Operative Management of Dupuytren's Contracture: A Comprehensive Guide
Key Takeaway
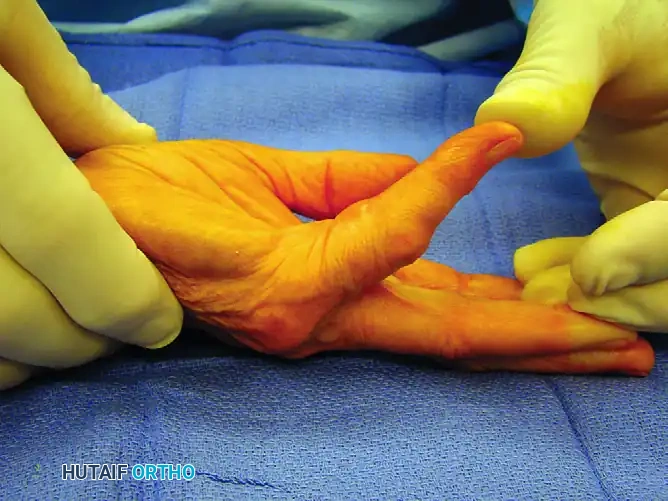
Dupuytren's contracture is a progressive fibroproliferative disorder of the palmar fascia, driven by myofibroblast activity. Surgical intervention, primarily regional fasciectomy, is indicated for metacarpophalangeal contractures exceeding 30 degrees or any proximal interphalangeal joint contracture. This guide details the pathoanatomy, biomechanics, and step-by-step surgical techniques required to safely excise diseased cords, protect displaced neurovascular bundles, and optimize postoperative functional recovery in orthopedic practice.
Introduction to Dupuytren's Disease
Dupuytren’s disease is a progressive, benign fibroproliferative disorder of the palmar fascia that leads to debilitating flexion contractures of the digits. Recognized as an active cellular process driven by the myofibroblast, the condition is characterized by the pathological transformation of normal fascial bands into hypertrophic, unyielding cords.
For the orthopedic surgeon, mastering the management of Dupuytren’s contracture requires a profound understanding of hand pathoanatomy, precise surgical execution, and rigorous postoperative rehabilitation. The disease exhibits a strong genetic predisposition, predominantly affecting individuals of Northern European descent. Furthermore, epidemiological studies have established definitive links between Dupuytren’s diathesis and systemic risk factors, including diabetes mellitus, epilepsy, cigarette smoking, and excessive alcohol consumption.
Clinical Pearl: The presence of ectopic manifestations—such as Garrod’s pads (dorsal knuckle pads), Ledderhose disease (plantar fibromatosis), and Peyronie’s disease (penile fibromatosis)—indicates a strong Dupuytren’s diathesis. These patients are at a significantly higher risk for aggressive disease progression and postoperative recurrence.
Pathogenesis and Cellular Biomechanics
The fundamental pathological unit of Dupuytren’s contracture is the myofibroblast. Ultrastructural and biochemical studies have demonstrated that these specialized contractile fibroblasts possess characteristics of both smooth muscle cells and fibroblasts.
The Role of the Myofibroblast
Myofibroblasts express alpha-smooth muscle actin, which connects to the extracellular matrix via specialized transmembrane linkages (fibronexuses). This allows the cells to exert immense contractile forces on the surrounding collagen network. The disease progresses through three distinct histological stages:
1. Proliferative Stage: Characterized by intense cellularity and the formation of nodules. Myofibroblasts multiply rapidly, and there is a localized increase in Type III collagen.
2. Involutional Stage: The cells align along the lines of tension. The ratio of Type III to Type I collagen remains elevated, and the nodule begins to contract, forming a dense cord.
3. Residual Stage: Cellularity decreases dramatically, leaving behind dense, acellular, and highly cross-linked collagenous cords that mechanically tether the joints in flexion.
Biochemical Alterations
In the diseased palmar fascia, there is a marked alteration in the extracellular matrix. The normal palmar fascia is composed predominantly of Type I collagen. In Dupuytren's disease, there is a significant upregulation of Type III collagen, alongside alterations in prostaglandins and local growth factors (e.g., TGF-beta, FGF, and PDGF) that perpetuate myofibroblast contractility and matrix deposition.
Pathoanatomy: Bands to Cords
Surgical intervention demands an intimate knowledge of how normal anatomical bands transform into pathological cords. The fundamental rule of Dupuytren’s pathoanatomy is that normal fascial bands become diseased cords.
The Pretendinous Cord
Arising from the pretendinous band of the palmar aponeurosis, this cord attaches to the distal palmar crease and the base of the proximal phalanx. Contraction of the pretendinous cord results in isolated metacarpophalangeal (MCP) joint flexion contractures.
The Spiral Cord
The spiral cord is the most critical anatomical structure for the operating surgeon due to its relationship with the neurovascular bundle. It is formed by the confluence of four structures:
1. The pretendinous band
2. The spiral band
3. The lateral digital sheet
4. Grayson’s ligament
Surgical Warning: As the spiral cord contracts, it causes a proximal interphalangeal (PIP) joint contracture and mechanically displaces the neurovascular bundle centrally, proximally, and superficially. The digital nerve is at extreme risk of iatrogenic transection during the initial surgical approach if this displacement is not anticipated.
The Natatory Cord
Originating from the natatory ligaments (superficial transverse metacarpal ligaments), these cords cause web space contractures, preventing digital abduction.
The Central and Lateral Cords
The central cord arises from fibrofatty tissue between the neurovascular bundles and attaches to the middle phalanx, contributing to PIP joint contractures. The lateral cord, derived from the lateral digital sheet, can tether the distal interphalangeal (DIP) joint or contribute to severe PIP flexion.
Clinical Evaluation and Surgical Indications
A thorough clinical examination must document the exact degree of contracture at the MCP, PIP, and DIP joints using a goniometer. The presence of palmar pits, nodules, and skin tethering should be noted.
Hueston’s Tabletop Test
The classic screening tool is Hueston’s tabletop test. The patient is asked to place their hand flat on a hard surface. If the hand cannot be placed completely flat due to fixed flexion, the test is positive, indicating a potential need for intervention.
Indications for Surgery
Surgical intervention is generally indicated when the contracture interferes with activities of daily living. Specific objective criteria include:
* MCP Joint Contracture: Greater than 30 degrees.
* PIP Joint Contracture: Any degree of fixed flexion contracture (typically > 15-20 degrees). PIP joint contractures are notoriously difficult to correct and tend to worsen rapidly; therefore, earlier intervention is recommended.
* Web Space Contracture: Severe adduction contracture limiting hand span.
Preoperative Planning and Patient Positioning
- Anesthesia: Regional anesthesia (axillary or supraclavicular brachial plexus block) is preferred, providing excellent intraoperative conditions and postoperative analgesia.
- Positioning: The patient is positioned supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is essential for a bloodless field. It is typically inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
- Magnification: Surgical loupes (minimum 2.5x to 3.5x magnification) are mandatory for the safe identification and dissection of the neurovascular bundles.
Surgical Approaches
The choice of incision is critical to prevent postoperative scar contracture and to allow adequate exposure of the diseased fascia.
Bruner Zig-Zag Incision
The Bruner volar zig-zag incision is the workhorse approach. The apices of the flaps must end at the mid-axial lines, and the transverse limbs must cross the flexion creases at an angle to prevent linear scar contracture. This approach provides excellent exposure of the neurovascular bundles.
Longitudinal Incision with Z-Plasty
A straight longitudinal incision directly over the palpable cord can be utilized, followed by multiple Z-plasties during closure. This technique effectively lengthens the volar skin, which is often contracted, and breaks up the linear scar.
V-Y Advancement Plasty
For severe proximal palmar disease, a V-Y advancement flap can be utilized to recruit skin and close defects without tension.
Step-by-Step Surgical Technique: Regional Fasciectomy
Regional fasciectomy—the excision of the macroscopically diseased fascia while preserving normal tissue—remains the gold standard of operative treatment.
1. Skin Incision and Flap Elevation
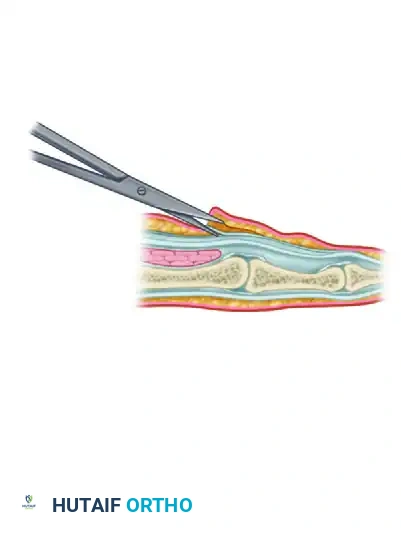
Following the planned Bruner or longitudinal incisions, full-thickness skin flaps are elevated.
* Pitfall: The subdermal plexus must be preserved. Dupuytren’s tissue often invades the dermis, making flap elevation tedious. Dissect sharply with a scalpel (No. 15 blade) or tenotomy scissors, leaving a thin layer of fat on the dermis to prevent full-thickness skin necrosis.
2. Identification of the Neurovascular Bundle
The golden rule of Dupuytren’s surgery is to identify the neurovascular bundle in normal, unscarred tissue before tracing it into the diseased area.
* Begin proximally in the palm where the anatomy is undisturbed.
* Identify the common digital nerve and artery.
* Trace the bundle distally into the digit.
* Use blunt-tipped scissors (e.g., Stevens tenotomy scissors) to gently spread parallel to the nerve.
Surgical Warning: Remember the spiral cord anatomy. At the level of the proximal phalanx, the neurovascular bundle may be displaced superficially and midline, lying directly beneath the skin incision. Extreme caution is required during the initial dermal dissection in this zone.
3. Excision of the Diseased Cords
Once the neurovascular bundles are identified and protected bilaterally, the diseased cords are systematically excised.
* Divide the pretendinous cord proximally in the palm.
* Apply traction to the cord and dissect it distally, peeling it away from the underlying flexor tendon sheath.
* Carefully separate the spiral and central cords from the neurovascular bundles.
* Excise the natatory cords to restore digital abduction.
4. Management of the PIP Joint
If a PIP joint contracture persists after complete fascial excision, the tethering is likely capsuloligamentous.
* Step 1: Perform a flexor tendon sheath release (excision of the C1 or C2 pulleys, preserving A2 and A4).
* Step 2: If contracture persists, perform a release of the accessory collateral ligaments.
* Step 3: If still contracted, a volar plate release (check-rein ligament excision) may be necessary.
* Note: Central slip attenuation can occur in chronic PIP contractures. If the PIP joint is forced into extension, the attenuated central slip may fail, leading to a postoperative boutonnière deformity. Accept a mild residual flexion contracture (10-20 degrees) rather than forcing the joint and risking extensor mechanism failure.
5. Hemostasis and Closure
- Deflate the tourniquet prior to closure.
- Achieve meticulous hemostasis using bipolar electrocautery. Hematoma formation is the most devastating early complication, leading to flap necrosis, infection, and severe stiffness.
- Irrigate the wound copiously.
- Close the skin with non-absorbable monofilament sutures (e.g., 4-0 or 5-0 Nylon). If a longitudinal incision was used, design and transpose the Z-plasties.
- If skin cannot be closed without tension, the "Open Palm Technique" (McCash) can be employed, leaving the transverse palmar wound open to heal by secondary intention.
Alternative Surgical and Minimally Invasive Techniques
Dermofasciectomy
Indicated for recurrent disease or severe primary disease with extensive dermal involvement. The diseased fascia and the overlying involved skin are excised en bloc. The resulting defect is covered with a full-thickness skin graft (typically harvested from the groin or medial arm). The presence of a skin graft acts as a "firebreak," significantly reducing the rate of local recurrence.
Percutaneous Needle Fasciotomy (Aponeurotomy)
A minimally invasive technique where a hypodermic needle is used to percutaneously score and rupture the palpable cords.
* Indications: Elderly patients, multiple comorbidities, or isolated, well-defined pretendinous cords (MCP joint contractures).
* Limitations: High recurrence rate (up to 65% at 3 years) and risk of nerve injury if performed blindly near the PIP joint.
Collagenase Clostridium Histolyticum (CCH) Injection
Enzymatic fasciotomy utilizes purified collagenase to lyse the collagen bonds within the cord. The enzyme is injected directly into the cord, and 24 to 48 hours later, the physician manipulates the finger to rupture the cord. While effective for MCP joints, it carries risks of skin tears, flexor tendon rupture, and immune reactions.
Postoperative Protocol and Rehabilitation
The success of Dupuytren’s surgery is equally dependent on the surgical execution and the postoperative hand therapy.
Immediate Postoperative Phase (Days 0-7)
- A bulky, non-compressive soft dressing is applied in the operating room, incorporating a volar plaster slab.
- The MCP joints are splinted in extension (or slight flexion to relieve tension on the skin flaps), and the PIP joints are splinted in maximum comfortable extension.
- Strict elevation of the hand is mandatory to minimize edema.
Early Rehabilitation (Weeks 1-4)
- The bulky dressing is removed at 3 to 5 days, and a custom thermoplastic volar extension splint is fabricated by a certified hand therapist.
- The splint is worn continuously, removed only for hygiene and active range of motion (ROM) exercises.
- Early active flexion and extension exercises are initiated to prevent tendon adhesions and joint stiffness.
- Sutures are removed at 10 to 14 days once the flaps are stable.
Late Rehabilitation (Weeks 4-12)
- Night splinting in extension is continued for 3 to 6 months to counteract the biological tendency of the healing tissue to contract.
- Scar massage, silicone gel sheeting, and desensitization techniques are employed.
- Strengthening exercises are gradually introduced after 6 weeks.
Complications and Pitfalls
Despite meticulous technique, complications in Dupuytren’s surgery are not uncommon.
- Hematoma: The most frequent early complication. It acts as a nidus for infection and causes pressure necrosis of the overlying skin flaps. Prevention relies on tourniquet deflation and meticulous bipolar hemostasis prior to closure.
- Digital Nerve Injury: The risk is highest at the level of the spiral cord and in revision surgeries. If a nerve is inadvertently transected, it must be repaired immediately using microsurgical epineurial techniques.
- Digital Artery Injury: While the hand has a robust dual blood supply, bilateral digital artery injury can lead to digital ischemia.
- Flare Reaction / Complex Regional Pain Syndrome (CRPS): Characterized by disproportionate pain, swelling, stiffness, and vasomotor changes. Treatment includes aggressive hand therapy, sympathetic blocks, and short courses of oral corticosteroids.
- Recurrence: Dupuytren’s is a systemic diathesis; surgery removes the macroscopic disease but does not cure the underlying cellular pathology. Recurrence rates range from 20% to 50% at 5 years. Patients must be counseled preoperatively that surgery is a management strategy, not a definitive cure.
Conclusion
The operative management of Dupuytren’s contracture is a highly nuanced procedure that demands respect for the intricate anatomy of the hand. By understanding the cellular biomechanics of the myofibroblast, anticipating the pathological displacement of neurovascular structures, and executing a meticulous regional fasciectomy, the orthopedic surgeon can safely restore digital function. Coupled with rigorous postoperative hand therapy, surgical intervention remains the most durable and effective treatment for advanced Dupuytren’s disease.
You Might Also Like