Operative Management of Ankle Ligament and Syndesmotic Injuries
Key Takeaway
The management of ankle ligamentous injuries requires a profound understanding of joint biomechanics and precise diagnostic imaging. While functional rehabilitation remains the gold standard for most lateral sprains, acute surgical intervention is mandated for irreducible deltoid disruptions, frank syndesmotic diastasis, and complex multiligamentous instability. This guide details the evidence-based indications, surgical techniques, and postoperative protocols for optimizing functional outcomes in complex ankle instability.
PRINCIPLES OF ANKLE LIGAMENTOUS INJURIES
The management of ankle ligamentous injuries has evolved significantly, driven by a deeper understanding of ankle kinematics, advanced imaging modalities, and rigorous biomechanical studies. The overarching goal of treatment is the restoration of a congruent ankle mortise and the prevention of chronic instability, which invariably leads to early-onset post-traumatic osteoarthritis.
Biomechanical Pearl: The fundamental principle guiding all ankle trauma surgery was established by Ramsey and Hamilton, who demonstrated that a mere 1-mm lateral shift of the talus within the mortise produces a 42% reduction in the tibiotalar contact area. Because stress per unit area increases exponentially as the total contact area decreases, even microscopic displacement contributes to poor functional outcomes and accelerated articular degradation.
Ankle instability may result from isolated ligamentous disruption, osseous fractures, or a complex combination of both. Clinicians must maintain a high index of suspicion; what may appear as a pure ligamentous injury with talar shift on initial radiographs may actually represent a severe rotational injury, such as a proximal fibular fracture (Maisonneuve variant) with complete syndesmotic disruption.
DIAGNOSTIC IMAGING AND EVALUATION
Advanced Magnetic Resonance Imaging (MRI)
More powerful, high-resolution, three-dimensional MRI studies have revolutionized the diagnostic accuracy of ankle and hindfoot injuries.
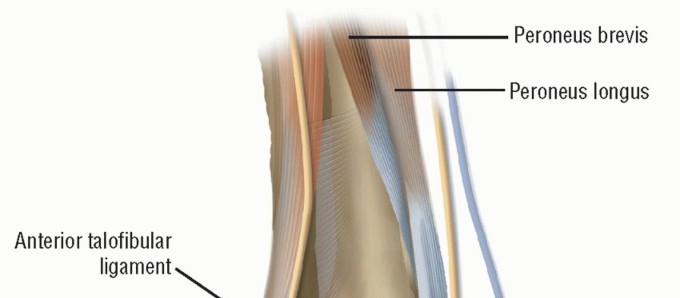
- Axial MRI with a local gradient provides optimal visualization of the anterior and posterior talofibular ligaments, the deep layers of the medial collateral (deltoid) ligament, and the tibionavicular ligament.
- Coronal MRI allows a comprehensive assessment of the calcaneofibular, posterior talofibular, tibiocalcaneal, and posterior tibiotalar ligaments.
In both imaging planes, modern MRI allows for the precise differentiation of the deep and superficial layers of the medial collateral ligament, as well as clear demarcation between the syndesmotic complex and the lateral collateral ligaments.
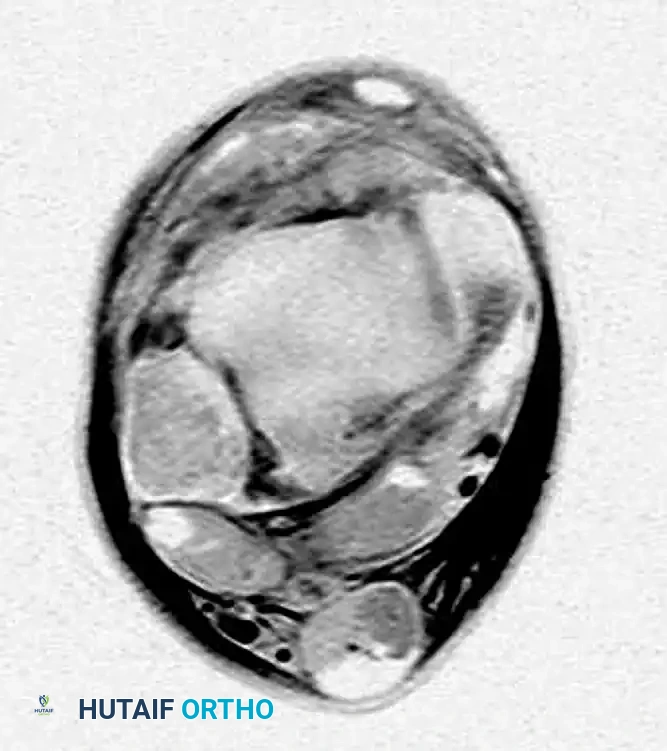
FIGURE 89-6: MRI of a patient with a syndesmosis injury; note the distinct tear of the anterior inferior tibiofibular ligament (AITFL).
Interestingly, Nielson et al. found no direct correlation between tibiofibular clear space and overlap measurements on standard radiographs in patients with MRI-confirmed syndesmotic injuries. However, a medial clear space measurement of more than 4 mm on MRI is highly indicative of deep deltoid ligament incompetence.
Radiographic Relationships
Accurate interpretation of standard radiographs remains the cornerstone of initial evaluation. The relationships evaluating the tibiofibular articulation are critical for diagnosing subtle diastasis.
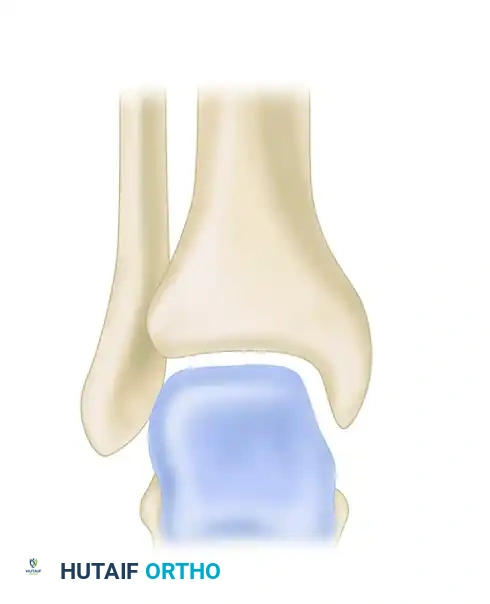
FIGURE 89-7: Radiographic relationships important in evaluating the tibiofibular articulation. Line EF represents the medial clear space; line AB represents the tibiofibular clear space.
MANAGEMENT OF LATERAL AND SUBTALAR LIGAMENT INJURIES
Non-Operative Management: The Role of Functional Rehabilitation
Most Type I and Type II sprains, and indeed the majority of isolated ligamentous injuries, are best treated with functional bracing and early, aggressive rehabilitation. This treatment paradigm allows stretched and attenuated ligaments to heal with reasonable anatomical alignment and length.
For patients with complete tears of the lateral ligaments (Grade III), functional treatment should be initiated immediately. This consists of:
1. A short period of protection with taping or a functional brace.
2. Immediate, protected weight-bearing as tolerated.
3. Early functional range-of-motion exercises.
4. Progressive neuromuscular and proprioceptive training.
Evidence-Based Practice: Kaikkonen et al., in a landmark study of complete Grade III lateral ligament tears, demonstrated that early mobilization yields functional results superior to both surgical repair and rigid cast immobilization. Functional treatment avoids the inherent complications of surgery and prevents the joint stiffness and muscle atrophy associated with prolonged casting.
Even in competitive elite athletes, functional treatment is highly successful, with only 10% to 20% eventually requiring secondary delayed repair or reconstruction. Late mechanical stability is not compromised by an initial trial of conservative care.
Indications for Acute Surgical Repair
While rare, acute surgical intervention for lateral ligament injuries is indicated in specific scenarios:
* Large, displaced bony avulsions.
* Severe, combined ligamentous damage on both the medial and lateral sides of the ankle (indicating a catastrophic joint injury or transient dislocation).
* Severe recurrent injuries failing prolonged conservative management.
Subtalar Instability
In the presence of a clinically severe ankle injury with negative stress radiographs of the tibiotalar joint, the surgeon must suspect an underlying subtalar sprain. Most subtalar ligamentous injuries occur concomitantly with lateral ankle ligament injuries.
Sectioning of the interosseous talocalcaneal ligament, combined with the anterior talofibular ligament, produces a profound change in subtalar kinematics. To quantify the relative contributions of these joints to inversion laxity, subtalar stress radiographs (inversion stress Broden views) may be utilized, though their diagnostic validity remains debated in the literature.
REPAIR OF ACUTE RUPTURE OF THE DELTOID LIGAMENT
Isolated partial ruptures of the deltoid ligament are common, but isolated complete ruptures are exceedingly rare. Typically, acute ruptures of the deltoid ligament are associated with a fracture of the lateral malleolus or disruption of the distal tibiofibular syndesmosis.

FIGURE 89-8A: Acute tear of the deltoid ligament associated with an oblique fracture of the fibula and lateral shift of the talus in the ankle mortise.

FIGURE 89-8B: Postoperative radiograph demonstrating restoration of the mortise after repair of the deltoid ligament and fibular fixation.
Operative vs. Non-Operative Management
Harper reported on 42 patients treated surgically for ankle fractures with complete disruption of the deltoid ligament, without primary deltoid repair. The functional results were highly satisfactory, provided that the surgical reduction of the lateral malleolus was perfectly anatomical and maintained until bone healing was complete. In these cases, the medial joint space reduced spontaneously, and no late medial instability was noted.
Indications for Medial Exploration:
Surgical exploration of the medial ankle is mandatory when there is evidence of severe, irreducible displacement at the time of injury. During attempted reduction of the laterally displaced talus, soft tissue can become incarcerated in the medial clear space. The most common offending structures are:
1. The posterior tibial tendon.
2. The proximal stump of the avulsed deltoid ligament.
Surgical Pitfall: Do not confuse an irreducible mortise with an isolated rupture of the posterior tibial tendon. If the medial clear space remains widened after anatomical fixation of the fibula, you must open the medial side, extract the enfolded tissue, and repair the deltoid ligament directly.

FIGURE 89-9A: Anteroposterior view showing a small avulsion fragment off the medial malleolus and a lateral shift of the talus.

FIGURE 89-9B: Oblique view demonstrating gross widening of the joint space on the medial side of the ankle.

FIGURE 89-9C: Open reduction and internal fixation of the lateral malleolus.

FIGURE 89-9D: Postoperative radiograph showing reduction of the talus into the ankle mortise. In this instance, the deltoid ligament did not require direct repair once the lateral column was restored.
MANAGEMENT OF SYNDESMOTIC INJURIES (DISTAL TIBIOFIBULAR JOINT)
Syndesmotic sprains account for approximately 1% of all ankle injuries and up to 18% of all ankle sprains. These "high ankle sprains" are particularly prevalent in collision sports and military training, carrying a significantly longer recovery time than standard lateral sprains.
Clinical Diagnosis
Accurate clinical diagnosis relies on specific provocative tests, performed only after ruling out proximal fibular fractures.
The Squeeze Test:
Described by Teitz and Harrington, compression of the calf causes separation of the distal fibula and tibia, eliciting pain at the syndesmosis.
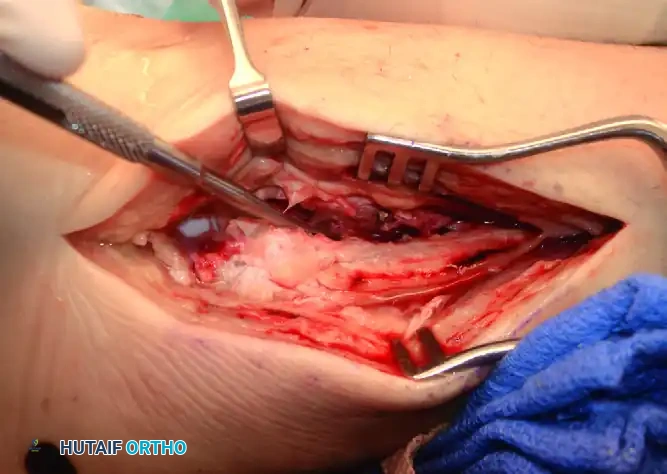
FIGURE 89-11: The Squeeze test is performed by compressing the fibula to the tibia above the midpoint of the calf.

Diagrammatic representation of the Squeeze test mechanism.
The External Rotation Stress Test:
Applying external rotation stress to the involved foot while the knee is flexed to 90 degrees produces pain over the anterior or posterior tibiofibular ligaments.

FIGURE 89-12: External rotation testing.
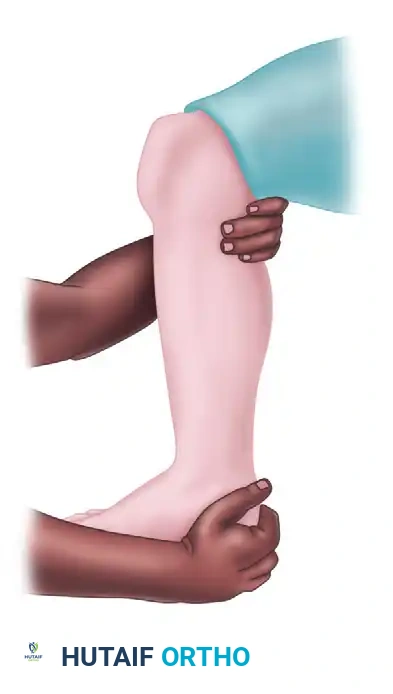
Diagrammatic representation of the External Rotation stress test.
Surgical Indications and Techniques
Diastasis after an isolated syndesmotic injury is rare, and most can be treated non-operatively. However, if widening of the ankle mortise remains after manipulation, or if there is frank instability during intraoperative stress testing (the "Hook Test"), surgical stabilization is absolutely necessary.
Surgical Warning: In surgically treated syndesmosis injuries, malreduction is the single greatest predictor of poor functional outcomes. We strongly advocate for direct open visualization of the syndesmosis (anteriorly) rather than relying solely on closed reduction and percutaneous clamping, which has a high rate of malreduction.

Intraoperative stress view demonstrating syndesmotic widening.

Post-fixation radiograph confirming restoration of the tibiofibular relationship.
Fixation Constructs: Screws vs. Suture Buttons
Screw Fixation:
Historically, metal screws (titanium or stainless steel) have been the gold standard. Biomechanical studies have not shown a significant difference between 3.5-mm and 4.5-mm screws, nor between tricortical and quadricortical fixation in terms of clinical outcomes. However, quadricortical fixation provides improved resistance to shear stress.
* Placement: The screw should be placed 2 to 3 cm proximal and parallel to the distal tibial articular surface.
* Trajectory: Angled 20 to 30 degrees anteromedially, starting on the posterolateral aspect of the fibula to match the anatomical axis of the syndesmosis.
Suture Button Fixation (Dynamic Fixation):
Recently, there has been a paradigm shift toward dynamic fixation using suture button constructs (e.g., Arthrex Tightrope). This device uses two metallic endobuttons secured by a No. 5 braided ultra-high-molecular-weight polyethylene suture.

FIGURE 89-14: Fixation of the syndesmosis utilizing a dynamic suture button construct.

Radiographic appearance of the suture button device maintaining the syndesmotic reduction.
Advantages of Suture Button Fixation:
1. Allows for physiologic micromotion at the syndesmosis, potentially accelerating rehabilitation.
2. Eliminates the need for routine hardware removal (a common requirement for rigid screws before weight-bearing).
3. Reduces the risk of hardware breakage and subsequent osteolysis.
Complications and Sequelae
At long-term follow-up, many patients with severe syndesmotic sprains develop heterotopic ossification or synostosis of the interosseous membrane. While often asymptomatic, in high-demand professional athletes, symptomatic ossification may require delayed surgical excision to allow a return to elite sports. In cases of chronic, painful instability, anatomical reconstruction using autologous grafts (e.g., gracilis tendon) or formal surgical fusion of the syndesmosis may be required.
POSTOPERATIVE PROTOCOL
Following operative stabilization of complex ankle ligamentous and syndesmotic injuries, a strict, phased rehabilitation protocol is essential:
- Phase I (0-2 Weeks): The patient is placed in a well-padded, short-leg splint. Strict non-weight-bearing is enforced to protect the soft tissue envelope and allow initial ligamentous healing. Elevation and cryotherapy are critical.
- Phase II (2-6 Weeks): Transition to a controlled ankle motion (CAM) boot. If rigid screw fixation was used for the syndesmosis, the patient remains non-weight-bearing. If a suture button was utilized, progressive partial weight-bearing may be initiated based on surgeon preference. Active dorsiflexion and plantarflexion are encouraged to prevent stiffness.
- Phase III (6-12 Weeks): Full weight-bearing is achieved. Physical therapy focuses on peroneal strengthening, Achilles stretching, and aggressive proprioceptive training (e.g., balance board). If syndesmotic screws were placed, they are typically removed at 8 to 10 weeks prior to full unprotected weight-bearing to prevent screw breakage.
-
Phase IV (3-6 Months): Return to sport-specific activities. A functional lace-up brace is recommended during high-impact activities for the first year post-injury.
You Might Also Like