Mastering Excision of Hand & Wrist Ganglion Cysts & Related Soft Tissue Tumors

Key Takeaway
Step into the operating room for a comprehensive masterclass on excising hand and wrist soft tissue tumors. This guide covers the meticulous surgical techniques for ganglion cysts, giant cell tumors of the tendon sheath, and epidermal inclusion cysts. Fellows will learn critical anatomy, precise instrument use, and strategies for managing potential complications, ensuring a thorough understanding of these common procedures from a seasoned surgeon's perspective.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of soft tissue tumors of the hand and wrist represents a foundational pillar of orthopedic hand surgery. While often erroneously dismissed as trivial "lumps and bumps" by the uninitiated, these lesions demand meticulous attention to anatomical detail, precise microscopic dissection, and a profound understanding of their unique pathophysiologies. An inadequate excision not only guarantees recurrence but places critical neurovascular and tendinous structures at profound risk. This chapter provides an exhaustive, master-level exposition on the excision of the most ubiquitous soft tissue lesions encountered in clinical practice: ganglion cysts, giant cell tumors of the tendon sheath (GCTTS), and epidermal inclusion cysts (EIC).
Before a surgical blade addresses the dermis, the operating surgeon must possess a granular understanding of the pathology being addressed. Ganglion cysts represent the most prevalent soft tissue tumor of the hand and wrist, comprising approximately 60% to 70% of all such lesions. By definition, a ganglion is a benign, mucin-filled pseudocyst. Unlike true cysts, ganglions lack a true epithelial or synovial lining; rather, they are encapsulated by a dense, fibrous pseudocapsule composed of compressed connective tissue. The internal fluid is a highly viscous, clear, jelly-like mucinous substance characterized by elevated concentrations of hyaluronic acid, glucosamine, albumin, and globulin. Clinically, these present as fluctuant, transilluminating masses that often vary in size, a phenomenon attributed to a micro-valvular mechanism at the capsular stalk that permits fluid ingress while restricting egress.

The pathogenesis of ganglion cysts remains a subject of academic debate, though the contemporary consensus heavily favors the "capsular rent" or "micro-trauma" theory. Chronic, repetitive biomechanical stress at the synovial-capsular interface—particularly at the scapholunate articulation for dorsal cysts and the radioscaphoid articulation for volar cysts—stimulates local mesenchymal and fibroblast cells to undergo mucoid degeneration and produce excess hyaluronic acid. This mucin dissects through the capsular and ligamentous planes, coalescing into the main cystic structure. Degenerative mucous cysts, a specific subtype of ganglion arising at the distal interphalangeal (DIP) joint, share this mucinous etiology but are inexorably linked to underlying osteoarthritis and marginal osteophyte formation.

Conversely, Giant Cell Tumors of the Tendon Sheath (GCTTS)—also referred to in the literature as localized nodular tenosynovitis—are solid, benign, slow-growing neoplasms. As the second most common tumor of the hand, they require a fundamentally different surgical mindset. Grossly, GCTTS present as firm, multilobulated, well-circumscribed masses ranging in color from pale yellow to deep mahogany, dictated by their internal concentrations of hemosiderin-laden macrophages, histiocytes, and collagen. Histologically, they are characterized by mononuclear cells, multinucleated osteoclast-like giant cells, and foam cells. While benign, their clinical behavior can be locally aggressive; they possess a distinct propensity to intimately envelop digital neurovascular bundles and erode into adjacent cortical bone, necessitating meticulous, magnification-assisted dissection to achieve complete en bloc resection without inducing iatrogenic morbidity.

Epidermal Inclusion Cysts (EIC) represent the third most common soft tissue tumor in the hand and are uniquely distinguished by their traumatic etiology. These are true cysts, lined by stratified squamous epithelium and filled with thick, white, malodorous keratinaceous debris. The pathogenesis is universally linked to a prior penetrating trauma—such as a laceration, puncture wound, or traumatic amputation—which drives surface epithelial cells deep into the subcutaneous tissues or intraosseous spaces. Over months to years, these implanted cells continue to proliferate and desquamate keratin, expanding the cyst. When located in the distal phalanx, they can cause significant lytic bone destruction and compromise the overlying nail matrix, demanding careful surgical planning to eradicate the cyst lining entirely while preserving the structural integrity of the digit.

Ganglion Cysts
Ganglion cysts are the quintessential manifestation of capsular and synovial stress in the upper extremity. As previously noted, their defining characteristic is the absence of a cellular lining, making them pseudocysts. The mucin within is highly concentrated, leading to its characteristic high viscosity. This viscosity is a critical diagnostic feature; during fine-needle aspiration, the fluid is often too thick to be easily drawn through a standard 22-gauge needle, requiring a larger bore. The multilobulated nature of many ganglions further complicates aspiration, as draining a single loculation rarely decompresses the entire mass, explaining the historically high recurrence rates associated with non-operative management.

Clinically, patients typically present with a mass that has been present for weeks to years, often reporting that the lesion waxes and wanes in size. This fluctuation is directly correlated with activity levels; vigorous use of the affected joint acts as a mechanical pump, driving synovial fluid through the one-way stalk valve into the cyst. During periods of rest, the water content of the mucin is slowly resorbed into the surrounding tissues, leading to a decrease in palpable size. Pain, when present, is classically described as a deep, dull ache exacerbated by extreme ranges of motion, such as terminal wrist extension in the case of dorsal wrist ganglions.

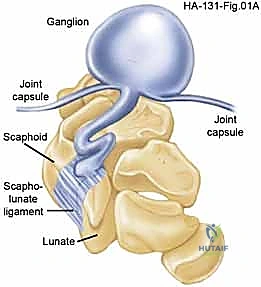
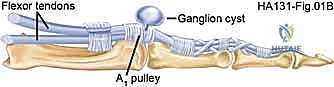
The anatomical distribution of ganglion cysts dictates the surgical approach and the specific neurovascular structures at risk. Dorsal wrist ganglions, comprising the vast majority, nearly universally originate from the dorsal aspect of the scapholunate interosseous ligament. Volar wrist ganglions, the second most common variant, typically arise from the radioscaphoid or scaphotrapezial joints and are intimately associated with the radial artery. Volar retinacular cysts arise from the A1 or A2 pulleys of the flexor tendon sheath and present as firm, tender nodules in the palm, often mimicking the initial stages of stenosing tenosynovitis (trigger finger).
Giant Cell Tumors of the Tendon Sheath
Giant Cell Tumors of the Tendon Sheath present a distinct diagnostic and surgical challenge. Unlike the fluctuant, transilluminating ganglion cyst, a GCTTS is a firm, non-compressible, and non-transilluminating mass. Patients typically present in their fourth to sixth decades, noting a very slow-growing, painless nodule, most frequently located on the volar aspect of the radial three digits. Because these tumors grow insidiously, they can reach substantial sizes before the patient seeks medical attention, often only presenting when the mass mechanically impedes digital flexion or causes pressure-related neuropathy by compressing the adjacent digital nerve.

The local invasiveness of GCTTS is its most clinically relevant characteristic. While histologically benign and devoid of metastatic potential, these tumors exhibit a relentless expansile growth pattern. They frequently track along the path of least resistance, which in the tightly compartmentalized digit means they dissect between the flexor tendon sheath and the neurovascular bundles. It is not uncommon during surgical exploration to find the tumor completely encircling a digital nerve or artery, necessitating painstaking micro-dissection to peel the tumor off the perineurium or adventitia.
Furthermore, longstanding GCTTS can induce pressure necrosis and remodeling of the adjacent cortical bone, a phenomenon visible on pre-operative radiographs as a well-corticated, "saucerized" lytic defect. Unlike malignant lesions, they do not typically breach the cortex to invade the medullary canal, nor do they destroy articular cartilage. However, the presence of bone erosion complicates excision, as tumor cells may be harbored within the bony defect. A thorough curettage of any associated bony crater is mandatory to minimize the risk of local recurrence, which historically ranges from 10% to 20% even in expert hands.
Epidermal Inclusion Cysts
Epidermal Inclusion Cysts are a fascinating testament to the regenerative capacity of displaced epithelial tissue. The sine qua non of an EIC is a history of penetrating trauma, though patients may occasionally have forgotten the inciting event if it occurred years prior. The classic demographic is a manual laborer or individual with a history of a crush injury, laceration, or surgical amputation. The traumatic event drives basal epithelial cells into the deeper dermal, subcutaneous, or even intraosseous layers. Separated from their normal surface environment, these cells form a spherical cyst, continuing their normal lifecycle of maturation and desquamation, shedding keratin into the enclosed central cavity.
Clinically, an EIC presents as a firm, well-circumscribed, slow-growing mass. Because it originates from epidermal cells, the cyst is frequently tethered to the overlying skin, occasionally presenting with a visible central punctum. The mass is typically painless unless it undergoes rapid expansion, ruptures, or becomes secondarily infected. A ruptured EIC releases highly irritating keratinous material into the surrounding soft tissues, inciting a robust, sterile inflammatory response that can clinically mimic a severe soft tissue infection or abscess, presenting with intense erythema, swelling, and localized pain.

When an EIC develops within the distal phalanx—often following a crush injury to the fingertip—it presents as an intraosseous lesion. Radiographically, this appears as a well-defined, radiolucent, expansile lesion within the tuft or diaphysis of the phalanx, without a sclerotic rim. Intraosseous EICs can cause significant cortical thinning, predisposing the patient to pathologic fractures. Surgical management in these cases requires not only meticulous excision of the entire cyst wall to prevent recurrence but also careful curettage of the bone cavity and, occasionally, bone grafting if the structural integrity of the phalanx is critically compromised.
Detailed Surgical Anatomy and Biomechanics
Mastery of hand and wrist soft tissue tumor excision is fundamentally an exercise in applied surgical anatomy. The wrist and hand comprise an intensely crowded landscape of critical neurovascular and tendinous structures, leaving virtually zero margin for error. A millimeter of errant dissection can result in permanent sensory loss, debilitating neuroma formation, or catastrophic vascular compromise. Therefore, the surgeon must approach these procedures with a robust, three-dimensional understanding of the regional anatomy, particularly the fascial planes, ligamentous intervals, and the predictable anomalies of the peripheral nerves.

The biomechanics of the wrist joint also play a crucial role, particularly in the treatment of ganglion cysts. The wrist is a complex intercalated segment, and its stability relies heavily on the intrinsic and extrinsic carpal ligaments. The scapholunate interosseous ligament (SLIL), the most frequent site of origin for dorsal ganglions, is the primary stabilizer of the proximal carpal row. Over-aggressive resection of the dorsal capsule and the dorsal component of the SLIL during ganglion excision can iatrogenically induce scapholunate dissociation, a devastating complication leading to dorsal intercalated segment instability (DISI) and eventual carpal collapse (SLAC wrist).

Similarly, the volar wrist anatomy is a high-stakes environment. The radial artery, the palmar cutaneous branch of the median nerve (PCBMN), and the flexor carpi radialis (FCR) tendon converge in the precise anatomical zone where volar ganglions typically arise. The radial artery, in particular, is often intimately draped over the dome of a volar cyst, its adventitia occasionally blending with the cyst's pseudocapsule. The surgeon must be prepared to perform meticulous sub-adventitial dissection to mobilize the artery safely. Failure to respect these biomechanical and anatomical constraints transforms a straightforward excision into a limb-threatening or function-destroying event.
Dorsal Wrist Anatomy and the Scapholunate Interval
The dorsal approach to the wrist requires navigation through several distinct anatomical layers. Upon incising the skin, the immediate concern is the superficial venous network and the terminal sensory branches of the radial and ulnar nerves. The dorsal sensory branch of the radial nerve (DSBRN) emerges from beneath the brachioradialis tendon approximately 5 to 8 centimeters proximal to the radial styloid. It arborizes extensively over the first, second, and third extensor compartments. These branches are highly variable, exquisitely sensitive to traction injury, and notoriously prone to forming painful neuromas if transected. Meticulous blunt dissection parallel to the nerve fibers is mandatory.

Deep to the subcutaneous tissue lies the extensor retinaculum, which is typically incised over the third extensor compartment, housing the extensor pollicis longus (EPL). The EPL is transposed radially, and the tendons of the fourth compartment (extensor digitorum communis and extensor indicis proprius) are retracted ulnarly to expose the dorsal wrist capsule. The dorsal capsule is a robust, thickened structure composed of the dorsal radiocarpal and dorsal intercarpal ligaments. A precise, often transverse or V-shaped, capsulotomy is required to expose the underlying carpal pathology without compromising the structural integrity of these extrinsic stabilizers.

The epicenter of dorsal ganglion pathology is the scapholunate interval. The SLIL is a C-shaped ligament with distinct dorsal, proximal, and volar components. The dorsal component is the thickest and most biomechanically critical for preventing scapholunate diastasis. Dorsal ganglions invariably arise from a micro-tear or degenerative cleft in this dorsal capsulo-ligamentous complex. The surgical objective is to excise the cyst stalk and a small rim of the surrounding capsule (typically a 1x1 cm window) at its origin on the SLIL, without violating the structural integrity of the ligament itself. Preserving the surrounding capsular tissue is essential to allow for adequate closure or healing without inducing instability.
Volar Wrist Anatomy and the Radioscaphoid Articulation
The volar wrist presents a significantly more hazardous anatomical landscape than the dorsum. Volar ganglion cysts typically present in the interval between the FCR tendon and the radial artery. The initial skin incision must be carefully planned to avoid the palmar cutaneous branch of the median nerve (PCBMN), which typically arises 5 cm proximal to the wrist crease and travels distally between the palmaris longus (PL) and FCR tendons. The PCBMN provides sensation to the base of the palm and is highly susceptible to injury during volar approaches, leading to debilitating dysesthesias.
The radial artery is the most critical structure at risk during volar ganglion excision. The artery runs deep to the brachioradialis in the distal forearm and becomes superficial at the wrist, resting directly on the radius and the volar carpal capsule before diving dorsally through the anatomical snuffbox. Volar ganglions frequently wrap around the radial artery or displace it superficially. The surgeon must routinely identify the artery proximally and distally, utilizing vessel loops for control, and perform meticulous dissection to separate the cyst wall from the arterial adventitia. Inadvertent arterial injury requires immediate microvascular repair.

Deep to the neurovascular structures, the stalk of the volar ganglion most commonly originates from the radioscaphoid or scaphotrapezial (STT) joint capsule. Accessing this deep origin requires retracting the FCR tendon ulnarly and the radial artery radially. The volar extrinsic ligaments, particularly the radioscaphocapitate (RSC) and long radiolunate (LRL) ligaments, are critical stabilizers of the volar carpus. The excision must trace the cyst stalk down to its capsular origin, excising a small window of the capsule while rigorously avoiding transection of the RSC or LRL ligaments, which could lead to a volar intercalated segment instability (VISI) pattern.
Digital Flexor Sheath and Distal Interphalangeal Joint Anatomy
Pathologies within the digits, such as volar retinacular cysts, mucous cysts, and GCTTS, require a deep understanding of the digital microanatomy. The digital neurovascular bundles run volarly and laterally along the digits, intimately associated with the flexor tendon sheath. The bundles are tethered by Cleland's ligaments (dorsal to the bundle) and Grayson's ligaments (volar to the bundle). When excising a GCTTS, these ligaments must often be sequentially divided to mobilize the neurovascular bundle and safely peel the tumor away from the epineurium and adventitia.

Volar retinacular cysts arise directly from the annular pulleys of the flexor tendon sheath, most commonly the A1 or A2 pulleys at the base of the digit. The surgical approach requires a transverse or Brunner incision over the affected pulley. The critical step is protecting the digital nerves, which lie immediately adjacent to the pulley system. The cyst is typically excised along with a small, superficial window of the underlying pulley. Crucially, the surgeon must ensure that the integrity of the A2 or A4 pulleys is not compromised during the excision, as total loss of these structures will result in flexor tendon bowstringing and severe mechanical deficit.

Mucous cysts at the DIP joint present unique challenges related to the nail apparatus. These cysts arise from the dorsal capsule of the DIP joint and frequently extend distally, compressing the germinal matrix of the nail. The germinal matrix is responsible for the production of the nail plate; damage to this structure during cyst excision will result in a permanent, disfiguring longitudinal ridge or split in the nail. The surgical approach must carefully elevate the eponychial fold, trace the cyst stalk to the joint capsule, and crucially, include the excision of any underlying marginal osteophytes, which are the mechanical culprits driving the cyst formation.
Exhaustive Indications and Contraindications
The decision to proceed with surgical excision of a hand or wrist soft tissue tumor must be grounded in a rigorous evaluation of the patient's symptoms, functional deficits, and the natural history of the specific lesion. While many of these tumors are benign and asymptomatic, their presence can cause significant psychological distress, cosmetic concern, and, in advanced cases, severe mechanical or neuropathic compromise. A nuanced understanding of the indications and contraindications is paramount to avoid unnecessary surgery and optimize patient outcomes.

Non-operative management remains the first-line treatment for asymptomatic or mildly symptomatic ganglion cysts. Observation and reassurance are often sufficient, as up to 50% of pediatric ganglions and a significant minority of adult ganglions may resolve spontaneously over time. Closed rupture, historically achieved by striking the cyst with a heavy book (the "Bible bump" treatment), is obsolete and strongly condemned due to the risk of collateral damage. Aspiration, with or without corticosteroid injection, is a common temporizing measure. However, patients must be explicitly counseled that the recurrence rate following aspiration of dorsal ganglions approaches 50% to 60%, and for volar ganglions, it can exceed 80%. Aspiration of volar ganglions is relatively contraindicated due to the proximity of the radial artery.

Surgical intervention is definitively indicated when non-operative measures fail, or when the lesion causes persistent pain, weakness, neurological symptoms, or significant functional impairment. For GCTTS, due to their progressive expansile growth and potential for bone erosion and neurovascular encasement, early surgical excision is almost universally recommended upon diagnosis. Similarly, symptomatic Epidermal Inclusion Cysts, particularly those in the fingertip threatening the bone or nail matrix, warrant prompt surgical removal.
| Pathology | Primary Surgical Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Dorsal Ganglion | Pain limiting function; Failure of aspiration; Cosmetic deformity causing distress; Neuropathic symptoms (rare). | Active local infection; Unmanaged medical comorbidities precluding anesthesia. | Asymptomatic small cysts; Patient unwilling to accept surgical scar/stiffness risk. |
| Volar Ganglion | Pain limiting grip strength; Compression neuropathy (median/ulnar); Rapid enlargement. | Active local infection. | Severe peripheral vascular disease (risk to radial artery); Asymptomatic presentation. |
| Mucous Cyst | Impending skin necrosis/rupture; Nail bed deformity; Painful underlying osteoarthritis. | Active local infection. | Lack of symptoms; Patient unwilling to accept risk of nail deformity. |
| GCTTS | Confirmed or highly suspected diagnosis (due to expansile nature); Neurovascular compression; Bone erosion. | Active local infection. | None strictly, though extensive bone involvement may require staged grafting. |
| Epidermal Inclusion Cyst | Pain; Rapid growth; Impending rupture; Intraosseous involvement threatening structural integrity. | Active local infection (unless incision and drainage is required first). | Small, asymptomatic, deeply seated cysts not causing functional deficit. |
Diagnostic Criteria and Non-Operative Management
Accurate diagnosis relies heavily on a thorough history and physical examination. Transillumination is a simple, highly effective bedside test; ganglion cysts will brilliantly transilluminate, whereas solid tumors like GCTTS or keratin-filled EICs will not. Advanced imaging is not routinely required for classic presentations but is invaluable for atypical masses, recurrent lesions, or when preoperative planning requires precise mapping of neurovascular structures.

Non-operative management, primarily observation or aspiration, requires detailed patient education. If aspiration is attempted, a large-bore needle (18 or 20 gauge) is often necessary to evacuate the viscous mucin. The addition of a corticosteroid injection may theoretically reduce capsular inflammation, though robust, high-level evidence demonstrating a significant reduction in long-term recurrence rates compared to aspiration alone remains equivocal.
Surgical Indications
The primary indication for surgical excision of any soft tissue tumor in the hand is the alleviation of patient symptoms that have proven refractory to conservative measures. Pain is the most common driver, particularly pain that limits activities of daily living or occupational duties. Mechanical symptoms, such as a GCTTS blocking full digital flexion or a volar retinacular cyst causing painful triggering, are absolute indications for surgical decompression.

Impending complications also dictate surgical intervention. A mucous cyst that has thinned the overlying skin to the point of impending rupture must be excised urgently to prevent a catastrophic septic arthritis of the DIP joint. Similarly, an intraosseous EIC that has eroded more than 50% of the cortical diameter of the distal phalanx requires excision and grafting to prevent a pathologic fracture.
Absolute and Relative Contraindications
Absolute contraindications to elective tumor excision are rare but include active, untreated local soft tissue infections (unless the surgery is an incision and drainage of an infected EIC) and severe, unoptimized systemic medical comorbidities that render anesthesia unacceptably dangerous.

Relative contraindications revolve primarily around patient expectations and risk tolerance. A patient with a small, asymptomatic dorsal ganglion who is unwilling to accept the risk of a visible surgical scar, postoperative wrist stiffness, or the 5-10
Clinical & Radiographic Imaging Archive