motion of the finger joints is initiated at 7 to 10 days postoperatively. The patient is instructed in gentle passive flexion and extension exercises to maintain joint suppleness and encourage the formation of a smooth pseudo-sheath around the implant.
- Adjuncts: Buddy strapping to adjacent fingers can help guide motion and prevent rotational deformities. If pulley reconstruction was performed concomitantly with a flexor tenolysis, an external orthotic ring should be worn over the reconstructed pulley site to provide external mechanical support and prevent early bowstringing.
Phase II: Post-Stage II (Tendon Grafting)
- Early Phase (0-4 weeks): The patient is placed in a dorsal blocking splint. A modified Duran or Kleinert early passive motion protocol is initiated within the first 3-5 days to promote intrinsic tendon healing and prevent graft adhesions.
- Intermediate Phase (4-6 weeks): The dorsal blocking splint is gradually discontinued. Active place-and-hold exercises are initiated.
- Late Phase (6-12 weeks): Progressive resistance exercises are introduced. Full unrestricted activity is generally not permitted until 10 to 12 weeks postoperatively to ensure complete graft incorporation and tensile strength maturation.
> Clinical Pearl for Tenolysis: If a standalone tenolysis is performed (without grafting), active motion must be initiated aggressively within the first 72 hours. Delaying motion beyond this window allows restrictive hematoma and early scar tissue to organize, rapidly negating the surgical release.
You Might Also Like


