Miscellaneous and Unusual Hand Infections: A Master Surgical Guide
Key Takeaway
Miscellaneous and unusual hand infections, including herpetic whitlow, clenched-fist human bite injuries, and necrotizing fasciitis, present unique diagnostic and therapeutic challenges. Successful management requires a profound understanding of specific bacteriology, injury biomechanics, and precise surgical indications. This guide details the evidence-based protocols, surgical approaches, and postoperative care necessary to prevent devastating complications such as osteomyelitis, systemic sepsis, or amputation in the compromised upper extremity.
MISCELLANEOUS AND UNUSUAL INFECTIONS OF THE HAND
The human hand is uniquely susceptible to a wide array of infectious pathogens due to its constant interaction with the environment, its complex compartmentalized anatomy, and its vulnerability to trauma. While routine pyogenic infections (such as paronychia and felons) are commonplace, the orthopedic surgeon must be acutely prepared to diagnose and manage miscellaneous and unusual infections. These include viral etiologies, complex polymicrobial inoculations from human bites, opportunistic infections in the immunocompromised host, and rapidly progressive, life-threatening conditions such as necrotizing fasciitis.
A profound understanding of the underlying pathophysiology, specific bacteriology, and precise surgical indications is paramount to preventing catastrophic outcomes, including permanent joint stiffness, digital amputation, and systemic sepsis.
HERPETIC INFECTIONS (HERPETIC WHITLOW)
First described by Adamson in 1909, herpetic infections of the hand—commonly referred to as herpetic whitlow—are viral infections that frequently mimic acute pyogenic bacterial infections. Misdiagnosis is common and can lead to inappropriate and potentially deleterious surgical interventions.
Etiology and Pathophysiology
Herpetic whitlow is caused by the Herpes Simplex Virus (HSV). HSV type 1 and type 2 are the most common culprits in the hand. The virus typically inoculates through a break in the skin, often involving the paronychial region, but it may also present on the volar pad or palm, usually distal to the metacarpophalangeal (MCP) joint. The thumb and index finger are the most frequently affected digits.
Historically, this infection was an occupational hazard for dental hygienists, respiratory therapists, and medical personnel exposed to oral secretions. Today, it is also frequently seen in children secondary to autoinoculation from herpetic gingivostomatitis, and in adults via contact with genital herpes.
Clinical Presentation
The clinical course is distinct but can be easily confused with a bacterial felon or paronychia.
* Prodromal Phase: The infection begins with localized pain, disproportionate to the physical findings, accompanied by erythema and non-pitting edema.
* Vesicular Phase: Over the next several days, clear, fluid-filled vesicles erupt. These vesicles may coalesce to form larger bullae.

FIGURE 78-19: Vesicle eruption typical of herpetic infection. Note the clear, fluid-filled lesions that must not be mistaken for purulent bacterial abscesses.
- Ulcerative Phase: Over approximately two weeks, the vesicles rupture and progress to shallow ulcers.
- Resolution Phase: In the subsequent 7 to 10 days, the lesions begin to dry, crust, and heal. However, viral shedding may continue, rendering the lesions highly infective for an additional 12 days.
Systemic symptoms, including fever, malaise, and regional lymphadenopathy (axillary and epitrochlear adenopathy with forearm lymphangitis), are common and should not automatically prompt a diagnosis of bacterial sepsis.
Diagnostic Evaluation
Diagnosis is primarily clinical, but laboratory confirmation is recommended in atypical cases or immunocompromised hosts.
* Tzanck Smear: Rapid but lacks high sensitivity; reveals multinucleated giant cells.
* Viral Culture & PCR: Polymerase Chain Reaction (PCR) is the gold standard for definitive diagnosis and typing.
* Serology: Herpes antibody titers can confirm primary infection but are less useful for acute management.
Surgical Warning: The "Do Not Cut" Rule
Incision and drainage (I&D) is strictly contraindicated for an uncomplicated herpetic whitlow. Surgical intervention does not decompress the lesion (as there is no true pus), but rather risks systemic viral dissemination, delayed healing, and introduces the high probability of a secondary bacterial superinfection.
Management Protocol
Treatment is primarily medical and supportive.
1. Immobilization and Dressing: The affected digit should be splinted and covered with a dry, sterile dressing to prevent autoinoculation to other body parts or transmission to healthcare workers.
2. Antiviral Therapy: Oral acyclovir, valacyclovir, or famciclovir significantly reduces the duration of symptoms if initiated within the first 48 hours of the prodrome.
3. Surgical Indications: Surgical drainage is only indicated if a concomitant, culture-proven secondary pyogenic infection with true abscess formation occurs. In such rare cases, I&D must be performed meticulously, followed by intravenous antibiotics and continued antiviral therapy.
CLENCHED-FIST INJURIES (HUMAN BITE WOUNDS)
Clenched-fist injuries, colloquially known as "fight bites," account for some of the most severe, destructive, and rapidly progressive infections of the hand. These injuries occur when a clenched fist strikes a human tooth, driving the tooth through the skin, extensor tendon, and joint capsule.
Biomechanics of Inoculation
The devastating nature of this infection is directly tied to the biomechanics of the injury.
When the hand is clenched in a fist, the MCP joint is flexed. The extensor tendon is pulled distally over the joint. The tooth penetrates the skin, slices through the extensor tendon, and breaches the dorsal joint capsule, inoculating the intra-articular space with virulent oral flora.
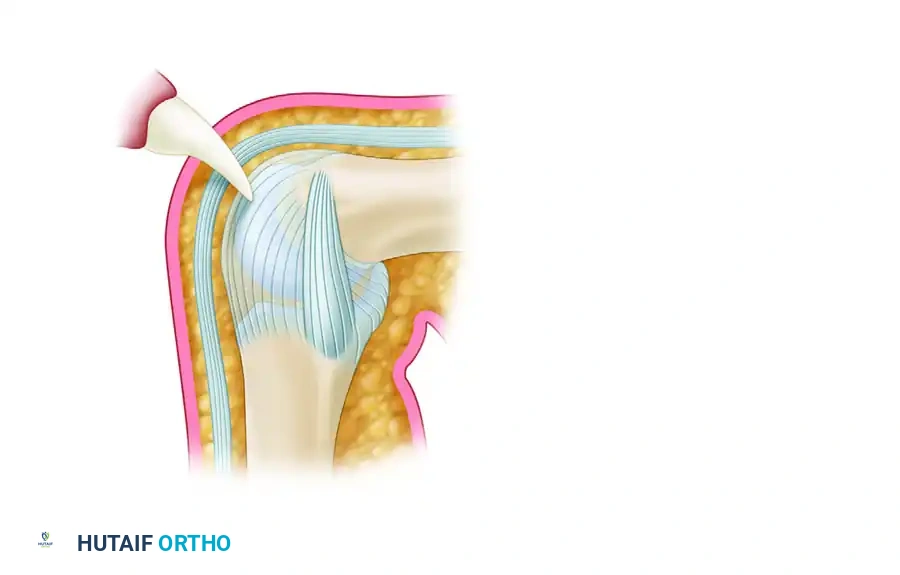
FIGURE 78-18A: Tooth penetrates skin, tendon, and joint capsule while the metacarpophalangeal joint is flexed.
When the altercation ends and the patient extends their fingers, the anatomical layers shift. The lacerated extensor tendon glides proximally, effectively sealing the capsular breach.
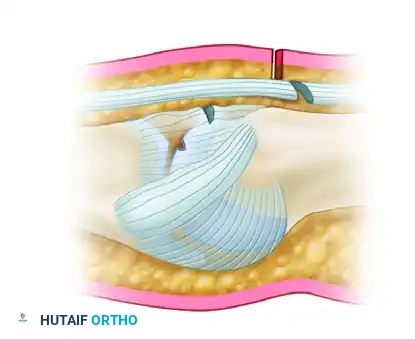
FIGURE 78-18B: When the joint is extended, these tissues shift to occupy different sites; this results in an inoculated, closed, intra-articular wound, providing a perfect anaerobic environment for bacterial proliferation.
Bacteriology
The human mouth harbors over 42 different bacterial species, making these wounds highly polymicrobial.
* Common Aerobes: Staphylococcus aureus and Streptococcus species (particularly α-streptococcus) are the most frequently isolated organisms.
* Pathognomonic Organism: Eikenella corrodens, a fastidious gram-negative facultative anaerobe, is present in up to 30% of human bites. It acts synergistically with other bacteria and is notoriously resistant to first-generation cephalosporins and clindamycin.
* Anaerobes: Bacteroides, Fusobacterium, Peptostreptococcus, and Clostridium thrive in the sealed, hypoxic joint space.
Clinical Evaluation
Patients frequently present with an average delay of 2.5 days, often due to intoxication or embarrassment. The third and fourth digits at the MCP joint are most commonly involved.
* Physical Exam: Look for a small, seemingly innocuous dorsal laceration over the MCP joint. Erythema, fusiform swelling, and severe pain with passive motion indicate established septic arthritis.
* Radiographic Assessment: True AP, lateral, and oblique radiographs are mandatory. Look for metacarpal neck fractures, embedded tooth fragments, and chondral/osteochondral fractures (present in 6% to 59% of cases). Subcutaneous gas may indicate anaerobic infection.
Clinical Pearl: The Index of Suspicion
Any small dorsal laceration over the MCP joint in a young male must be treated as a human bite wound until proven otherwise. Never close these wounds primarily in the emergency department.
Surgical Management Step-by-Step
Aggressive surgical intervention is the cornerstone of treatment. The incidence of complications (osteomyelitis, permanent stiffness, amputation) ranges from 25% to 50%, largely due to delayed or inadequate surgery.
- Positioning and Anesthesia: The patient is placed supine with an arm board. General anesthesia or a regional brachial plexus block is utilized. A sterile proximal tourniquet is applied for hemostasis.
- Incision and Approach: The traumatic laceration is incorporated into a longitudinal or lazy-S dorsal incision. The skin edges are sharply debrided.
- Tendon and Joint Exploration: The extensor tendon is identified. The surgeon must passively flex the MCP joint to recreate the position of injury, bringing the tendon laceration into view and exposing the underlying capsular breach.
- Arthrotomy and Debridement: A formal dorsal arthrotomy is performed. Any foreign bodies (tooth fragments) are removed. Osteochondral fractures are debrided. The joint is aggressively curetted to remove fibrinous exudate and necrotic synovium.
- Lavage: Copious pulsatile lavage (minimum 3 liters of normal saline) is directed into the joint space.
- Wound Management: The wound is strictly left open. Primary closure is contraindicated. The joint capsule and skin are left to heal by secondary intention or delayed primary closure. The hand is dressed with non-adherent gauze and placed in a bulky intrinsic-plus splint (wrist extended 30°, MCPs flexed 70-90°, IP joints fully extended).
Postoperative Protocol
- Antibiotics: Intravenous broad-spectrum antibiotics (e.g., Ampicillin-Sulbactam or Cefoxitin) are initiated immediately after deep cultures are obtained, specifically targeting S. aureus, Streptococcus, E. corrodens, and anaerobes.
- Wound Care: Daily or twice-daily dressing changes.
- Rehabilitation: Early, protected range of motion is initiated once the acute infection is controlled (usually post-operative day 3-5) to prevent extensor tendon adhesions and joint contractures.
INFECTIONS IN PATIENTS WITH ACQUIRED IMMUNODEFICIENCY SYNDROME (AIDS)
Patients with AIDS or AIDS-related complex present a unique challenge to the orthopedic surgeon. The profound depletion of CD4+ T-lymphocytes alters the host's inflammatory response, leading to atypical presentations, rapid progression, and infections by opportunistic organisms.
Clinical Characteristics
- Atypical Pathogens: While S. aureus remains common, surgeons must maintain a high index of suspicion for Mycobacterium avium-intracellulare (MAI), Mycobacterium marinum, Sporothrix schenckii, and Cryptococcus.
- Virulent Herpetic Infections: HSV infections in AIDS patients are exceptionally virulent. They rarely resolve spontaneously, frequently progress to deep tissue necrosis, and require prolonged intravenous antiviral therapy (e.g., IV Acyclovir or Foscarnet for resistant strains).
- Masked Symptoms: Due to immunosuppression, the classic signs of infection (erythema, purulence, leukocytosis) may be blunted. A seemingly benign dorsal bacterial abscess can rapidly silently progress to devastating osteomyelitis or tenosynovitis.
Management Principles
Treatment requires a multidisciplinary approach involving infectious disease specialists. Surgical thresholds should be lowered. Aggressive I&D, extensive debridement of necrotic tissue, and prolonged culture-directed antimicrobial therapy are mandatory. Reconstructive procedures (flaps/grafts) should be delayed until absolute microbiological clearance is confirmed.
NECROTIZING FASCIITIS
Necrotizing fasciitis is a rapidly progressive, life-threatening soft-tissue infection characterized by widespread necrosis of the superficial fascia and subcutaneous tissue, with relative sparing of the underlying muscle. Historically termed "hospital gangrene," the modern nomenclature was established by Wilson in 1952.
Pathophysiology and Classification
The infection spreads rapidly along fascial planes, driven by bacterial exotoxins and enzymes (hyaluronidase, collagenase) that liquefy tissue and cause microvascular thrombosis. This thrombosis leads to ischemia, further necrosis, and systemic toxicity.
Necrotizing infections are classified into two primary microbiological groups:
* Type 1 (Polymicrobial): Accounts for 80% of cases. Caused by a synergistic combination of non-group A streptococci, aerobic gram-negative rods (e.g., E. coli, Klebsiella pneumoniae, Serratia marcescens), and anaerobes (Bacteroides, Clostridium). Often seen in diabetics and the immunocompromised.
* Type 2 (Monomicrobial): Caused by Group A β-hemolytic Streptococcus (GAS), either alone or in combination with Staphylococcus aureus (including MRSA). This type can occur in young, healthy individuals following minor trauma.
Risk Factors
While it can occur in healthy hosts following minor trauma (insect bites, lacerations, steroid injections), susceptibility is vastly increased in patients with:
* Diabetes mellitus
* Peripheral vascular disease
* Immunosuppression (AIDS, chemotherapy)
* Intravenous drug abuse
* Alcoholism and liver cirrhosis
Clinical Presentation
The hallmark of necrotizing fasciitis is pain out of proportion to physical findings.
* Early Stage: The skin may appear normal or exhibit mild erythema, but the patient experiences excruciating pain. Swelling extends far beyond the margins of erythema.
* Intermediate Stage: Development of severe, non-pitting edema. The skin becomes tense, shiny, and loses its capillary refill.
* Late Stage: Microvascular thrombosis leads to skin ischemia, manifesting as violaceous discoloration, hemorrhagic bullae, and eventual frank cutaneous gangrene. Crepitus may be palpable if gas-forming organisms are present.
Notably, lymphangitis and lymphadenopathy are frequently absent because the infectious process destroys the lymphatic vessels. Systemic toxicity (tachycardia, hypotension, altered mental status) ensues rapidly.
Diagnostic Pearl: The LRINEC Score
The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score utilizes CRP, WBC count, Hemoglobin, Sodium, Creatinine, and Glucose to stratify risk. A score ≥ 6 warrants high suspicion. However, a low score does not rule out the disease; clinical judgment remains paramount.
Surgical Management: A True Emergency
Necrotizing fasciitis is an absolute surgical emergency. Survival is directly correlated with the time to initial debridement.
- Radical Debridement: The goal is the complete excision of all necrotic fascia and non-viable tissue until healthy, bleeding tissue is encountered.
- Incision: Extensile longitudinal incisions are made over the involved compartments.
- The "Finger Sweep" Test: Intraoperatively, the diagnosis is confirmed by the lack of resistance to blunt finger dissection along the fascial planes, the presence of "dishwater" (gray, foul-smelling) fluid, and a lack of bleeding from the fascial edges.
- Tissue Sparing: While fascia and subcutaneous fat are aggressively resected, underlying viable muscle and vital neurovascular structures are preserved when possible.
- Second-Look Operations: The wound is packed open. Mandatory "second-look" debridements are scheduled every 24 to 48 hours until the necrosis halts.
Postoperative Care
- ICU Admission: Patients require aggressive hemodynamic resuscitation, vasopressor support, and correction of coagulopathies.
- Antimicrobial Therapy: Empiric broad-spectrum intravenous antibiotics must be initiated immediately (e.g., Meropenem + Vancomycin + Clindamycin). Clindamycin is critical as it halts the ribosomal production of bacterial exotoxins in Group A Strep infections.
- Reconstruction: Once the infection is eradicated and a healthy granulation bed forms, the massive soft-tissue defects are managed with split-thickness skin grafts, local flaps, or free tissue transfer. In cases of irreversible destruction or overwhelming sepsis, life-saving amputation may be required.
📚 Medical References
You Might Also Like
