Mallet Toe: Comprehensive Pathophysiology and Surgical Management
Key Takeaway
Mallet toe is a flexion deformity of the distal interphalangeal (DIP) joint, frequently affecting the second digit. Driven by terminal extensor tendon attenuation and unopposed flexor digitorum longus traction, it often results in painful apical corns. Management ranges from conservative shoe modifications to surgical interventions, including percutaneous flexor tenotomy, resection dermodesis, and the terminal Syme procedure, tailored to deformity rigidity and patient comorbidities.
Introduction to Mallet Toe Deformity
Mallet toe is a common forefoot pathology characterized by an isolated flexion posture of the distal interphalangeal (DIP) joint. While it frequently presents as an isolated structural anomaly, it can also occur in conjunction with a hammer toe deformity at the proximal interphalangeal (PIP) joint or as part of a broader cascade of lesser toe deformities involving the metatarsophalangeal (MTP) joint.
Understanding the precise pathoanatomy and biomechanical imbalances driving this deformity is critical for orthopedic surgeons to select the appropriate conservative or operative intervention. This guide provides an exhaustive, evidence-based review of mallet toe etiology, clinical evaluation, and step-by-step surgical management.

Fig. 80-16 Mallet toe demonstrating the classic isolated flexion deformity at the distal interphalangeal joint.
Etiology and Biomechanics
The exact etiology of mallet toe is multifactorial, encompassing structural, biomechanical, and neuropathic elements. It occurs most frequently in the second toe, which is often the longest digit in the human foot (a structural variant sometimes referred to as Morton's toe or Greek foot).
Pathoanatomy of the Deformity
The projection of the second toe distal to the hallux and lesser digits makes it highly susceptible to repetitive microtrauma. When confined within a shoe featuring a narrow or shallow toe box, the distal tip of the toe is subjected to continuous axial loading. This pressure forces the DIP joint into a buckled, flexed position.
Over time, this chronic flexion posture leads to the attenuation and eventual incompetence of the terminal extensor tendon. Once the terminal extensor mechanism fails, it can no longer effectively extend the distal phalanx. In the absence of a strong antagonist, the flexor digitorum longus (FDL) exerts an unopposed plantarflexion force on the distal phalanx. This dynamic imbalance eventually leads to capsular contracture, transforming a flexible deformity into a rigid, fixed mallet toe.
Clinical Pearl: Transfer of the deforming flexor digitorum longus to the extensor mechanism to correct a flexion deformity this far distal is technically difficult and yields unpredictable results. It has little to recommend it over simpler, more dependable procedures such as resection dermodesis or tenotomy.
Neuropathic Considerations
Mallet toe is disproportionately common in diabetic patients suffering from peripheral neuropathy. While the exact mechanism remains a subject of academic debate, it is widely accepted that intrinsic muscle wasting (intrinsic minus foot) combined with extrinsic muscle overpull exacerbates digital deformities. Furthermore, the loss of protective sensation prevents the patient from altering their gait or footwear in response to the repetitive trauma that initiates the deformity.
Clinical Evaluation and Complications
Patients typically present with a primary complaint of pain at the distal tip of the affected toe. Clinical examination must differentiate between a flexible deformity (which is passively correctable) and a rigid deformity (which is fixed due to soft tissue contracture and joint subluxation).

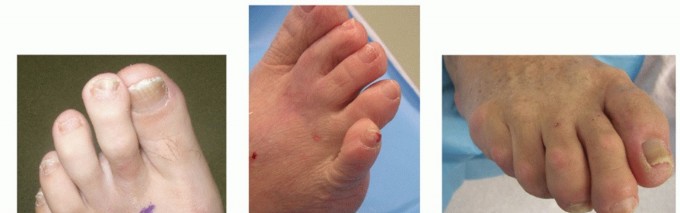
Fig. 80-17A Mallet deformity of the third toe with a prominent dorsal callus, accompanied by a hammer toe deformity of the second digit.
The Apical End Corn
In feet with normal sensibility, the most frequent and bothersome complication of a mallet toe is a painful end corn (heloma durum) located just beneath the nail bed or at the apical pulp. This hyperkeratotic lesion results from chronic, concentrated pressure at the tip of the toe, which is habitually driven into the sole of the shoe during the toe-off phase of the gait cycle.

Fig. 80-18 Mallet toe complicated by a severely painful end corn at the distal pulp.
Surgical Warning: In diabetic patients with peripheral neuropathy, an apical end corn can rapidly ulcerate and progress to deep osteomyelitis before the patient is even aware of the problem. Prophylactic surgical intervention is often warranted in this demographic to prevent catastrophic limb-threatening infections.
It should be noted that congenital mallet toe, much like congenital hammer toe, is usually asymptomatic and rarely requires medical or surgical treatment.
Non-Operative Management
Conservative management of mallet toe is notoriously difficult and generally unrewarding, particularly once the deformity becomes rigid. However, it remains the first-line approach for mild, flexible deformities or for patients with absolute contraindications to surgery.
- Footwear Modifications: The use of extra-depth shoes with a wide, high toe box is paramount to eliminate dorsal and apical pressure.
- Orthotics and Padding: A toe crest pad can be utilized to elevate the distal phalanx and relieve pressure at the tip of the toe. Silicone toe sleeves may also reduce friction over dorsal callosities.
- Limitations: Splinting is generally ineffective for fixed deformities, as the contracted plantar capsule and attenuated extensor mechanism cannot be remodeled through external bracing alone.
Surgical Indications and Decision Making
When conservative measures fail and symptoms warrant surgical intervention, the orthopedic surgeon must select a procedure based on the rigidity of the deformity, the presence of concomitant joint pathology, and the patient's vascular and neurologic status.
The primary surgical alternatives include:
1. Flexor Tenotomy: Indicated for flexible deformities, particularly in elderly or diabetic patients.
2. Resection Dermodesis: The gold standard for rigid mallet toes, involving subtotal or total resection of the middle phalanx head combined with dorsal skin excision.
3. Terminal Syme Procedure: A salvage procedure involving amputation of the distal half of the distal phalanx, indicated for severe fixed deformities with recurrent ulceration or osteomyelitis.
Surgical Technique: Percutaneous Flexor Tenotomy
In elderly patients or those with significant medical comorbidities, a simple flexor tenotomy at the DIP flexion crease may be sufficient to relieve symptoms. We frequently utilize this procedure in diabetic patients due to its simplicity, low risk of ischemic complications, and high efficacy in offloading apical pressure.
Step-by-Step Procedure
- Setting: This procedure can be performed percutaneously in the outpatient clinic setting under local digital block anesthesia.
- Incision: A #11 blade is used to make a stab incision in the midline of the plantar distal interphalangeal crease.
- Tenotomy: The blade is swept medially and laterally to transect the flexor digitorum longus tendon completely. A palpable "pop" and immediate release of the flexion contracture confirm successful tenotomy.
- Manual Correction: The tenotomy is combined with manual, forceful dorsiflexion to rupture any residual fixed capsular contracture at the DIP joint.
- Closure and Dressing: One or two simple sutures are used for hemostasis if needed. A compression forefoot dressing is applied.
- Postoperative Care: The foot is elevated for 5 minutes post-procedure. A wooden-soled postoperative shoe is recommended until the sutures are removed at 2 weeks. Subsequently, the patient is transitioned to adequately long shoes with wide toe boxes.
Surgical Technique: Resection Dermodesis (Technique 80-6)
For mallet deformities of long duration that are fixed in severe flexion, soft tissue release alone is insufficient. Resection of a portion or all of the middle phalanx head, combined with a flexor tenotomy and dorsal dermodesis, is necessary to decompress the joint and maintain correction. This procedure is highly favored as it preserves the nail plate while effectively eliminating the apical end corn.

Fig. 80-17B Dorsal incision demonstrating the elliptical skin excision required for dermodesis.
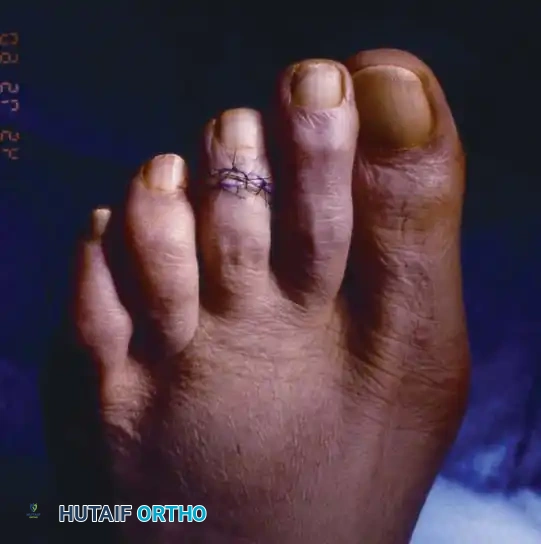
Fig. 80-17C Final correction of the mallet toe achieved via dermodesis and hemiphalangectomy.
Step-by-Step Procedure
- Plantar Tenotomy: Make a 5- to 6-mm transverse incision in the plantar flexion crease of the DIP joint. Meticulously avoid the neurovascular bundles located at the medial and lateral extents of the incision. Using a small, single-pronged hook, isolate the flexor digitorum longus tendon, bring it into the wound, and sharply divide it.
- Note: While the FDL can be exposed dorsally after bone resection, performing the plantar tenotomy first allows the surgeon to better gauge the exact amount of bone resection required to achieve neutral alignment.
- Dorsal Approach: Center a dorsal, transverse, elliptical incision over the DIP joint. Resect the skin within the ellipse (Fig. 80-20A).
- Deep Dissection: Create short (2- to 3-mm) longitudinal extensions of the elliptical incision on each side to facilitate exposure. Divide the collateral ligaments, the terminal extensor tendon, and the dorsal capsule (Fig. 80-20B and C).
- Bone Resection: Acutely flex the distal phalanx to expose the condyles of the middle phalanx. Using a microsagittal saw or a sharp rongeur, remove the head and neck of the middle phalanx at the supracondylar level (Fig. 80-20D).
- Joint Preparation (Optional): If a formal arthrodesis is desired, remove the articular cartilage from the base of the distal phalanx using a small saw or rongeur (Fig. 80-20E).
- Fixation: Reduce the DIP joint to a neutral, straight position. Drive a 0.045-inch Kirschner wire (K-wire) antegrade through the distal phalanx, then retrograde into the middle and proximal phalanges to secure the arthrodesis (Fig. 80-20F).
- Closure: Deflate the tourniquet (if used) and secure hemostasis. Close the dorsal incision with a horizontal mattress stitch in the center to approximate the dermodesis, flanked by simple sutures on each side. Close the plantar wound with simple interrupted sutures.
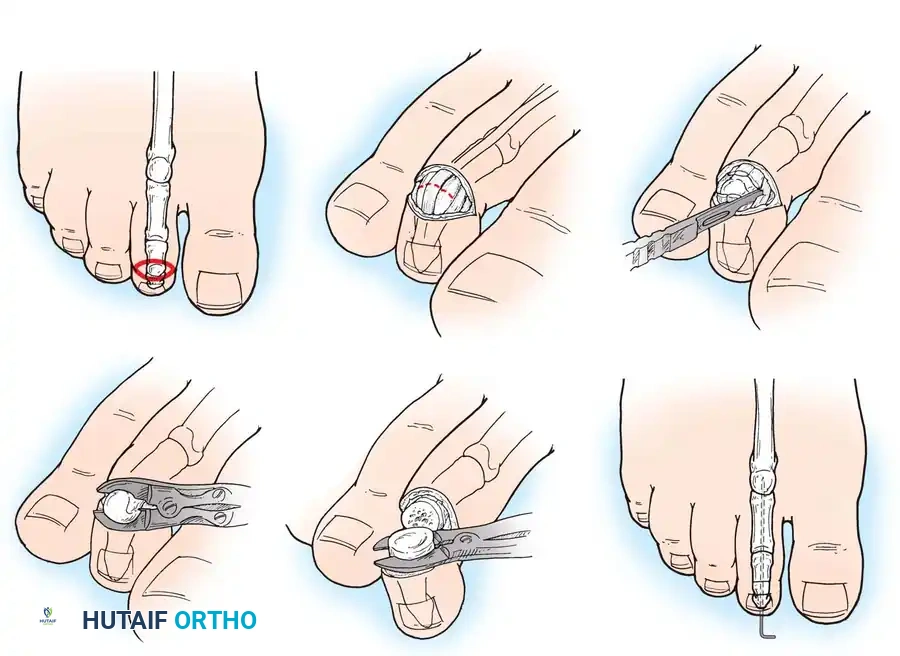
Fig. 80-20 Resection dermodesis technique. A, Elliptical skin incision. B, Excision of extensor tendon and dorsal capsule. C, Severing of collateral ligaments. D, Excision of middle phalanx condyles. E, Excision of distal phalanx articular surface. F, Placement of Kirschner wire for stabilization.
Postoperative Protocol
The toe is splinted to an adjacent digit using a soft dressing. Sutures are removed at 2 weeks. The K-wire is typically maintained for 3 to 4 weeks to allow for fibrous or bony union, after which it is removed in the clinic. The toe is kept buddy-taped for an additional week following pin removal.
Surgical Technique: Terminal Syme Procedure (Technique 80-7)
The terminal Syme procedure is analogous to the technique described for the hallux. It is reserved for severe, fixed flexion contractures at the DIP joint, particularly when complicated by chronic ulceration, osteomyelitis of the distal phalanx, or severe nail dystrophy. By bringing the healthy plantar pulp dorsally, the symptomatic end-bearing tip is eliminated. A flexor tenotomy is generally unnecessary with this approach.

Fig. 80-19 Terminal Syme procedure. A, Incision outlining the nail matrix. B, Following removal of the nail matrix and distal half of the distal phalanx. C, Final closure, bringing the plantar pulp dorsally.
Step-by-Step Procedure
- Incision: Make an elliptical incision that completely encircles the nail of the affected toe. The incision must include 2 to 3 mm of the nail fold on each side and distally, and extend 3 to 4 mm proximally to the eponychium to ensure absolute, complete removal of the germinal nail matrix (Fig. 80-19A). Failure to remove the entire matrix will result in painful nail spicules.
- Dissection: Carry the incision sharply down to the bone proximally. Carefully skirt the side and tip of the phalangeal tuft, freeing the plantar pulp tissue from the distal half of the distal phalanx. Take great care not to disturb or transect the flexor digitorum longus tendon insertion at the base of the distal phalanx.
- Bone Resection: Using a small bone biter or rongeur, resect the exposed distal half of the distal phalanx (Fig. 80-19B). Smooth any sharp bony prominences with a rasp.
- Closure: Bring the robust plantar pulp flap dorsally over the remaining bone and suture it to the proximal dorsal skin edge using non-absorbable sutures (Fig. 80-19C).
Postoperative Protocol
The surgical site is dressed with a non-adherent layer and a compressive wrap. The dressing and sutures are removed at 2 weeks. Because the DIP joint remains stable and the distal lever arm has been shortened, postoperative K-wire splinting is not necessary.
Management of Associated MTP Joint Pathology: Weil Osteotomy (Technique 80-5)
Mallet toe deformities frequently present as part of a complex forefoot collapse, often accompanied by MTP joint subluxation or dislocation (e.g., crossover toe deformity). When the metatarsal is excessively long or the MTP joint is dorsally dislocated, addressing the DIP joint in isolation will lead to suboptimal outcomes. In such cases, a Weil osteotomy of the lesser metatarsal is indicated to decompress the MTP joint, restore the metatarsal parabola, and allow for reduction of the digit.
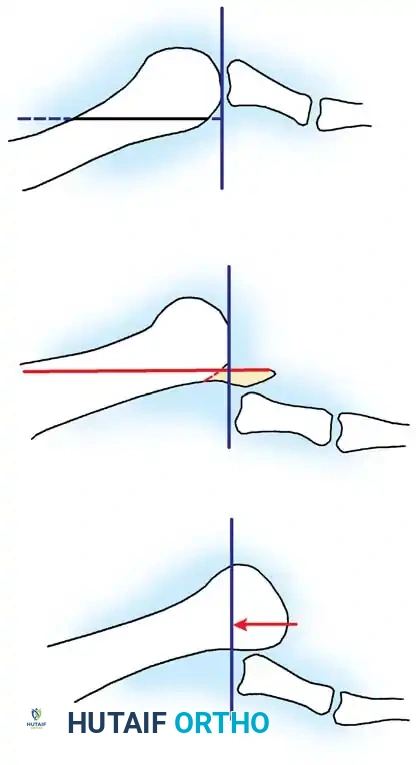
Fig. 80-15 Weil osteotomy. A, Preoperative alignment. B, Following proximal displacement of the plantar metatarsal head fragment. C, After resection of the overhanging distal tip of the dorsal fragment.
Step-by-Step Procedure
- Exposure: Make a 3-cm dorsal longitudinal incision centered over the affected lesser MTP joint. Retract the extensor tendons and incise the dorsal joint capsule.
- Soft Tissue Release: Meticulously dissect the collateral ligaments of the MTP joint off their origins on the metatarsal head.
- Joint Preparation: Partly reduce the dorsal dislocation of the MTP joint and forcefully plantarflex the toe. This maneuver provides optimal, direct exposure of the metatarsal head articular surface.
- Osteotomy: Using a small sagittal saw, create an intra-articular osteotomy. The plane of the cut must be strictly parallel to the weight-bearing surface (the ground), starting from the dorsal portion of the metatarsal head and exiting proximally in the metatarsal metaphysis.
- Displacement: Shift the plantar articular fragment proximally to achieve the requisite amount of shortening. This shortening (typically ranging from 3 to 8 mm) must be measured preoperatively on weight-bearing dorsoplantar radiographs. The goal is to restore a harmonious metatarsal cascade and relieve tension on the plantar plate.
- Fixation: Secure the osteotomy with a single cortical screw from a minifragment AO/ASIF set (typically 2.0 mm or 2.4 mm). Measure the screw length precisely to avoid plantar soft tissue irritation. Ensure the screw head is adequately countersunk into the dorsal cortex. Evaluate the reduction and hardware placement with intraoperative fluoroscopy.
- Remodeling: Remove the resulting dorsal bony protuberance (the overhanging remnant of the proximal fragment) using a rongeur or saw to prevent dorsal impingement and shoe wear irritation.
Clinical Pearl: Studies by Trnka et al. and Vandeputte et al. demonstrate excellent clinical and pedobarographic outcomes with the Weil osteotomy. However, surgeons must be vigilant regarding screw length; penetration of the screw through the plantar cortex is a primary cause of postoperative dissatisfaction and localized plantar pain.
📚 Medical References
- mallet toe deformity with associated double corns, Clin Podiatr Med Surg 13:263, 1996.
- Parrish TF: Dynamic correction of claw toes, Orthop Clin North Am 4:97, 1973.
- Pyper JB: The fl exor-extensor transplant operation for claw toes, J Bone Joint Surg 40B:528, 1958.
- Resnick RB: Jahss MH, Choueka J, et al: Deltoid ligament forces after tibialis posterior tendon rupture: effects of
You Might Also Like