Operative Management of Acute and Chronic Paronychia
Key Takeaway
Paronychia is a common perionychial infection typically caused by Staphylococcus aureus. Acute presentations require prompt incision and drainage, often with partial nail plate excision, to prevent nail bed damage or osteomyelitis. Chronic paronychia, frequently a multifactorial inflammatory dermatitis, may necessitate eponychial marsupialization for recalcitrant cases. Accurate diagnosis is critical to differentiate bacterial paronychia from herpetic whitlow, which strictly contraindicates surgical intervention.
Introduction to Perionychial Infections
Infections of the hand and fingertips are among the most common pathologies encountered by orthopedic surgeons and hand specialists. Among these, paronychia represents the most frequent infection of the hand. The perionychium comprises the paronychial folds (lateral nail folds), the eponychium (proximal nail fold), the hyponychium (distal nail bed), and the nail bed itself, which is subdivided into the proximal germinal matrix and the distal sterile matrix.
A paronychia is defined as an inflammatory or infectious process affecting the soft-tissue fold around the fingernail. Depending on the duration, etiology, and clinical presentation, paronychia is broadly classified into acute and chronic forms. Understanding the precise anatomical relationships and the underlying pathophysiology is paramount, as improper surgical technique can lead to permanent nail dystrophy, chronic pain, or deep space infections such as a felon or osteomyelitis of the distal phalanx.
Acute Paronychia
Pathophysiology and Microbiology
Acute paronychia typically results from minor mechanical trauma to the perionychium, such as nail biting, aggressive manicuring, or the avulsion of a "hangnail." This microtrauma disrupts the protective seal between the nail plate and the eponychium, allowing direct inoculation of skin flora into the closed perionychial space.
Staphylococcus aureus is the most frequently isolated pathogen. However, in cases associated with nail-biting or oral contact, mixed flora including Streptococcus species, Eikenella corrodens, and anaerobic bacteria (such as Bacteroides or Fusobacterium) may be present.
The infection typically begins at one corner of the horny nail fold as a localized cellulitis. If left untreated, it rapidly progresses to abscess formation. The purulence can track proximally under the eponychium or transversely across the nail root to the contralateral side, creating a classic "runaround" infection. In severe cases, the abscess may decompress beneath the nail plate, separating it from the sterile or germinal matrix.
Clinical Evaluation
Patients present with acute onset of throbbing pain, erythema, and tense swelling of the lateral or proximal nail folds. Palpation reveals exquisite tenderness, and a localized collection of purulence is often visible beneath the translucent eponychial skin.
🚨 Surgical Warning: The Felon Extension
Untreated acute paronychia can extend volarly into the digital pulp, resulting in a felon. The pulp abscess can penetrate the periosteum, causing osteomyelitis of the distal phalanx, or track proximally through the fibrous septa into the flexor tendon sheath, precipitating acute suppurative flexor tenosynovitis. Severe, throbbing pain lasting longer than 12 hours with volar pulp tension strongly suggests felon formation, necessitating simultaneous volar drainage.
Differential Diagnosis: Herpetic Whitlow
Before proceeding with any surgical intervention, the surgeon must definitively rule out Herpetic Whitlow, an infection caused by Herpes Simplex Virus (HSV) type 1 or 2.
Herpetic whitlow is an occupational hazard frequently seen in healthcare workers (dental hygienists, respiratory therapists) and immunocompromised patients. It presents as a localized area of swelling characterized by the eruption of clear, coalescing vesicles on an erythematous base. Unlike bacterial paronychia, the fluid within these vesicles is initially clear, though it may become cloudy later. Lymphangitis and epitrochlear or axillary lymphadenopathy are commonly associated.
Diagnostic Confirmation:
* Tzanck Smear: Reveals multinucleated giant cells.
* Viral Culture/PCR: Confirms HSV DNA from vesicular fluid.
* Serum Antibody Titers: Useful for establishing primary vs. recurrent infection.
🛑 Pitfall: Incising a Herpetic Whitlow
Herpetic whitlow is a strictly self-limiting condition, typically resolving over 3 to 4 weeks. Surgical incision and drainage is absolutely contraindicated. Incising a herpetic lesion does not relieve pain; rather, it risks secondary bacterial superinfection, delayed healing, and potential systemic dissemination of the virus. Management consists of dry dressings, oral antivirals (e.g., acyclovir or valacyclovir) if initiated early, and observation.
Surgical Management of Acute Paronychia
When an abscess has formed in the eponychial or paronychial fold, surgical incision and drainage (I&D) is the definitive treatment. The surgical approach is dictated by the extent of the abscess.
Indications
- Visible purulence in the paronychial fold.
- Fluctuance upon palpation.
- Failure of conservative management (warm soaks, oral antibiotics) after 24-48 hours.
Surgical Technique: Incision and Drainage
- Anesthesia and Preparation: Administer a digital block using 1% lidocaine or 0.5% bupivacaine without epinephrine. Ensure profound anesthesia before proceeding. Cleanse the digit with a chlorhexidine or povidone-iodine solution and drape in a sterile fashion. A digital tourniquet (e.g., a sterile Penrose drain) may be applied at the base of the finger for a bloodless field.
- Unilateral Paronychial Abscess: If the abscess is confined to one lateral fold, use a #11 scalpel blade to elevate the eponychial fold away from the nail plate. The blade must be kept parallel to the nail plate and angled away from the nail bed.
- Pearl: Never direct the blade volarly into the nail bed. Iatrogenic injury to the germinal matrix will result in permanent longitudinal ridging or deformity of the nail plate.
- Subungual Extension: If the purulence extends beneath one corner of the nail root, the floating, undermined portion of the nail must be excised. Use straight iris scissors to longitudinally split the lateral quarter of the nail plate, and gently avulse it with a hemostat.
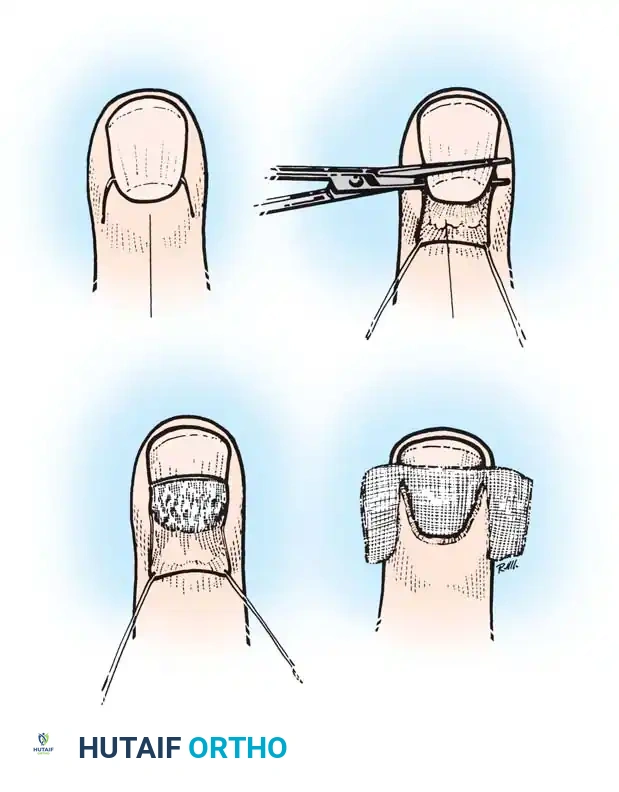
- The "Runaround" Infection: If the infection has migrated to the opposite side and under the proximal nail fold, a more extensive approach is required.
- Make two parallel longitudinal incisions at the junction of the lateral nail folds and the eponychium.
- Fold the eponychial skin flap back proximally to expose the entire nail root.
- Excise the proximal one-third of the nail plate to ensure complete decompression of the germinal matrix.
- Wound Management: Irrigate the cavity copiously with sterile saline. Loosely pack the wound with iodoform gauze or a small wick to stent the eponychial fold open, ensuring continuous drainage for the first 48 hours.
Postoperative Protocol for Acute Paronychia
- Day 0-2: The digit is dressed in a bulky, non-compressive dressing. The patient is instructed to keep the hand elevated above heart level to minimize throbbing and edema.
- Day 2: The iodoform packing is removed in the clinic.
- Day 3 Onward: The patient begins warm water and chlorhexidine (Hibiclens) or hydrogen peroxide soaks three times daily.
- Antibiotic Therapy: While I&D is the primary treatment, a short course of oral antibiotics (e.g., cephalexin, dicloxacillin, or clindamycin/trimethoprim-sulfamethoxazole if MRSA is suspected) is prescribed for 5-7 days, particularly if surrounding cellulitis is present.
Chronic Paronychia
Etiology and Pathogenesis
Unlike its acute counterpart, chronic paronychia is rarely a primary bacterial infection. It is more accurately classified as a multifactorial inflammatory dermatitis of the perionychium. It typically occurs in patients whose occupations require prolonged, repetitive exposure to water, harsh chemicals, or alkaline irritants (e.g., dishwashers, bartenders, florists, and healthcare workers).
The chronic moisture leads to the maceration and eventual loss of the cuticle, which serves as the primary mechanical barrier between the nail plate and the eponychium. The loss of this seal allows irritants and opportunistic organisms to colonize the potential space.
Microbiology and Medical Management
Cultures from chronic paronychial lesions frequently yield a mixed flora, including Staphylococcus pyogenes, Staphylococcus epidermidis, colonic gram-negative bacteria, and most notably, Candida albicans.
Historically, chronic paronychia was treated primarily as a fungal infection. However, contemporary evidence suggests that the fungal presence is often secondary colonization rather than the primary driver of the disease. A landmark study by Tosti et al. compared the efficacy of topical methylprednisolone against two oral antifungal agents (terbinafine and itraconazole) in 45 patients with multiple nail involvement.
* Topical Methylprednisolone: Cured or improved 85% of the affected nails.
* Oral Terbinafine: Effective in 52%.
* Oral Itraconazole: Effective in 45%.
These findings strongly support the paradigm that chronic paronychia is primarily an eczematous dermatitis related to environmental exposure. Therefore, first-line management consists of strict avoidance of moisture (using cotton-lined rubber gloves), application of high-potency topical corticosteroids, and topical antifungals.
Surgical Management: Eponychial Marsupialization
When conservative measures and prolonged medical therapy fail, surgical intervention is indicated. The eponychial marsupialization technique, originally described by Keyser and Eaton and later modified by Bednar and Lane, is the gold standard for recalcitrant chronic paronychia.
The goal of marsupialization is to excise the fibrotic, chronically inflamed tissue of the eponychial fold, thereby decompressing the nail matrix and allowing a new, healthy epithelial barrier to regenerate. Bednar and Lane noted that if concurrent nail irregularities (such as severe transverse ridging or dystrophy) are present, simultaneous removal of the nail plate significantly improves healing rates and prevents recurrence.
🔪 Surgical Technique 75-2: Eponychial Marsupialization
1. Preparation and Anesthesia
* Administer a standard digital block anesthetic using a long-acting agent such as 0.5% bupivacaine to provide extended postoperative pain relief.
* Thoroughly cleanse the entire finger and hand with an appropriate surgical antiseptic (chlorhexidine gluconate or povidone-iodine).
* Drape the hand in a standard sterile fashion. Apply a digital tourniquet to ensure precise visualization of the eponychial microanatomy.
2. The Marsupialization Incision
* Identify the proximal extent of the eponychial fold.
* Using a #15 scalpel blade, excise a crescent-shaped wedge of skin, approximately 3 mm wide, parallel to the curve of the eponychium.
* This crescentic excision must extend fully from the radial border to the ulnar border of the nail fold. The widest portion of the crescent should be at the dorsal midline of the digit.
3. Tissue Resection (Keyser/Eaton vs. Bednar/Lane)
* Keyser and Eaton Approach: Deepen the incision to remove all thickened, fibrotic, and chronically inflamed tissue down to the level of the germinal matrix.
* Bednar and Lane Modification: Carefully excise the skin but leave the underlying subcutaneous fat intact. This modification is believed to protect the delicate germinal matrix from iatrogenic injury while still effectively marsupializing the fold.
4. Nail Plate Management
* Critically evaluate the nail plate. If the nail exhibits significant irregularities, thickening, or detachment, it acts as a nidus for ongoing fungal colonization.
* In such cases, use a Freer elevator or straight hemostat to gently separate the nail plate from the sterile and germinal matrices, and completely avulse the nail.
5. Wound Dressing
* The marsupialized defect is left open to heal by secondary intention; it is never primarily closed.
* Cover the exposed wound bed with a non-adherent, petroleum-bismuth tribromophenate–impregnated gauze (Xeroform).
* If the nail plate was removed, carefully tuck a single layer of this Xeroform gauze beneath the newly marsupialized proximal nail fold to prevent synechiae (adhesions) between the dorsal roof and the germinal matrix.
Postoperative Rehabilitation and Aftertreatment
The postoperative care following eponychial marsupialization is intensive and requires high patient compliance to ensure optimal outcomes and prevent premature closure of the fold.
- Initial Medications: Oral antibiotics (such as cephalexin or erythromycin) are initiated immediately postoperatively to prevent secondary bacterial infection of the open wound bed.
- Wound Care Protocol: The initial surgical dressing remains in place for 48 to 72 hours. Beginning on postoperative day 3, the patient is instructed to remove the dressing and commence a rigorous soaking regimen.
- Soaking Regimen: The affected finger must be soaked in a dilute solution of hydrogen peroxide and washed gently with a chlorhexidine gluconate skin cleanser (Hibiclens) three times daily.
- Duration of Care: These daily washings and soaks are continued meticulously until all purulent or serous drainage ceases and the wound bed demonstrates healthy granulation tissue.
- Antibiotic Duration: Antibiotics are generally continued for a full 2 weeks. However, if intraoperative tissue cultures return negative for bacterial growth, the antibiotic regimen can be safely discontinued in 3 to 5 days to prevent antimicrobial resistance.
- Long-Term Follow-Up: The marsupialized defect will epithelialize over 3 to 6 weeks. If the nail was removed, a new, healthy nail plate will take approximately 4 to 6 months to fully regenerate from the germinal matrix to the hyponychium. Patients must be counseled to strictly avoid environmental moisture and irritants during this entire regenerative phase.
You Might Also Like
