Primary Flexor Tendon Repair: Surgical Techniques & Zones

Key Takeaway
Primary flexor tendon repair requires meticulous surgical technique and a profound understanding of hand biomechanics. Outcomes depend heavily on the anatomical zone of injury, particularly within Zone II's fibro-osseous sheath. Successful repair necessitates precise core and peripheral suturing, preservation of the A2 and A4 pulleys, and careful management of the flexor digitorum sublimis and profundus relationship. This guide details zone-specific approaches, surgical pearls, and rehabilitation protocols to optimize functional recovery.
INTRODUCTION TO PRIMARY FLEXOR TENDON REPAIR
The primary repair of flexor tendons remains one of the most technically demanding procedures in hand surgery. The ultimate functional outcome is inextricably linked to the initial surgeon’s skill, the precise management of the fibro-osseous sheath, and the rigorous application of postoperative rehabilitation protocols. Historically fraught with high rates of adhesion and rupture, modern primary flexor tendon repair—when executed by an experienced hand surgeon—yields satisfactory to excellent functional results in over 80% of patients.
Outcomes are generally superior in younger demographics (particularly patients under 40 years of age) and significantly outpace the results of secondary repairs or staged tendon reconstructions. The decision to perform a primary repair carries profound responsibility; the operating surgeon must possess the advanced microsurgical proficiency required to perform subsequent tenolysis or tendon grafting should the primary repair fail.
ANATOMICAL ZONES OF THE FLEXOR SURFACE
The surgical approach, prognosis, and potential complications of flexor tendon repair are dictated by the specific anatomical zone of injury. The flexor surface of the hand is universally divided into five distinct zones based on the unique biomechanical and anatomical challenges present in each region.
Zone I: Distal to the Sublimis Insertion
Zone I extends from just distal to the insertion of the flexor digitorum sublimis (FDS) tendon to the terminal insertion of the flexor digitorum profundus (FDP) tendon at the base of the distal phalanx. Injuries here isolate the FDP.
Zone II: "No Man’s Land"
Zone II encompasses the critical area of the flexor pulley system, extending from the distal palmar crease to the insertion of the FDS tendon. Coined "no man's land" by Bunnell due to historically poor outcomes, this zone houses both the FDS and FDP tendons within a tight fibro-osseous sheath, making it highly susceptible to post-surgical adhesions.
Zone III: Lumbrical Origin
Zone III comprises the area between the distal margin of the transverse carpal ligament and the proximal reflection of the flexor sheath (the A1 pulley). This zone is characterized by the origin of the lumbrical muscles from the FDP tendons.
Zone IV: The Carpal Tunnel
Zone IV represents the segment of tendons passing deep to the transverse carpal ligament (TCL) within the carpal tunnel. Space is highly restricted here, and injuries are frequently accompanied by median nerve lacerations.
Zone V: Proximal to the Carpal Tunnel
Zone V extends proximally from the transverse carpal ligament into the distal forearm. Tendon gliding is generally excellent in this zone due to the presence of loose paratenon rather than a restrictive synovial sheath.
BIOMECHANICS AND SUTURE CONFIGURATION
The mechanical integrity of a flexor tendon repair must withstand the forces of early active motion protocols to prevent adhesion formation while avoiding gap formation or rupture.
Core Suture Techniques
In Zone II and beyond, a core suture utilizing two or more strands, locking components, and buried knots is the foundational standard. However, contemporary evidence strongly supports the use of a four-strand or six-strand core suture. Increasing the number of strands crossing the repair site directly correlates with increased tensile strength, permitting a postoperative routine of light active flexion with the wrist extended.
Clinical Pearl: Placing the core sutures in the dorsal half of the tendon provides a mean repair strength that is 58% greater than sutures placed in the volar half. Traditionally, volar placement was advocated to preserve intratendinous circulation, but the biomechanical advantage of dorsal placement is now widely recognized as critical for early active motion.
Peripheral Epitendinous Sutures
A running, circumferential peripheral suture (typically 5-0 or 6-0 monofilament nylon) is mandatory. This peripheral stitch serves two vital functions:
1. It increases the overall tensile strength of the repair by up to 50%.
2. It smooths the repair site, minimizing adhesion formation and preventing "triggering" or catching on the annular pulleys during excursion.
Suture Materials
The choice of suture material is dictated by surgeon preference and handling characteristics. Most master surgeons prefer synthetic, braided, non-absorbable or slowly absorbable materials for the core suture (e.g., Mersilene, Tycron, Tevdek, Fiberwire). Monofilament nylon or stainless steel wire may also be utilized successfully in specific scenarios. Typically, 3-0 or 4-0 caliber is required for the core repair.
ZONE-SPECIFIC SURGICAL TECHNIQUES
Zone I Repair Strategies
In Zone I, the FDP tendon is often lacerated near its insertion. If the distal stump is 1 cm or less, the proximal tendon can be advanced and reinserted directly into the distal phalanx using a pull-out wire technique or suture anchors.
Surgical Warning: The 1-Centimeter Rule
Extreme caution must be exercised when advancing the FDP tendon. The "1-cm rule" dictates that the total advancement—including the excised tendon, any "kinking" or bunching, and the length inserted into the bone—must not exceed 1 cm.
Excessive advancement alters the resting tension of the finger, disrupting the normal digital "cascade." More critically, because the FDP tendons share a common muscle belly, over-tensioning one tendon restricts the excursion of the adjacent, uninjured FDP tendons. This phenomenon, described by Verdan, is known as the "quadriga effect." If excessive shortening has occurred, tendon lengthening at the wrist or a staged tendon graft must be considered.
Management of FDP Avulsions (Jersey Finger)
When diagnosis is delayed, the FDP may retract proximally, disrupting its vincula. Ruptures are classified by retraction level:
* Type 1: Retracted into the palm. Must be repaired within 7 to 10 days before the tendon becomes contracted and the sheath collapses.
* Type 2: Retracted to the PIP joint. Can occasionally be reattached even after a few months.
* Type 3: Retracted to the DIP joint, usually with a bony avulsion fragment. Easily reattached, though some limitation in DIP joint motion is expected.
Zone II Repair Strategies ("No Man's Land")
Primary repair of both the FDS and FDP tendons in Zone II is now the gold standard, superseding historical recommendations to excise the FDS. Exacting tissue handling is paramount.
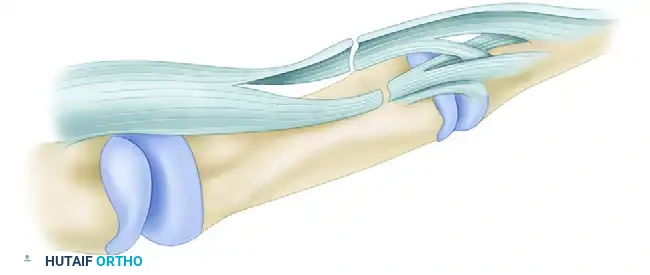
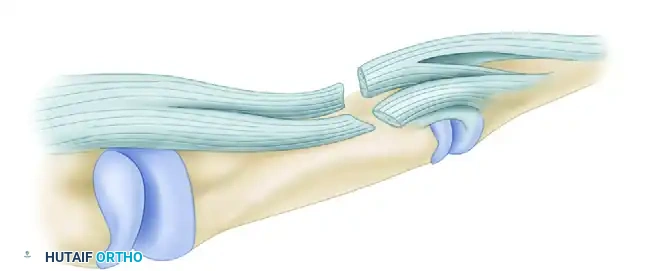
Pulley Preservation
Most of the annular pulley component of the fibro-osseous sheath must be preserved to prevent bowstringing and loss of mechanical advantage. The A2 and A4 pulleys are biomechanically critical and must be meticulously protected or reconstructed. Repairing defects in the synovial sheath is also recommended to restore the gliding surface and contain synovial fluid, which aids in intrinsic tendon nutrition.
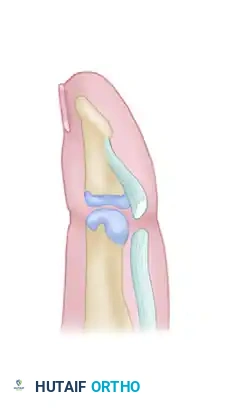
Managing the Sublimis Spiral (Camper's Chiasma)
A profound understanding of the FDS anatomy is required to avoid catastrophic surgical errors. Just distal to the metacarpophalangeal (MCP) joint, the FDS splits into two slips. These slips wind around the FDP tendon, decussating at Camper's chiasma to insert on the middle phalanx. During this spiral, the superficial portion of the proximal FDS becomes deep.

Surgical Pitfall: If a laceration occurs at the midpoint of this spiral, the proximal and distal ends rotate 90 degrees in opposite directions. An unwary surgeon may suture ends that appear to align but are actually malrotated. This obliterates the channel for the FDP tendon, blocking excursion and destroying functional motion.
Delivering the Retracted Profundus
When the FDP has retracted proximally, it must be carefully delivered back through the split portion of the FDS. The anatomical relationship must be perfectly reestablished, ensuring the FDP lies palmar to Camper's chiasma before passing distally into the digit.
Zone III Repair Strategies
In Zone III, lacerations frequently involve both the tendons and the lumbrical muscle bellies. Primary repair of all tendons is indicated. Furthermore, primary repair of sharply severed digital nerves is crucial; delaying nerve repair even a few weeks results in significant retraction and gaps.
Surgical Pitfall: Do not suture the lumbrical muscle bellies. Suturing the lumbricals increases their resting tension. When the patient attempts active finger flexion, the increased tension is transmitted through the lateral bands, resulting in paradoxical PIP joint extension—a debilitating condition known as the "lumbrical plus" finger.
Zone IV Repair Strategies
Injuries within the carpal tunnel require partial or complete release of the transverse carpal ligament (TCL) for adequate exposure.
If the TCL is completely released, the wrist must not be splinted in flexion past neutral postoperatively. Flexing the wrist beyond neutral allows the repaired tendons to subluxate out of their normal bed, bowstringing directly beneath the sutured skin. To prevent this, the TCL can be released using a Z-lengthening configuration, allowing it to be repaired loosely to act as a retaining pulley while accommodating postoperative swelling.
Zone V Repair Strategies
Because Zone V lacks a restrictive fibro-osseous sheath, tendon gliding after repair is typically excellent. All lacerated tendons and nerves should be repaired primarily.
Exposure often requires proximal and distal extension of the transverse laceration. Blood clots within the tenosynovium serve as anatomical breadcrumbs to locate severed tendon ends. While hematoma evacuation is necessary, a total synovectomy is contraindicated. Note that at this level, the FDP tendons are not completely separated into individual units, whereas the FDS tendons are distinct. An isolated laceration of the palmaris longus tendon does not require repair.
DELAYED PRESENTATIONS AND SALVAGE PROCEDURES
In cases of old, untreated injuries (particularly in Zone I), primary repair is often impossible due to tendon retraction and muscle contracture. Treatment options include:
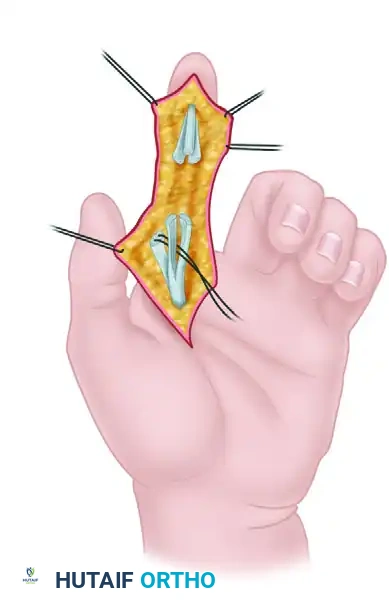
1. Tendon Grafting: Recommended for highly motivated patients (typically aged 10-21) with supple joints. The graft may be passed around the intact FDS tendon, or a two-stage reconstruction utilizing a silicone Hunter rod may be employed.
2. Tenodesis or Arthrodesis: For older, non-compliant patients, or those with joint stiffness, arthrodesis of the DIP joint provides a stable, functional digit without the high risks associated with tendon grafting.
POSTOPERATIVE MANAGEMENT AND TENOLYSIS
The success of a primary flexor tendon repair is equally dependent on the surgical execution and the postoperative rehabilitation protocol. A four-strand core repair combined with a peripheral epitendinous suture is robust enough to withstand early active motion (EAM). EAM protocols (such as the modified Belfast or Indiana protocols) involve light active flexion with the wrist extended, which significantly reduces adhesion formation compared to historical passive-only protocols (e.g., Kleinert or Duran).
Indications for Tenolysis
Despite optimal technique, adhesions may still form, restricting glide. Tenolysis is required in an estimated 18% to 25% of patients.
Criteria for Tenolysis:
* The patient has reached a definitive plateau in postoperative rehabilitation.
* Wounds are completely supple, and skin is soft with minimal induration.
* Fractures are fully healed, and joint contractures are resolved (near-normal passive range of motion is mandatory).
* A minimum of 3 to 6 months has elapsed since the primary repair.
Flexor tenolysis is a technically demanding salvage procedure that requires extensive experience. When performed correctly on a properly selected patient, active digital function can be improved by upwards of 50%.
You Might Also Like