Flexor Tendon Grafting of the Flexor Pollicis Longus: A Masterclass in Surgical Reconstruction
Key Takeaway
Flexor tendon grafting of the flexor pollicis longus (FPL) is a critical salvage procedure for delayed presentations or segmental tendon loss. This comprehensive guide details the precise surgical approach, critical pulley preservation, graft harvesting, tensioning biomechanics, and rigorous postoperative rehabilitation protocols required to restore thumb kinematics, prevent bowstringing, and optimize functional outcomes in complex hand reconstruction.
Introduction to Flexor Pollicis Longus Tendon Grafting
The reconstruction of the flexor pollicis longus (FPL) tendon via free tendon grafting is a technically demanding procedure reserved for scenarios where primary repair is impossible. Such situations typically arise from delayed presentations, neglected ruptures, severe crush injuries with segmental tendon loss, or failed primary repairs resulting in extensive scarring and tendon retraction.
Unlike the multi-tendon systems of the lesser digits, the thumb relies solely on the FPL for interphalangeal (IP) joint flexion. Consequently, restoring the precise biomechanical tension and excursion of the FPL is paramount for overall hand function, grip strength, and fine pinch kinematics. This comprehensive guide delineates the postgraduate-level surgical techniques, anatomical considerations, and rigorous postoperative protocols required to execute a successful single-stage flexor tendon graft of the thumb.
Surgical Anatomy and Biomechanics
A profound understanding of the thumb's unique flexor anatomy is non-negotiable for the reconstructive hand surgeon. The FPL tendon traverses a specialized fibro-osseous canal that differs significantly from the digital sheaths of the fingers.
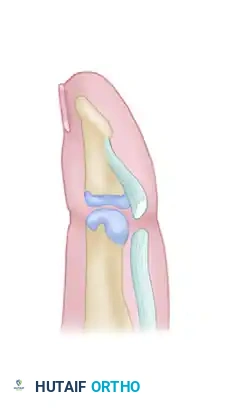
The Thumb Pulley System
The thumb pulley system is composed of three primary pulleys that maintain the FPL tendon closely apposed to the phalanges, thereby maximizing mechanical advantage and preventing bowstringing:
1. The A1 Pulley: Located at the level of the metacarpophalangeal (MCP) joint.
2. The Oblique Pulley: Originates proximally on the ulnar aspect of the proximal phalanx and inserts distally on the radial aspect. It is the most critical pulley for preventing bowstringing and maintaining the biomechanical excursion of the FPL.
3. The A2 Pulley: Located just proximal to the IP joint.
💡 Clinical Pearl: Pulley Preservation
The absolute minimum requirement for functional FPL excursion without bowstringing is the preservation (or reconstruction) of the oblique pulley and a robust segment of the A1 pulley (at least 1 cm wide over the MCP joint). Failure to preserve these structures will result in a profound loss of IP joint flexion secondary to a loss of mechanical advantage.
Neurovascular Anatomy
The digital neurovascular bundles of the thumb are positioned more volarly (anteriorly) than those of the fingers. The radial digital nerve is particularly vulnerable during radial-sided surgical approaches and must be meticulously identified and protected.
Preoperative Planning and Patient Positioning
Indications for Single-Stage Grafting
Single-stage tendon grafting is indicated when there is segmental tendon loss but the fibro-osseous sheath is relatively pliable, the pulley system is intact (or reconstructable), and the soft tissue bed is well-vascularized and free of dense cicatrix. If the sheath is heavily scarred or the pulleys are destroyed, a two-stage reconstruction utilizing a silicone Hunter rod is mandated.
Graft Selection
The ideal tendon graft must possess adequate length, a small cross-sectional area to glide smoothly within the thumb sheath, and minimal donor site morbidity.
* Palmaris Longus (PL): The gold standard. Present in approximately 85% of the population. It offers ideal length and caliber.
* Plantaris Tendon: An excellent alternative if the PL is absent, providing substantial length.
* Toe Extensor Digitorum Longus (EDL): Typically harvested from the second or third toe. Useful when upper extremity grafts are unavailable.
Positioning and Anesthesia
- Positioning: Supine with the operative arm extended on a radiolucent hand table.
- Anesthesia: Regional block (axillary or supraclavicular brachial plexus block) is preferred, supplemented with intravenous sedation.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
Step-by-Step Surgical Technique
1. Incision and Exposure of the Thumb
The surgical approach must provide extensive exposure while preventing postoperative scar contractures across flexion creases.
- The Incision: Make a precise incision on the radial side of the thumb, commencing near the base of the nail. Extend it proximally to the middle of the first metacarpal. From this point, angle the incision toward the palm, terminating near the middle of the thenar eminence.
- Flap Elevation: Elevate the skin and subcutaneous tissue as a unified, full-thickness flap with its base directed toward the palm.
- Neurovascular Protection: Carefully dissect the terminal branches of the radial nerve and the corresponding radial digital vessels. Retract them gently with the volar flap. The digital neurovascular bundle lies well toward the anterior aspect of the thumb; meticulous blunt dissection is required to avoid iatrogenic injury.
2. Pulley Management and Tendon Preparation
- Sheath Exposure: Identify the fibro-osseous sheath and the pulley system.
- Sheath Incision: Open the tendon sheath and the pulleys sufficiently to allow for the clearance of scar tissue and the eventual insertion of the tendon graft.
- Critical Preservation: You must leave a segment of the A1 pulley at least 1 cm wide intact over the MCP joint. Furthermore, the oblique pulley (located at the proximal and middle thirds of the proximal phalanx) must be left entirely intact.
- Tendon Excision: Free the scarred or retracted remnants of the native FPL tendon. Exercise extreme caution to avoid entering the interphalangeal joint capsule or damaging its volar plate, which could lead to postoperative joint stiffness or subluxation.
⚠️ Surgical Warning: Volar Plate Integrity
Iatrogenic violation of the IP joint volar plate during distal tendon excision can result in severe postoperative flexion contractures or joint instability. Dissect strictly within the tendon sheath.
3. Proximal Exposure and Tendon Retrieval
- Wrist Incision: Make a transverse incision approximately 2.5 cm long, located just proximal to the flexor crease of the wrist.
- FPL Identification: Deepen the dissection through the antebrachial fascia. Identify the FPL tendon muscle belly and its tendinous junction, which lies radial to the flexor digitorum superficialis (FDS) tendons.
- Tendon Withdrawal: Withdraw the proximal stump of the FPL tendon into the wrist wound.
- Tagging: Crucial step: If the distal remnant of the FPL is still present in the carpal tunnel, tag its distal end with a non-absorbable suture before withdrawing it proximally. This suture will act as a vital guide-wire for threading the new tendon graft through the carpal tunnel and into the thumb.
4. Graft Harvesting
Harvest the selected graft (e.g., Palmaris Longus) using standard minimally invasive techniques (e.g., utilizing a Brand tendon stripper). Ensure the graft is kept moist in saline-soaked gauze until ready for insertion.
5. Distal Fixation of the Graft
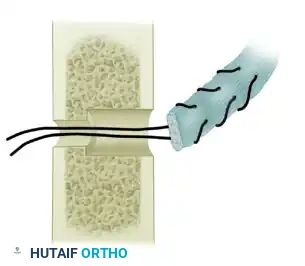
- Insertion Site: The distal end of the graft must be anchored precisely at the anatomical insertion footprint of the native FPL tendon at the base of the distal phalanx.
- Fixation Technique: This can be achieved using a classic Bunnell pull-out suture technique (exiting the dorsal nail matrix and tied over a button) or, more contemporarily, utilizing a micro-suture anchor embedded into the volar base of the distal phalanx. Ensure the fixation is robust enough to withstand early active motion protocols.
6. Proximal Juncture and Tensioning (The End-Weave)
The proximal anastomosis is the most critical determinant of postoperative function. The tension must be set perfectly to restore the natural tenodesis cascade of the hand.
- Weave Technique: Utilize the Pulvertaft end-weave technique. Suture the proximal end of the graft to the distal end of the FPL tendon at a level proximal to the wrist crease.
- Anatomical Consideration: The juncture must be positioned so that it does not enter the carpal tunnel or encroach upon the median nerve during full thumb and wrist extension. A bulky Pulvertaft weave within the carpal canal will cause acute carpal tunnel syndrome and restrict tendon glide.
- Setting the Tension: The graft should be placed under enough tension to slightly flex the IP joint of the thumb when the wrist is held in a neutral position.
- Intraoperative Tenodesis Test:
- Place a single mattress suture through the first pass of the end-weave to hold the tension temporarily.
- Extend the wrist maximally: This should produce full, passive flexion of the thumb IP and MCP joints.
- Flex the wrist maximally: This should produce full, passive extension of the thumb.
- Final Fixation: Once the tension is deemed satisfactory, place additional mattress sutures (typically using 3-0 or 4-0 non-absorbable braided suture) to secure the Pulvertaft weave. Ensure the weave is smooth and tapered to prevent catching on surrounding fascia.
🔪 Surgical Technique 66-16: The Metacarpal Juncture Alternative
As an alternative method, particularly when the proximal FPL tendon is healthy and reaches the mid-hand, the proximal end of the graft can be sutured to the native tendon opposite the middle of the thumb metacarpal.
Advantage: This requires only a single incision and completely avoids the carpal tunnel, thereby eliminating potential median nerve complications and wrist-level adhesions.
Closure and Immobilization
- Hemostasis: Deflate the tourniquet and achieve meticulous hemostasis using bipolar electrocautery. Hematoma formation is a primary catalyst for restrictive adhesions.
- Wound Closure: Close the skin with 5-0 nylon or a similar monofilament non-absorbable suture. Subcutaneous sutures are strictly avoided to minimize foreign body reactions and subsequent scarring near the tendon graft.
- Splinting: Apply a robust dorsal blocking splint to the wrist, hand, and thumb.
- Wrist: Positioned in 45 degrees of flexion.
- Thumb MCP: Positioned in slight flexion.
- Thumb IP: Positioned in full extension.
This posture removes tension from the proximal anastomosis and the distal insertion site.
Postoperative Care and Rehabilitation Protocol
The success of a flexor tendon graft is equally dependent on the surgical execution and the postoperative rehabilitation. A delicate balance must be struck between protecting the graft from rupture and preventing restrictive adhesions.
Phase 1: Weeks 0 to 3 (Protection and Early Passive Motion)
- The dorsal blocking splint is worn continuously.
- Edema control is paramount.
- Passive flexion and active extension within the constraints of the dorsal splint are initiated under the strict supervision of a certified hand therapist.
- If a pull-out suture and button were utilized for distal fixation, they are removed at the 3-week mark.
Phase 2: Weeks 3 to 7 (Active Motion Initiation)
- At 3 weeks, the pull-out suture is removed.
- Active motion is cautiously begun. The patient initiates active place-and-hold exercises.
- The dorsal blocking splint is modified to allow greater wrist extension but continues to protect against hyperextension of the thumb and wrist. Splint protection against hyperextension is strictly continued for 7 to 8 weeks.
Phase 3: Weeks 7 to 10 (Strengthening)
- At 7 weeks, the splint is typically discontinued during the day.
- Active flexion exercises are progressively increased.
- Gentle blocking exercises are introduced to isolate FPL glide.
- By 9 to 10 weeks, the patient is progressed to heavy resistance exercises, pinch strengthening, and full functional integration.
🛑 Pitfall: Premature Resistance
Initiating resistance exercises before the 8-week mark dramatically increases the risk of graft rupture or elongation at the Pulvertaft weave. The biological integration of a free tendon graft is slower than that of a primary tendon repair. Patience is a clinical virtue.
Complications and Management
- Tendon Adhesions: The most common complication. If active range of motion plateaus despite rigorous therapy for 3-6 months, a surgical tenolysis may be indicated.
- Graft Rupture: Usually occurs at the proximal or distal juncture due to non-compliance with the splinting protocol. Requires immediate surgical exploration and potential revision grafting.
- Bowstringing: Results from failure to preserve or reconstruct the oblique and A1 pulleys. Presents as a loss of active IP flexion despite good tendon excursion. Requires secondary pulley reconstruction using tendon slips or extensor retinaculum.
- Median Nerve Compression: Caused by placing a bulky Pulvertaft weave within the carpal tunnel. Prevented by ensuring the proximal juncture remains proximal to the wrist crease during full extension.
Conclusion
Flexor tendon grafting of the flexor pollicis longus is a highly rewarding procedure that can restore vital thumb kinematics in the setting of complex trauma. By adhering strictly to the principles of atraumatic tissue handling, meticulous pulley preservation, precise biomechanical tensioning, and disciplined postoperative rehabilitation, the orthopedic surgeon can achieve excellent functional outcomes and restore the critical pinch and grasp capabilities of the human hand.
📚 Medical References
- Flexor tendon graft for late management of isolated rupture of the profundus tendon, J Trauma 43:103, 1997.
- McClinton MA, Curtis RM, Wilgis EFS: One hundred tendon grafts for isolated fl exor digitorum profundus injuries, J Hand Surg 7:224, 1982.
- Naam NH: Staged fl exor tendon reconstruction using pedicled tendon graft from the fl exor digitorum superfi cialis, J Hand Surg 22A:323, 1997.
- Pulvertaft RG: Tendon grafts for fl exor tendon injuries in the fi ngers and thumb: a study of technique and results, J Bone Joint Surg 38B:175, 1956.
- Pulvertaft RG: The treatment of profundus division by free tendon graft, J Bone Joint Surg 42A:1363, 1960.
- Rozmaryn LM: Tendon graft reconstruction of the extensor hood defi cits with subluxation, J Hand Surg 20A:841, 1995.
- Sakellarides HT, Papadopoulos G: Surgical treatment of the divided fl exor digitorum profundus tendon in zone 2, delayed more than 6 weeks, by tendon grafting in 50 cases, J Hand Surg 21B:63, 1996.
- Schlenker JD: Infection following pulp pull-through technique of fl exor tendon grafting, J Hand Surg 6A:550, 1981.
- Schneider LH: Staged fl exor tendon reconstruction using the method of Hunter, Clin Orthop Relat Res 171:164, 1982.
- Schneider LH: Staged tendon reconstruction, Hand Clin 1:109, 1985.
- Silfverskiöld KL, May EJ: Early active mobilization of tendon grafts using mesh reinforced suture techniques, J Hand Surg 20B:301, 1995.
- Stark HH, Anderson DR, Zelem NP, et al: Bridge fl exor tendon grafts, Clin Orthop Relat Res 242:51, 1989.
- Stark HH, Zemel NP, Boyes JH, et al: Flexor tendon graft through intact superfi cialis tendon, J Hand Surg 2A:456, 1977.
- Tang JB, Zhang QG, Ishii S: Autogenous free sheath grafts in reconstruction of injured digital fl exor tendon sheath at the delayed primary stage, J Hand Surg 18B:31, 1993.
- Urbaniak JR, Goldner JL: Laceration of the fl exor pollicis longus tendon: delayed repair by advancement, free graft or direct suture: a clinical and experimental study, J Bone Joint Surg 55A:1123, 1973.
- Watanabe T, Iwasawa M, Kushima H, et al: Free temporal fascial fl ap for coverage and extensor tendon reconstruction, Ann Plast Surg 37:469, 1996.
- Wehbé MA: Tendon graft donor sites, J Hand Surg 17A:1130, 1992.
- White WL: Tendon grafts: a consideration of their source, procurement, and suitability, Surg Clin North Am 40:403, 1960.
- White WL: The unique, accessible and useful plantaris tendon, Plast Reconstr Surg 25:133, 1960.
You Might Also Like