Mastering the Surgical Management of Pyogenic Flexor Tenosynovitis
Key Takeaway
Pyogenic flexor tenosynovitis is a rapidly progressive orthopedic emergency threatening hand function. Diagnosis relies on Kanavel’s four cardinal signs: fusiform swelling, resting flexed posture, pain on passive extension, and tenderness along the flexor sheath. Prompt surgical intervention via closed catheter irrigation or open drainage is critical to decompress the sheath, prevent tendon necrosis from elevated pressures, and eradicate infection, followed by aggressive early rehabilitation.
Introduction to Pyogenic Flexor Tenosynovitis
Pyogenic flexor tenosynovitis (PFT) represents a rapidly progressive, limb-threatening orthopedic emergency characterized by a closed-space bacterial infection within the synovial sheath of the flexor tendons. Most commonly, this condition arises from direct inoculation via puncture wounds in the flexor creases or through the contiguous spread of adjacent pulp space infections (felons).
Because the flexor tendon relies heavily on synovial fluid diffusion for nutrition, the accumulation of purulent exudate not only incites a severe inflammatory response but also drastically increases intrasheath pressure. Without prompt recognition and aggressive surgical intervention, the resulting ischemia and enzymatic degradation inevitably lead to tendon necrosis, dense adhesion formation, profound joint stiffness, and catastrophic loss of hand function.
Clinical Pearl: Time is tissue in pyogenic flexor tenosynovitis. If non-operative management (intravenous antibiotics and splinting) does not yield significant clinical improvement within 12 to 24 hours, or if the patient presents with symptoms lasting longer than 48 hours, immediate surgical decompression and irrigation are mandatory.
Surgical Anatomy and Pathomechanics
To effectively manage flexor tenosynovitis, the orthopedic surgeon must possess an intimate understanding of the flexor sheath anatomy and its biomechanical vulnerabilities.
The Synovial Sheath and Bursal Anatomy
The flexor tendon sheath is a double-walled, closed synovial cylinder that facilitates frictionless tendon gliding.
* Digits II, III, and IV: The synovial sheaths typically begin at the level of the metacarpal neck (proximal to the A1 pulley) and terminate at the insertion of the flexor digitorum profundus (FDP) at the distal phalanx.
* Digit I (Thumb) and Digit V (Small Finger): The flexor pollicis longus (FPL) sheath routinely communicates proximally with the radial bursa. The small finger flexor sheath communicates with the ulnar bursa.
* The Space of Parona: The radial and ulnar bursae frequently communicate with each other in the proximal palm and distal forearm, creating a potential conduit for a "horseshoe abscess" that can spread rapidly across the hand and into the deep fascial spaces of the forearm (Space of Parona).
Pathophysiology of Tendon Ischemia
The flexor tendons receive their blood supply via the segmental vincula (breve and longa) and through passive diffusion from the synovial fluid.
In the presence of infection, bacterial proliferation and the host's purulent inflammatory response rapidly increase the volume of fluid within the unyielding retinacular pulley system. Research by Schnall et al. demonstrated that pressures within the infected flexor sheath can easily exceed 30 mm Hg. This elevated pressure surpasses the capillary perfusion pressure of the vincula, rendering the tendons acutely ischemic. Concurrently, bacterial exotoxins and host-derived matrix metalloproteinases (MMPs) actively degrade the collagenous architecture of the tendon, predisposing it to spontaneous rupture.
Clinical Evaluation and Diagnosis
The diagnosis of pyogenic flexor tenosynovitis is primarily clinical, relying heavily on the classic criteria described by Allen B. Kanavel in 1912.
Kanavel’s Four Cardinal Signs
- Tenderness along the Flexor Sheath: Exquisite tenderness elicited by palpation directly over the anatomic course of the flexor sheath. This is widely considered the most significant and earliest sign.
- Fusiform Swelling: Symmetrical, uniform swelling of the entire digit, often described as a "sausage digit," distinguishing it from localized abscesses.
- Pain on Passive Extension: Severe pain elicited by passive extension of the digit. This stretches the inflamed visceral and parietal layers of the tenosynovium.
- Flexed Resting Posture: The digit is held in a rigid, slightly flexed position to maximize the volume of the flexor sheath and minimize intrasheath pressure and pain.
Surgical Warning: Purulent fluid might not always be present in the flexor sheath, especially in early presentations with overlying cellulitis. Needle aspiration of the sheath through cellulitic tissue carries a high risk of iatrogenically inoculating a sterile sheath with bacteria. Aspiration should be reserved for the operating room under direct visualization.
Microbiology and Antimicrobial Management
Empiric antibiotic therapy must be initiated immediately upon suspicion of PFT, following appropriate blood and wound cultures.
- Staphylococcus aureus: The most frequently isolated pathogen, particularly following penetrating trauma. Methicillin-resistant S. aureus (MRSA) must be covered empirically in endemic areas.
- Streptococcus species: Commonly seen in conjunction with S. aureus or following human bites.
- Gram-Negative Organisms: Pseudomonas aeruginosa and other gram-negative bacilli may be present, particularly in immunocompromised patients, intravenous drug users, or following exposure to contaminated water.
- Mixed Flora: Animal bites (e.g., Pasteurella multocida from cats/dogs) or human bites (Eikenella corrodens) require specific coverage.
Antibiotic Resistance: Historical data from urban trauma centers (e.g., Cook County Hospital) demonstrate significant resistance to Penicillin G and Cefazolin (up to 16.2%). Therefore, empiric therapy often involves Vancomycin (for MRSA and resistant gram-positives) combined with a broad-spectrum agent like Ciprofloxacin or a third-generation cephalosporin for gram-negative coverage.
Indications for Surgical Intervention
While early tenosynovitis (symptoms < 48 hours) may occasionally be aborted with aggressive intravenous antibiotics and strict elevation/splinting, surgical intervention is the gold standard for the vast majority of cases.
Absolute Indications for Surgery:
* Presence of gross pus upon aspiration or clinical examination.
* Failure to improve clinically after 12 to 24 hours of targeted intravenous antibiotic therapy.
* Delayed presentation (symptoms present for > 48 hours).
* Signs of systemic toxicity, compartment syndrome, or impending tendon necrosis.
Surgical Technique: Closed Postoperative Irrigation (Modified Neviaser Technique)
Popularized by Neviaser and supported by the foundational work of Carter, Burman, and Mersheimer, closed catheter irrigation is highly effective for acute infections yielding serous exudate or frank purulent fluid. Gutowski et al. demonstrated that closed catheter irrigation is as effective as open drainage, with the added benefit of reduced postoperative morbidity and faster rehabilitation.
Preoperative Preparation and Positioning
- Anesthesia: General anesthesia or a regional brachial plexus block is preferred. Local infiltration directly into the infected digit is contraindicated due to the risk of spreading the infection and the ineffectiveness of local anesthetics in acidic, infected tissues.
- Tourniquet: Apply a pneumatic tourniquet to the proximal arm.
- CRITICAL STEP: Elevate the arm for gravity exsanguination for 3 minutes prior to inflation. Do not wrap the limb with an Esmarch bandage, as the mechanical compression can force purulent material proximally into the palmar spaces or forearm.
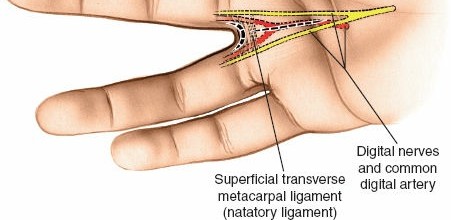
Incision Planning and Proximal Exposure
Depending on the digit involved and the surgeon's preference, several palmar incisions can be utilized to access the proximal flexor sheath (A1 pulley region).
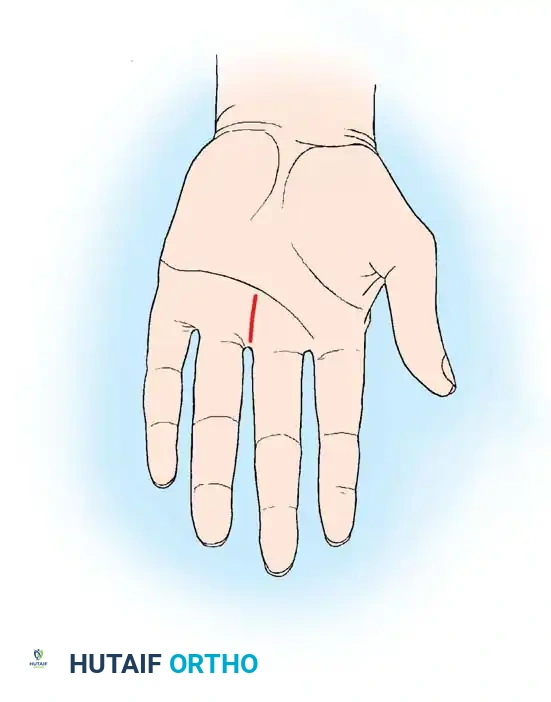
Fig. 1: Distal longitudinal palmar incision.
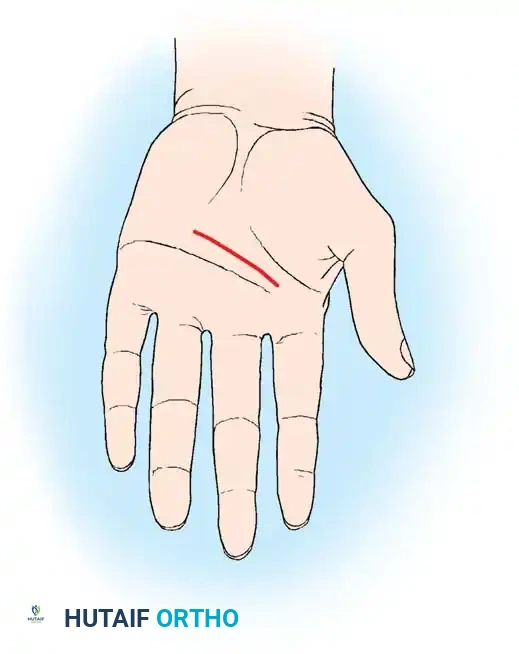
Fig. 2: Transverse palmar incision.
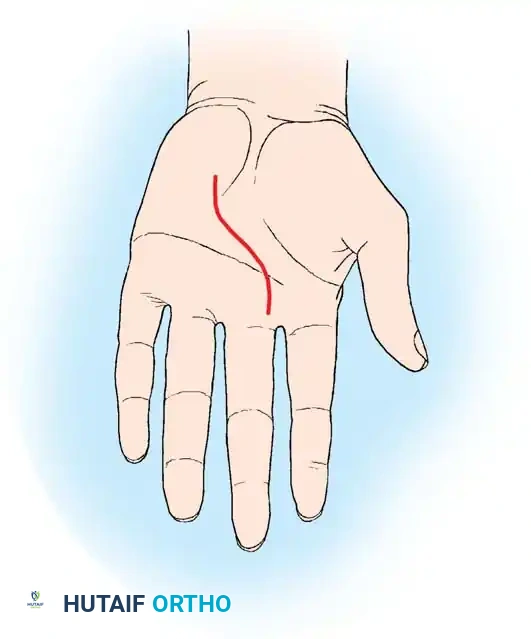
Fig. 3: Extended longitudinal palmar incision.
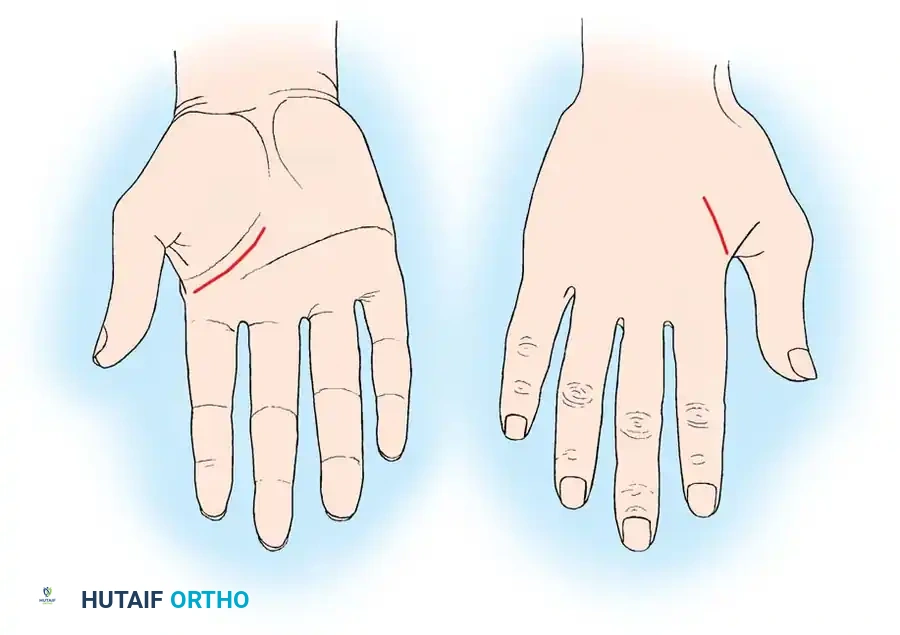
Fig. 4: A, Thenar crease incision (palmar) for thumb involvement. B, Dorsal longitudinal incision.
- Expose the proximal end of the flexor sheath in the region of the A1 pulley using a straight transverse incision parallel to the distal palmar crease, or a zigzag Brunner incision.
- Carefully dissect through the subcutaneous tissue, protecting the neurovascular bundles.
- Identify the A1 pulley. Expect to encounter serosanguineous or frank purulent fluid upon exposing the sheath.
- Open the sheath just proximal to the A1 pulley. Immediately swab the fluid or aspirate it for Gram stain, aerobic, anaerobic, and mycobacterial cultures.
Distal Exposure and Catheter Placement
- Make a second incision in the midaxial line on either side of the finger in the distal portion of the middle phalanx. Alternatively, a careful transverse incision over the distal interphalangeal (DIP) flexion crease can be utilized.
- Identify and open the flexor sheath distal to the A4 pulley.
- Using smooth forceps or a hemostat, gently pass a 16-gauge or 18-gauge polyethylene catheter (or a pediatric feeding tube) beneath the A1 pulley, directing it from proximal to distal within the flexor sheath for approximately 1.5 to 2 cm.
- Distally, place a small piece of a Penrose rubber drain beneath the A4 pulley and bring it out through the distal skin incision to maintain patency for outflow.
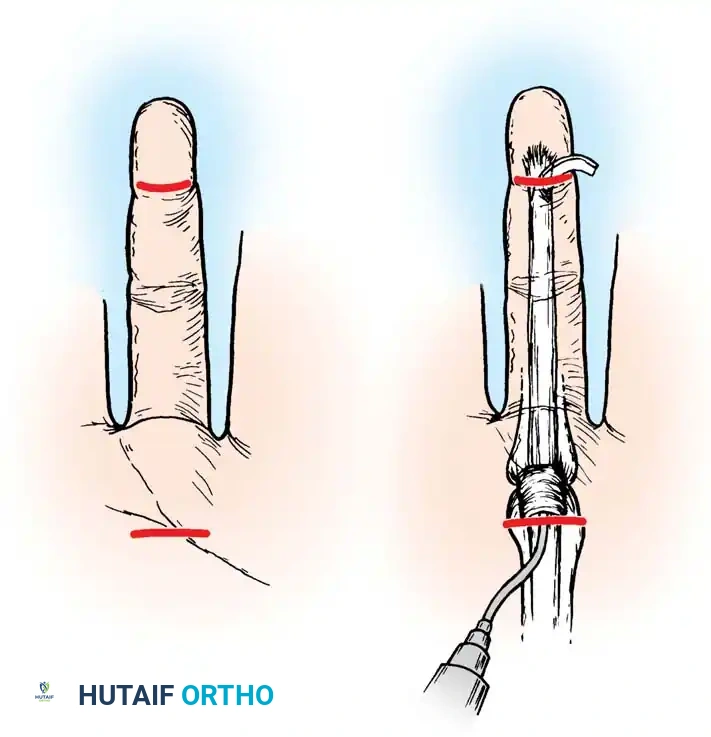
Fig. 5: Closed irrigation setup demonstrating proximal catheter inflow and distal drain outflow.
Irrigation and Closure
- Copiously irrigate the sheath from proximal to distal with sterile normal saline. Ensure clear, unobstructed outflow from the distal drain.
- Close the proximal wound loosely around the catheter. Suture the catheter securely to the palmar skin using a non-absorbable suture (e.g., 3-0 Nylon) to prevent accidental dislodgement.
- Leave the distal wound sufficiently loose around the rubber drain to allow unimpeded fluid egress.
- Test the system for patency by flushing with 10-20 mL of saline.
- Apply a bulky, non-compressive hand dressing supported by a volar resting splint. Leave the tip of the distal rubber drain exposed to monitor outflow.
- Attach the proximal inflow catheter to a 30-mL syringe or an automated irrigation pump.
Surgical Pearl - Radial and Ulnar Bursae Involvement: If the infection involves the thumb or small finger, suspect bursal extension. Place a second catheter in the palmar wound and pass it proximally. Open the respective bursa proximally through a longitudinal incision on the radial or ulnar aspect of the distal forearm (proximal to the wrist crease). Place a drain in the forearm wound and irrigate in both proximal and distal directions.
Surgical Technique: Open Drainage and Debridement
Open drainage is reserved for chronic infections, delayed presentations, or cases where intraoperative inspection reveals gross necrosis of the flexor tendon and extensive destruction of the tenosynovium requiring aggressive debridement.
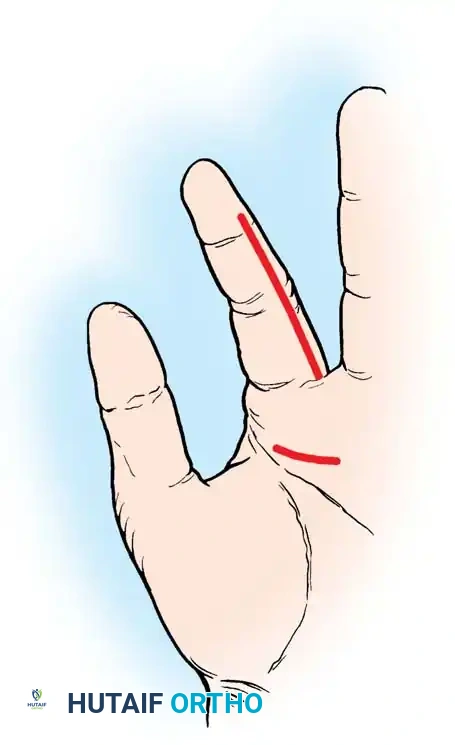
Fig. 6: Open drainage utilizing a midaxial incision for advanced infection and tendon necrosis.
The Midaxial Approach
- Under appropriate anesthesia and tourniquet control (gravity exsanguination only), mark a midaxial line on the affected digit. This line connects the apices of the flexion creases on the lateral aspect of the digit.
- Make a longitudinal midaxial incision extending from the distal flexion crease proximally toward the web space.
- Critical Anatomy: Deepen the incision, ensuring the dissection remains strictly dorsal to the neurovascular bundle. Divide Cleland's ligaments (dorsal to the NV bundle) to mobilize the skin flap volarly, carrying the digital artery and nerve safely with the volar flap.
- Make a second, separate incision in the palm, parallel to the distal palmar crease, over the A1 pulley.
- Identify the flexor sheath in the distal wound. Open the sheath extensively, specifically targeting the thinner cruciform pulleys (C1, C2, C3) while meticulously attempting to preserve the critical annular pulleys (A2 and A4) to prevent postoperative tendon bowstringing.
- Obtain deep tissue and fluid specimens for culture.
- Perform a radical tenosynovectomy, debriding all necrotic, fibrinous, and infected tenosynovium. If the tendon itself is frankly necrotic and non-viable, a staged tendon reconstruction (e.g., Hunter rod placement) may eventually be required, though the primary goal is infection eradication.
- Irrigate copiously from the proximal palmar wound distally.
- Do not close the wounds. Leave them open to heal by secondary intention or for delayed primary closure. Apply a bulky, absorbent dressing and a volar splint.
Postoperative Protocols and Rehabilitation
The success of surgical intervention hinges on meticulous postoperative care and aggressive rehabilitation to prevent crippling adhesions.
Irrigation Protocol (Closed Technique)
- Irrigate the proximal catheter with 20 to 30 mL of sterile normal saline every 2 to 4 hours.
- Continuously monitor the distal wound for catheter patency and unobstructed outflow. If outflow ceases, the system must be flushed or adjusted immediately to prevent fluid accumulation and recurrent pressure elevation.
- Note: Lille et al. found no statistically significant difference in long-term outcomes between patients receiving only massive intraoperative irrigation versus those receiving continuous postoperative irrigation for 24-48 hours, provided the initial decompression was adequate. However, postoperative irrigation remains a standard safeguard in many institutions.
Wound Care and Mobilization
- At 48 Hours: Remove the bulky dressing and inspect the digit.
- If clinical signs of infection (erythema, swelling, purulent drainage) have resolved, remove the catheter and the distal drain. Apply a light dressing.
- If signs of persistent infection remain, continue irrigation for an additional 24 hours and reassess.
- Rehabilitation: Initiate active and active-assisted range of motion (ROM) exercises immediately upon catheter removal (or within 36-48 hours for open drainage).
- For open drainage cases, institute daily or twice-daily whirlpool treatments to facilitate mechanical debridement of the open wounds, encouraging active motion during the hydrotherapy sessions.
- Prolonged splinting is strictly contraindicated once the acute infection is cleared, as it guarantees dense adhesion formation and permanent loss of digital excursion.
By adhering to these rigorous diagnostic criteria and executing precise, timely surgical decompression, the orthopedic surgeon can successfully eradicate pyogenic flexor tenosynovitis and restore optimal function to the critically threatened hand.
You Might Also Like