Operative Management of Digital Deformities: Flexor Superficialis Transfers and Congenital Anomalies
Key Takeaway
The transfer of the flexor digitorum superficialis (FDS) tendon to the extensor apparatus is a robust surgical technique utilized to correct complex flexion deformities of the proximal interphalangeal joint. This comprehensive guide details the McFarlane technique, alongside the diagnosis and management of congenital digital anomalies including delta phalanx and Kirner deformity, providing orthopedic surgeons with evidence-based operative strategies and postoperative protocols.
TRANSFER OF THE FLEXOR SUPERFICIALIS TENDON TO THE EXTENSOR APPARATUS
The correction of severe, recalcitrant flexion deformities of the proximal interphalangeal (PIP) joint remains a formidable challenge in hand surgery. When conservative measures, such as dynamic splinting and serial casting, fail to yield functional extension, surgical intervention becomes necessary. The transfer of the flexor digitorum superficialis (FDS) tendon to the extensor apparatus, as popularized by McFarlane et al., is a highly effective dynamic tendon transfer designed to augment PIP joint extension while simultaneously removing a deforming volar flexor force.
This procedure is particularly indicated in cases of paralytic deformities, intrinsic minus hands with secondary PIP flexion contractures, and specific traumatic or congenital anomalies where the extensor mechanism is attenuated but the FDS remains functional and expendable.
Preoperative Biomechanical Considerations
Before undertaking an FDS transfer, the surgeon must meticulously evaluate the biomechanical status of the digit. The flexor digitorum profundus (FDP) must be fully intact and functional, as the sacrifice of the FDS will leave the FDP as the sole flexor of the interphalangeal joints. Furthermore, the passive mobility of the PIP joint must be assessed. A dynamic tendon transfer cannot overcome a fixed, rigid joint contracture. If passive extension is severely limited, a concurrent or staged volar plate release and collateral ligament excision (capsulectomy) must be factored into the surgical plan.
Surgical Pearl: The success of the FDS-to-extensor transfer relies heavily on the tenodesis effect. The transferred tendon must be tensioned precisely so that synergistic wrist flexion induces digital extension, while wrist extension allows for digital flexion.
Surgical Technique (McFarlane et al.)
1. Patient Positioning and Anesthesia
The patient is placed supine with the operative arm extended on a radiolucent hand table. The procedure is typically performed under regional anesthesia (brachial plexus block) or general anesthesia, depending on patient compliance and the need for concurrent procedures. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
2. Incision and Exposure
Make a straight midline longitudinal incision over the volar aspect of the affected finger.
Note: While Brunner zig-zag incisions are standard in flexor tendon surgery, a straight midline incision is specifically utilized here so that a multiple Z-plasty closure can be executed at the conclusion of the procedure. This approach allows for the lengthening of the volar skin, which is often contracted in chronic flexion deformities.
Carefully dissect through the subcutaneous tissues, identifying and protecting the neurovascular bundles bilaterally. Expose the flexor tendon sheath from the A1 pulley to the A4 pulley.
3. Tendon Harvest and Routing
Open the flexor tendon sheath, preserving the critical A2 and A4 pulleys to prevent postoperative bowstringing of the remaining FDP tendon.
Identify the flexor digitorum superficialis (FDS) tendon. Isolate the FDS slips at the level of Camper’s chiasm.
Divide the FDS tendon just proximal to the vinculum longum. Preserving the vinculum longum to the FDP is critical to maintaining the vascular supply to the profundus tendon.
Once harvested, withdraw the FDS tendon proximally into the palm or proximal digit. Create a pathway through the lumbrical canal to route the FDS tendon to the dorsal surface of the finger. The lumbrical canal provides a smooth, well-vascularized, and anatomically favorable trajectory that minimizes postoperative adhesions.
4. Tendon Fixation and Tensioning
Expose the dorsal extensor apparatus over the proximal phalanx and PIP joint. The transferred FDS tendon is woven into or sutured directly to the central slip and lateral bands of the extensor apparatus using nonabsorbable, braided sutures (e.g., 3-0 or 4-0 polyester).
Critical Pitfall - Tensioning: Setting the correct tension is the most technically demanding aspect of this procedure. Suture the sublimis tendon to the extensor apparatus and assess the cascade. Tension the transferred tendon so that a normal, physiological stance of the digit is achieved in all wrist positions. Over-tensioning will result in a rigid, extended digit that cannot flex, while under-tensioning will fail to correct the deformity.
5. Management of Residual Deformity
If, after tensioning, the correction of the PIP flexion deformity is incomplete, the surgeon must consider a proximal release of the volar plate (capsulotomy).
Surgical Warning: Aggressive release can lead to PIP joint instability or hyperextension deformities (swan neck). It is generally considered best practice to accept a mild residual flexion deformity of approximately 20 degrees rather than risk destabilizing the joint.
6. Skeletal Stabilization
To protect the tendon transfer and the volar skin closure during the initial healing phase, insert a 0.045-inch or 0.035-inch Kirschner wire (K-wire) retrogradely or anterogradely across the PIP joint to maintain it in maximum safe extension.
7. Closure
Address the volar skin shortage by closing the straight midline incision with single or multiple Z-plasty procedures. This recruits adjacent lateral skin to lengthen the volar contracture line, significantly reducing the risk of recurrent scar-induced flexion contractures. Deflate the tourniquet, achieve meticulous hemostasis, and apply a sterile, non-adherent dressing.
Postoperative Care and Rehabilitation Protocol
The postoperative protocol is designed to protect the transfer while preventing stiffness in adjacent joints.
* Immediate Postoperative Phase: Apply a short-arm cast or rigid orthosis with the metacarpophalangeal (MCP) joints immobilized in 90 degrees of flexion and the interphalangeal digits fully extended. This position relaxes the intrinsic muscles and protects the dorsal transfer.
* Week 4: The cast and the transarticular Kirschner wire are removed in the clinic.
* Weeks 4 to 8: A dorsal blocking splint is applied. This splint must feature a metacarpal stop to prevent overstretching of the newly transferred tendon. Active flexion and extension exercises are initiated within the constraints of the splint.
* Week 8 and Beyond: The splint is gradually weaned, and progressive strengthening is commenced under the guidance of a certified hand therapist.
CONGENITAL DIGITAL ANOMALIES
Understanding congenital anomalies of the phalanges is essential for the pediatric orthopedic surgeon. These deformities often present complex reconstructive challenges due to abnormal physeal growth patterns.
DELTA PHALANX (Longitudinally Bracketed Epiphysis)
The delta phalanx is a complex congenital anomaly characterized by an abnormal, trapezoidal, or triangular-shaped phalanx. The term "delta" is derived from its radiographic resemblance to the Greek letter delta ($\Delta$). Pathoanatomically, this condition is more accurately described as a "longitudinally bracketed epiphysis" (LBE).
Pathoanatomy and Genetics
In a normal phalanx, the epiphysis is located at the proximal base. In a delta phalanx, the abnormal epiphysis is C-shaped or J-shaped and extends longitudinally to bracket the shorter side of the diaphysis. This continuous physeal bracket tethers longitudinal growth on one side while allowing continued growth on the contralateral side, inevitably resulting in a progressive angular deformity (clinodactyly).
The exact incidence of delta phalanx in the general population remains unestablished due to underreporting of mild cases. The specific etiology is unknown; however, in approximately 44% of patients, there is a strong family history demonstrating an autosomal dominant transmission pattern with variable penetrance.
Associated Syndromes
Delta phalanx is rarely an isolated, sporadic anomaly. It serves as a critical clinical marker and usually occurs in association with broader congenital syndromes and hand deficiencies, including:
* Polydactyly and Syndactyly
* Symphalangism
* Cleft foot and Central hand deficiency
* Triphalangeal thumb
* Ulnar clubhand
* Apert syndrome and Poland syndrome
* Diastrophic dwarfism
* Holt-Oram syndrome
Radiographic Evaluation

FIGURE 79-86: Radiographic appearance of delta phalanx. Note the classic triangular shape of the affected phalanx and the continuous bracketed epiphysis tethering the short side of the bone, leading to severe angular deviation.
Radiographs are diagnostic. The affected phalanx appears shortened and wedge-shaped. The continuous epiphyseal bracket is visible along the concave side of the deformity. Early radiographic identification is crucial, as intervention prior to skeletal maturity can alter the growth trajectory.
Management Principles
Treatment is dictated by the severity of the angulation and the age of the patient.
* Early Intervention (Infants/Toddlers): Physioloysis (the Langenskiöld procedure) involves resecting the longitudinal bracket of the physis and interposing fat or synthetic material to prevent physeal bar reformation. This allows the tethered side to resume growth and correct the angulation dynamically.
* Late Intervention (Older Children/Adolescents): Once the deformity is established and growth potential is limited, opening wedge or closing wedge osteotomies of the diaphysis are required to restore mechanical alignment.
KIRNER DEFORMITY (Dystelephalangy)
Originally described by Kirner in 1927, Kirner deformity is a rare, specific congenital anomaly consisting of palmar and radial curving of the distal phalanx, almost exclusively affecting the little finger.
Epidemiology and Etiology
It is an unsightly deformity that occurs infrequently, with an estimated incidence of one per 410 live births. The deformity exhibits a strong sex predilection, occurring significantly more frequently in girls. While it typically affects the little finger bilaterally, it rarely may affect several fingers.
Both sporadic and familial occurrences have been reported, though there is no known specific causative genetic mutation. It is imperative to differentiate true congenital Kirner deformity from acquired conditions that mimic its appearance, such as:
* Frostbite injuries affecting the physis
* Prior physeal fractures (Salter-Harris injuries)
* Osteomyelitis or deep space infections of the distal phalanx
Furthermore, Kirner deformity has been documented in association with several systemic conditions, including Cornelia de Lange syndrome, Silver syndrome, and Turner syndrome.
Clinical Presentation
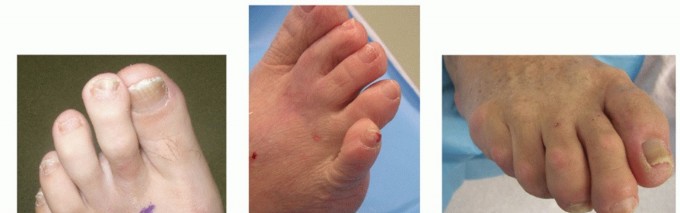
The deformity typically becomes clinically apparent during late childhood or early adolescence, usually when the child is 8 to 10 years old. It presents as a characteristic "beaked" little fingertip accompanied by an increased convexity (clubbing-like appearance) of the fingernail.
The fingertip curves radially and toward the palm. The deformity is usually bilateral and symmetrical. A hallmark of Kirner deformity is that, although it can be progressive during the adolescent growth spurt, it is characteristically not painful.
Radiographic Evaluation
Radiographs are essential to confirm the diagnosis and rule out trauma or infection. Imaging reveals a broadened epiphysis with distinct irregularities of the metaphysis. The typical palmar and radial curvature is localized entirely within the diaphysis of the distal phalanx, distinguishing it from deformities originating at the distal interphalangeal (DIP) joint.
Surgical Management
Clinical Pearl: For mild deformities, conservative management is the rule. Either dynamic splinting or simple observation (no treatment) may be appropriate, as the condition is painless and functional impairment is often minimal.
However, more severe, cosmetically unacceptable, or functionally limiting deformities in skeletally mature patients require surgical correction. The gold standard surgical approach involves one or more osteotomies of the terminal phalanx, as originally described by Carstam and Eiken.
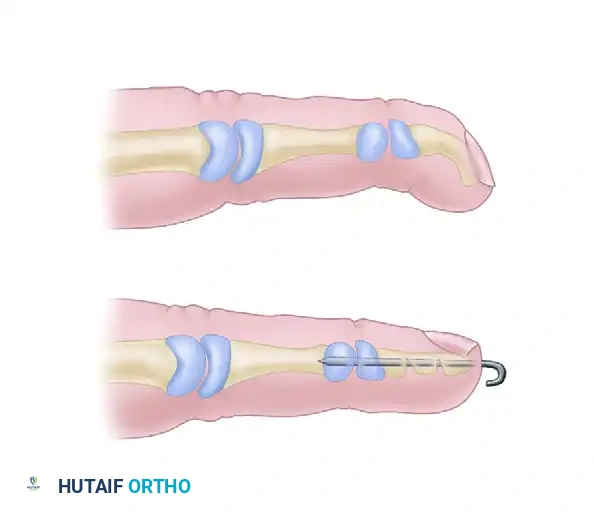
FIGURE 79-85: Carstam and Eiken correction of Kirner deformity. (A) Preoperative clinical and skeletal deformity demonstrating the palmar-radial beak. (B) Multiple opening wedge osteotomy cuts performed in the distal phalanx, corrected, and rigidly fixed with a longitudinal Kirschner wire.
The Carstam and Eiken Technique:
1. A mid-lateral or volar-ulnar incision is made over the distal phalanx to expose the diaphysis while protecting the nail matrix and digital nerves.
2. Multiple transverse, parallel osteotomy cuts (usually two or three) are made across the concave (volar-radial) aspect of the distal phalanx. These are incomplete cuts, leaving the dorsal-ulnar cortex intact to act as a hinge.
3. The osteotomies are gently opened (opening wedge) to correct the palmar and radial curvature, straightening the phalanx.
4. The corrected alignment is stabilized by driving a single longitudinal Kirschner wire antegrade through the tip of the distal phalanx, across the osteotomy sites, and into the base of the distal phalanx or across the DIP joint if additional stability is required.
5. Bone graft is rarely needed due to the robust healing potential of the terminal phalanx.
Note on Nail Deformity: It is vital to counsel patients and parents preoperatively that while the skeletal alignment can be corrected via osteotomy, no effective surgical treatment has been described for the complete correction of the associated convex nail deformity. The nail will likely retain some degree of abnormal curvature despite a perfectly executed osseous correction.
You Might Also Like