Mallet Toe: Comprehensive Surgical Management & Techniques
Key Takeaway
Mallet toe is a rigid or flexible flexion deformity of the distal interphalangeal (DIP) joint, often presenting with a painful terminal corn or dorsal callus. Surgical management is indicated when conservative measures fail. Operative interventions include resection dermodesis, distal interphalangeal joint arthrodesis, and the terminal Syme procedure. This guide details the biomechanics, indications, and step-by-step surgical techniques required to achieve optimal functional outcomes and prevent recurrence in mallet toe correction.
INTRODUCTION TO MALLET TOE DEFORMITY
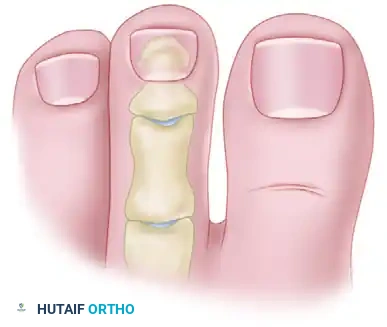
Mallet toe is a common sagittal plane deformity of the lesser digits characterized by an abnormal flexion posture isolated to the distal interphalangeal (DIP) joint. Unlike hammer toe (which involves proximal interphalangeal joint flexion) or claw toe (which involves both PIP and DIP flexion coupled with metatarsophalangeal joint hyperextension), the mallet toe deformity is anatomically restricted to the terminal phalanx.
While it can occur as an isolated clinical entity, it is frequently observed in conjunction with other forefoot pathologies. The primary source of morbidity is mechanical; the flexion deformity drives the tip of the toe into the plantar weight-bearing surface during the propulsive phase of gait, leading to the formation of a painful end corn (heloma durum) or a dorsal callus over the DIP joint due to shoe friction.
This comprehensive guide delineates the pathoanatomy, clinical evaluation, and evidence-based surgical management of mallet toe deformities, tailored for the practicing orthopedic surgeon and foot and ankle specialist.
ETIOLOGY AND BIOMECHANICS
The etiology of mallet toe is multifactorial, encompassing biomechanical imbalances, anatomical predispositions, and extrinsic factors.
Dynamic Muscle Imbalance
The primary biomechanical driver of a mallet toe is an imbalance between the flexor digitorum longus (FDL) and the terminal extensor tendon mechanism.
* Flexor Stabilization: Seen in flexible flatfoot deformities where the FDL fires earlier and longer to stabilize the forefoot, overpowering the interossei.
* Flexor Substitution: Occurs when the triceps surae is weak, and the deep posterior compartment muscles (including the FDL) attempt to substitute for plantarflexion, leading to late-stance phase digital flexion.
* Extensor Substitution: During the swing phase, overactivity of the extensor digitorum longus (EDL) can lead to secondary DIP flexion if the intrinsic muscles fail to stabilize the proximal phalanx.
Extrinsic and Structural Factors
- Footwear: Constrictive, narrow toe-box shoes or high heels force the digits into a flexed posture, leading to adaptive shortening of the plantar capsule and FDL tendon over time.
- Digit Length: A relatively long digit (most commonly the second toe) is mechanically predisposed to buckling within standard footwear, initiating the mallet deformity.
- Trauma: Intra-articular fractures of the DIP joint, crush injuries, or lacerations to the terminal extensor tendon can result in a post-traumatic mallet toe.
- Neurologic Conditions: Charcot-Marie-Tooth disease, diabetic peripheral neuropathy, or lumbar radiculopathy can precipitate intrinsic minus foot mechanics, though these typically present with global clawing rather than isolated mallet toes.
CLINICAL EVALUATION
Patient History
Patients typically present with localized pain at the tip of the involved digit or over the dorsal aspect of the DIP joint. The pain is exacerbated by weight-bearing and tight footwear. A thorough history should rule out systemic inflammatory arthropathies, prior trauma, and neuropathic conditions.
Physical Examination
The hallmark of the physical examination is assessing the flexibility of the deformity.
* Flexible Deformity: The DIP joint can be passively reduced to a neutral alignment.
* Rigid Deformity: The DIP joint is fixed in flexion due to contracture of the plantar capsule, collateral ligaments, and FDL tendon.

Clinical presentation of a rigid mallet deformity of the third toe, demonstrating a prominent dorsal callus over the distal interphalangeal joint.
Plantar view revealing a severe mallet toe with a painful, hyperkeratotic end corn at the terminal pulp.
CLINICAL PEARL: Always evaluate the proximal interphalangeal (PIP) and metatarsophalangeal (MTP) joints. Correcting a mallet toe while ignoring a subtle MTP joint subluxation or PIP contracture will lead to suboptimal outcomes and patient dissatisfaction.
Radiographic Evaluation
Weight-bearing anteroposterior (AP) and lateral radiographs of the foot are mandatory.
* Lateral View: Quantifies the degree of DIP joint flexion and assesses for joint space narrowing, osteophytes, or subluxation.
* AP View: Evaluates the overall digital alignment, relative metatarsal lengths, and the presence of any transverse plane deformities.
SURGICAL INDICATIONS AND DECISION MAKING
Surgical intervention is indicated when conservative measures (e.g., extra-depth shoes, crest pads, silicone toe sleeves, and routine callus debridement) fail to alleviate pain.
The choice of procedure depends heavily on the rigidity of the deformity and the condition of the terminal skin/nail:
1. Flexible Mallet Toe: May be managed with an isolated percutaneous FDL tenotomy.
2. Rigid Mallet Toe: Requires bony resection. Options include DIP joint arthroplasty (resection of the middle phalanx head) or DIP joint arthrodesis. Coughlin and others have reported slightly higher long-term satisfaction rates with successful arthrodesis of the DIP joint, as it prevents recurrence.
3. Severe Mallet Toe with Terminal Ulceration/End Corn: The Terminal Syme procedure or a resection dermodesis is preferred, as these techniques bring the healthy plantar pulp dorsally to close the defect and remove the offending bony prominence.
SURGICAL TECHNIQUE: RESECTION DERMODESIS AND ARTHROPLASTY/ARTHRODESIS
The resection dermodesis combined with hemiphalangectomy (or complete arthrodesis) is the workhorse procedure for a rigid mallet toe. It simultaneously addresses the bony deformity and the redundant, often callused, dorsal skin.
Step 1: Positioning and Anesthesia
The patient is placed in the supine position. The procedure is typically performed under a digital block using a long-acting local anesthetic (e.g., 0.5% bupivacaine) without epinephrine, though a regional ankle block may be utilized. A digital tourniquet (e.g., a sterile Penrose drain or rolled glove finger) is applied to the base of the digit to ensure a bloodless surgical field.
Step 2: Incision and Skin Excision
An elliptical transverse incision is planned over the dorsal aspect of the DIP joint. The ellipse should encompass the dorsal callus. The width of the ellipse dictates the amount of skin tension that will assist in holding the toe in extension (the "dermodesis" effect).

Diagrammatic representation of the planned dorsal elliptical skin incision over the DIP joint.

Intraoperative clinical photograph demonstrating the dorsal incision with the elliptical skin excision completed, removing the hyperkeratotic tissue.
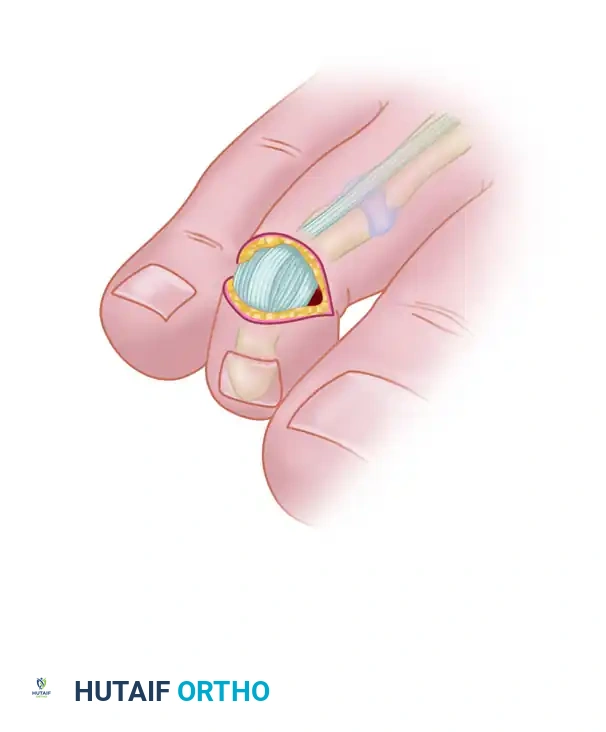
Step 3: Soft Tissue Dissection and Joint Exposure
Following skin removal, the terminal extensor tendon and the dorsal capsule of the DIP joint are identified. These structures are sharply excised in a transverse fashion to expose the underlying articular surfaces.

The extensor tendon and dorsal capsule are sharply excised to gain entry into the distal interphalangeal joint.
Further reflection of the soft tissues exposes the head of the middle phalanx and the base of the distal phalanx.
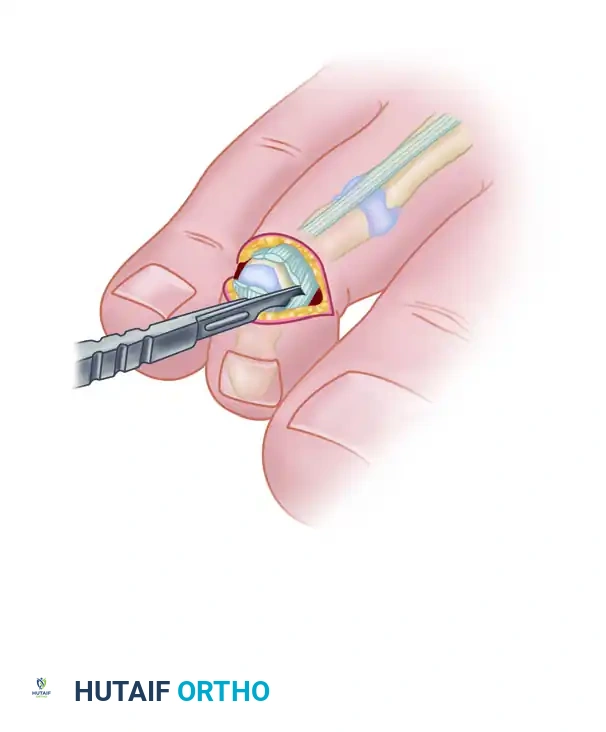
To fully mobilize the joint and allow for adequate bony resection, the medial and lateral collateral ligaments must be completely severed. A #15 blade is passed down the medial and lateral gutters of the middle phalanx head.

The collateral ligaments are severed bilaterally, allowing the distal phalanx to be plantarflexed, fully exposing the condyles of the middle phalanx.
Complete exposure of the middle phalanx condyles, ready for osteotomy.
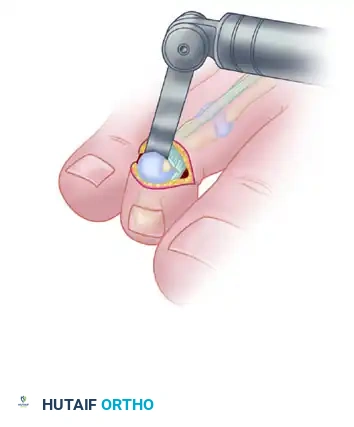
Step 4: Bony Resection (Hemiphalangectomy / Arthrodesis Preparation)
Using a double-action bone rongeur or a microsagittal saw, the head and condyles of the middle phalanx are resected at the surgical neck.
The condyles of the middle phalanx are excised in the supracondylar region using a rongeur or saw.
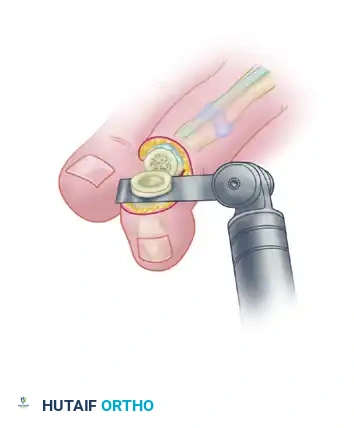
If an arthroplasty is planned, resection of the middle phalanx head alone may suffice. However, if an arthrodesis is desired (which is generally preferred to prevent recurrence), the articular cartilage at the base of the distal phalanx must also be denuded to expose bleeding subchondral bone.
The articular surface of the distal phalanx is excised to prepare the surfaces for a bony fusion.
SURGICAL WARNING: Ensure that the plantar plate and the insertion of the FDL tendon on the distal phalanx are not inadvertently compromised during the bony resection, unless a formal FDL release is pre-operatively planned.
Step 5: Fixation
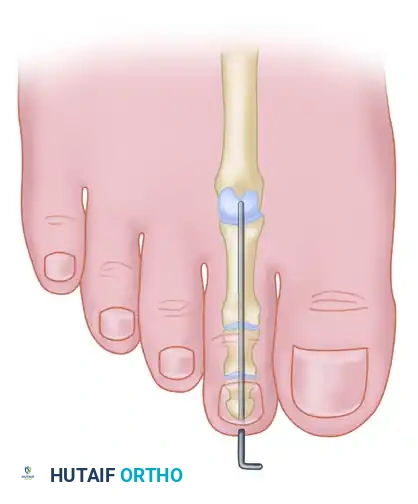
The DIP joint is reduced into a neutral, straight alignment. A 0.045-inch or 0.062-inch Kirschner wire (K-wire) is driven antegrade through the center of the distal phalanx, exiting the tip of the toe just plantar to the nail bed. The wire is then driven retrograde across the prepared DIP joint and into the medullary canal of the middle phalanx.
Placement of the Kirschner wire across the DIP joint to maintain alignment and compress the arthrodesis site.
Step 6: Closure
The tourniquet is released, and hemostasis is achieved. The skin is closed using non-absorbable monofilament sutures (e.g., 4-0 nylon). The elliptical nature of the incision creates a dermodesis effect, mechanically splinting the toe in extension.
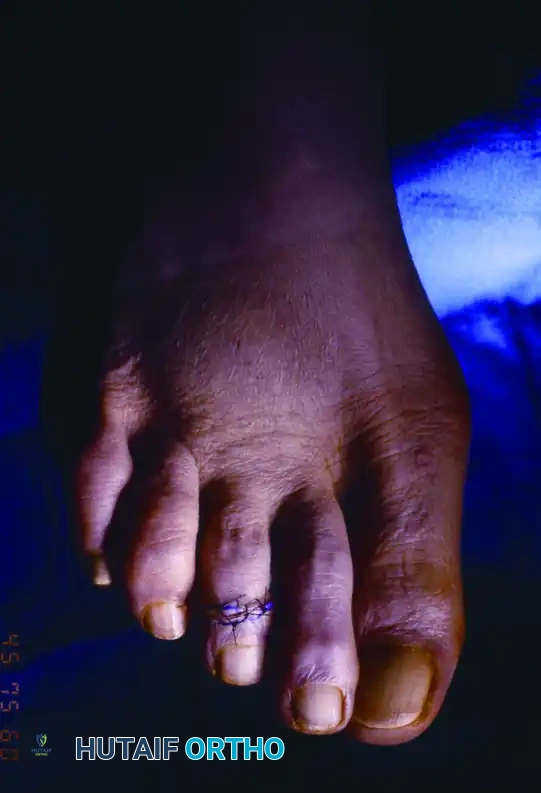
Final clinical appearance after mallet toe correction by dermodesis and hemiphalangectomy. The toe is straight, and the dorsal skin defect is closed under appropriate tension.
SURGICAL TECHNIQUE: TERMINAL SYME PROCEDURE
The Terminal Syme procedure is reserved for severe, rigid mallet toes accompanied by a painful, intractable end corn, terminal ulceration, or significant nail dystrophy. By removing the distal half of the distal phalanx and the entire nail matrix, the symptomatic end-bearing pulp is brought dorsally to close the wound, effectively eliminating the mechanical conflict.
Indications
- Recurrent mallet toe with terminal ulceration.
- Osteomyelitis of the distal phalanx secondary to an infected end corn.
- Severe mallet toe with concomitant onychogryphosis or painful nail deformity.
Step-by-Step Technique
- Incision: An elliptical incision is made encompassing the entire nail plate and the germinal matrix. The incision extends from the distal tip of the toe, curving proximally around the eponychium.
- Nail and Matrix Excision: The nail plate is avulsed. It is absolutely critical to excise the entire germinal and sterile matrix down to the periosteum.
- Bone Resection: The distal half of the distal phalanx (the ungual tuberosity) is resected using a rongeur or bone-cutting forceps.
- Flap Advancement and Closure: The plantar pulp flap, which contains the hyperkeratotic end corn, is mobilized. The corn itself may be sharply excised from the flap. The robust plantar flap is then advanced dorsally over the remaining stump of the distal phalanx and sutured to the proximal dorsal skin margin.

Terminal Syme procedure. A, The planned elliptical incision encompassing the nail. B, Appearance after complete removal of the nail matrix and the distal half of the distal phalanx. Strict attention is paid to ensuring no nail matrix remains. C, Final closure, bringing the plantar pulp dorsally to cover the bony stump.
PITFALL: Failure to completely excise the lateral horns of the germinal matrix is the most common cause of failure in a Terminal Syme procedure. Retained matrix will result in the growth of painful nail spicules through the dorsal flap, necessitating revision surgery.
Notably, a flexor tenotomy is rarely necessary during a Terminal Syme procedure, because the symptomatic end-bearing pulp is physically relocated dorsally, neutralizing the mechanical pressure point regardless of the FDL tension.
POSTOPERATIVE PROTOCOL
Optimal postoperative care is essential to ensure bony union (in arthrodesis) and prevent soft tissue complications.
- Weeks 0-2: The patient is placed in a rigid-soled postoperative shoe and allowed heel-weight-bearing or flat-foot weight-bearing as tolerated. The foot should be elevated strictly to minimize edema. The initial surgical dressing remains intact until the first postoperative visit.
- Weeks 2-4: Sutures are removed at 14 days. If a K-wire is present, pin tract care is initiated (daily cleansing with alcohol or betadine). The patient continues to wear the postoperative shoe.
- Weeks 4-6: The K-wire is typically removed in the clinic between 4 and 6 weeks postoperatively, once clinical stability and radiographic evidence of consolidation (if arthrodesis was performed) are observed.
- Weeks 6+: The patient is transitioned to a wide toe-box athletic shoe. Toe taping or a silicone toe spacer may be used for an additional 2-4 weeks to manage residual edema and maintain alignment.
COMPLICATIONS AND MANAGEMENT
While mallet toe correction is generally highly successful, surgeons must be prepared to manage potential complications:
- Recurrence: More common with isolated arthroplasty or soft-tissue procedures. If symptomatic, revision to a formal DIP joint arthrodesis is indicated.
- Nonunion: Asymptomatic fibrous nonunions of the DIP joint are common and rarely require intervention. Painful nonunions may require revision bone grafting and rigid internal fixation.
- Pin Tract Infection: Superficial erythema around the K-wire is common and usually resolves with oral antibiotics and local pin care. Deep infections may necessitate early pin removal.
- Vascular Compromise: Over-lengthening or excessive straightening of a chronically contracted digit can stretch the digital neurovascular bundles, leading to ischemia. If the toe appears blanched and fails to regain capillary refill after K-wire insertion, the wire must be removed, and the toe allowed to rest in slight flexion. If perfusion does not return, the bony resection must be increased to shorten the digit and relieve vascular tension.
- "Sausage Toe" (Chronic Edema): Prolonged swelling is a known sequela of lesser toe surgery. Patients should be counseled preoperatively that swelling may persist for 3 to 6 months. Compression wrapping and lymphatic massage can aid in resolution.
CONCLUSION
The surgical management of mallet toe deformity requires a nuanced understanding of forefoot biomechanics and meticulous surgical execution. Whether employing a resection dermodesis with arthrodesis for a rigid deformity or a Terminal Syme procedure for a toe with severe terminal ulceration, the primary goals remain consistent: restoration of a plantigrade digit, relief of mechanical pain, and prevention of recurrence. By adhering to the evidence-based techniques and anatomical principles outlined in this guide, orthopedic surgeons can achieve highly reliable and satisfactory outcomes for their patients.
You Might Also Like
