Comprehensive Surgical Management of Hammer Toe and Claw Toe Deformities
Key Takeaway
Hammer toe and claw toe deformities represent complex biomechanical imbalances of the lesser digits. While claw toes typically stem from neuromuscular intrinsic deficits, hammer toes frequently arise from extrinsic factors like constrictive footwear or adjacent ray pathology. Successful surgical management requires a meticulous, stage-based approach—ranging from dynamic flexor-to-extensor transfers for flexible deformities to osseous resections, capsular releases, and Weil osteotomies for rigid, fixed contractures.
Introduction and Pathoanatomy
The terms hammer toe and claw toe describe complex, multi-planar deformities of the lesser digits. While frequently conflated in general practice, they represent distinct pathoanatomical entities with different etiologies, biomechanical drivers, and surgical algorithms.
A hammer toe is primarily characterized by an abnormal flexion posture of the proximal interphalangeal (PIP) joint of one of the lesser four toes. This flexion deformity may present as flexible (passively correctable to a neutral position) or fixed (rigid and not passively correctable). In severe, chronic cases, the metatarsophalangeal (MTP) joint often deforms in the opposite direction, assuming an extension posture. The distal interphalangeal (DIP) joint typically remains supple but may secondarily develop a flexion or extension deformity.

Conversely, a claw toe is defined by a triad of deformities: hyperextension at the MTP joint, flexion at the PIP joint, and flexion at the DIP joint. Claw toes are frequently bilateral, involve all lesser toes simultaneously, and are highly indicative of an underlying neuromuscular disorder.

Differentiating Hammer Toe from Claw Toe
To ensure accurate surgical planning, the orthopedic surgeon must differentiate these deformities based on the following clinical hallmarks:
* Etiology: Claw toes are frequently driven by neuromuscular diseases (e.g., Charcot-Marie-Tooth disease, diabetic neuropathy, spinal dysraphism). Hammer toes are typically idiopathic or related to extrinsic factors.
* Involvement: Claw toes usually affect all lesser toes globally. Hammer toes typically involve only one or two digits (most commonly the second toe).
* MTP Joint Posture: Claw toes always present with an extension deformity at the MTP joint. In hammer toes, MTP extension may or may not be present.
* DIP Joint Posture: Claw toes consistently exhibit a flexion deformity at the DIP joint. Hammer toes generally spare the DIP joint, or it remains supple.


Biomechanics and Etiology
The "Intrinsic Minus" Foot and Claw Toes
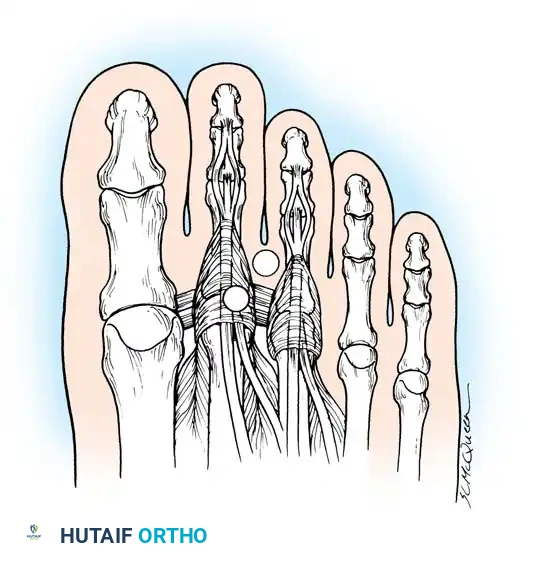
Claw toes are the classic manifestation of an "intrinsic minus" foot. The intrinsic muscles of the foot—specifically the interossei and lumbricals—pass plantar to the axis of rotation of the MTP joint, acting as primary flexors of the MTP joint and extensors of the IP joints.
When a neuromuscular disease causes a loss of intrinsic muscle function, a profound biomechanical imbalance occurs. The extensor digitorum longus (EDL) is left unopposed and hyperextends the MTP joint. Simultaneously, the flexor digitorum longus (FDL) flexes the PIP and DIP joints.
Clinical Pearl: Although the long extensors of the toes can extend the IP joints when the MTP joint is in neutral, they lose their mechanical excursion once the MTP joint hyperextends. Consequently, the EDL can no longer extend the IP joints, allowing the powerful FDL (which inserts at the base of the distal phalanx) to accentuate the clawing deformity.
Idiopathic Hammer Toes
While the etiology of claw toes is rooted in intrinsic denervation, most hammer toes exhibit no underlying intrinsic imbalance. Electromyographic (EMG) studies by Mann and Inman evaluated the phasic activity of the intrinsic muscles during the gait cycle. They found no intrinsic muscle activity during the first 35% of the gait cycle or during quiet standing. Because hammering of the toes is typically accentuated by standing, the absence of intrinsic activity implies that intrinsic weakness is not the primary driver of hammer toe deformities.
Instead, hammer toes are driven by:
1. Extrinsic Compression: Long-term use of poorly fitting shoes with a narrow, restrictive toe box forces the digits into a buckled posture. Over time, this leads to capsular contractures and fixed deformities.
2. Anatomical Predispositions: A "two-bone toe" (synostosis of the PIP or DIP), a long second ray, or severe hallux valgus can cause lateral pressure and buckling of the adjacent second toe.
3. Trauma and Connective Tissue Disorders: Previous fractures, compartment syndrome, or inflammatory arthropathies (e.g., Rheumatoid Arthritis) can disrupt the delicate balance of the extensor hood mechanism.
Clinical Evaluation
Patients with hammer toe deformities typically present with pain localized to three distinct areas of pathological pressure:
- Dorsal PIP Joint: The most common site of pain. A hard corn (heloma durum) develops due to friction against the shoe vamp.
- Distal Phalanx Tip: If a severe flexion or end-bearing posture of the DIP joint is present, a painful "end corn" develops just plantar to the nail bed.
- Plantar Metatarsal Head: If the proximal phalanx subluxates dorsally, the plantar plate is drawn distally, exposing the metatarsal head to increased plantar pressure, leading to an intractable plantar keratosis (IPK).

Neuropathic Considerations
In patients with diminished protective sensation (e.g., diabetes mellitus, myelomeningocele), these areas of focal pressure can rapidly progress to ulceration, deep space infection, and osteomyelitis. Surgical intervention in these patients is often prophylactic to salvage the digit.
Differential Diagnosis of MTP Pain
When evaluating a patient with second toe pathology, the surgeon must differentiate between an interdigital neuroma and idiopathic MTP joint synovitis (predislocation syndrome).
Diagnostic Warning: Tenderness localized to the interspace suggests a neuroma, whereas tenderness directly over the dorsofibular capsule and fibular collateral ligament of the second MTP joint strongly indicates MTP synovitis and impending crossover toe deformity.
Non-Operative Management
Conservative treatment of established hammer toes is frequently disappointing. While commercially available silicone pads, crest pads, and toe strappings can relieve focal pressure, they do not alter the natural history of the deformity.
If the deformity is acute, flexible, and lacks an MTP extension contracture, daily manipulation and taping (plantarflexing the MTP joint to allow the EDL to extend the PIP joint) may provide temporary relief. However, recurrence is nearly universal once taping ceases. Consequently, most symptomatic patients eventually require surgical reconstruction.
Surgical Indications and Decision-Making
Surgical intervention is indicated strictly for symptomatic deformities. Cosmetic dissatisfaction alone is an absolute contraindication to surgery. The surgical algorithm is dictated by the flexibility of the deformity and the joints involved.
1. Mild Deformity (Flexible)
- Characteristics: No fixed contracture at the MTP or PIP joints. Deformity is dynamic and increases upon weight-bearing.
- Treatment: Flexor-to-extensor tendon transfer (FDL transfer).
2. Moderate Deformity (Fixed PIP, Supple MTP)
- Characteristics: Fixed flexion contracture at the PIP joint; no extension contracture at the MTP joint.
- Treatment: Resection arthroplasty of the PIP joint (resection of the head and neck of the proximal phalanx) combined with dermodesis. A percutaneous EDL tenotomy may be added if mild extensor tightness is noted.
3. Severe Deformity (Fixed PIP, Fixed MTP)
- Characteristics: Fixed PIP flexion contracture combined with a fixed MTP extension contracture, with or without dorsal subluxation/dislocation of the proximal phalanx.
- Treatment: PIP resection arthroplasty, EDL lengthening, extensor digitorum brevis (EDB) tenotomy, and dorsal MTP capsulotomy. If the MTP joint remains subluxated, collateral ligament release and a Weil distal metatarsal osteotomy are required.
Operative Techniques
Soft-Tissue Procedures: Flexor-to-Extensor Transfer
Advocated by Girdlestone, Taylor, and later refined by Mann and Coughlin, the flexor-to-extensor transfer is ideal for young patients (<30 years) with dynamic, flexible hammer toes and a normal medial longitudinal arch.
The procedure operates on the principle of converting a deforming force (the FDL) into a corrective force. By transferring the FDL to the dorsal extensor hood, it plantarflexes the MTP joint and extends the PIP joint.

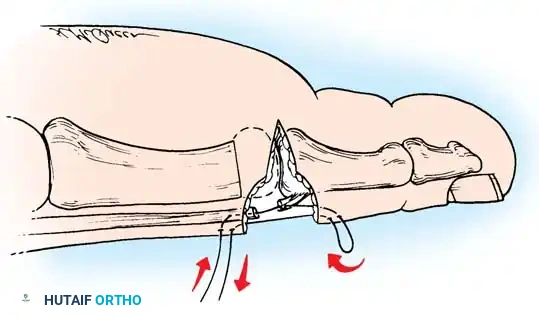
Surgical Pitfall: Myerson and Shereff have questioned the anatomical role of the FDL in causing PIP flexion contractures. Therefore, this soft-tissue procedure must never be used in isolation if any rigid osseous contracture is present at the PIP joint.
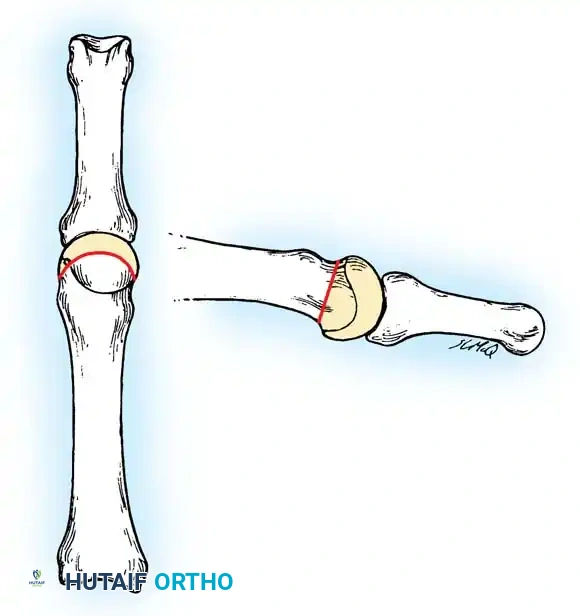
Bone and Joint Procedures: PIP Resection Arthroplasty
For moderate, fixed deformities, resection of the head and neck of the proximal phalanx (DuVries arthroplasty) remains the gold standard. While some authors advocate for formal PIP joint arthrodesis (fusion), clinical studies (e.g., Lehman and Smith) show that up to 52% of patients are dissatisfied with a completely rigid, fused toe. Resection arthroplasty allows for fibrous pseudoarthrosis, providing the toe with limited, comfortable mobility that molds to adjacent digits.
Technique 80-2: Correction of Moderate Deformity
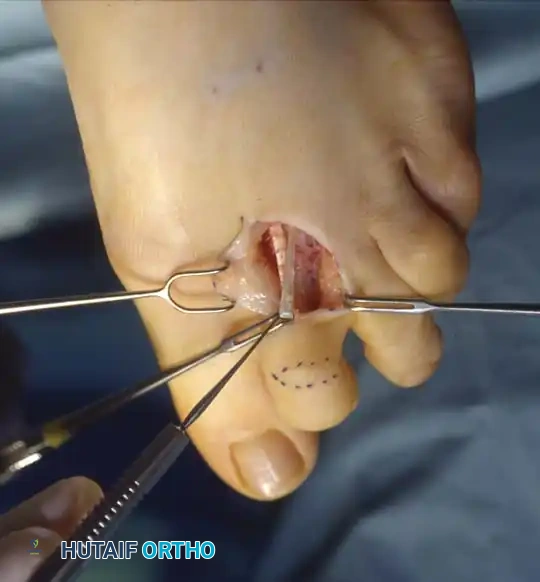
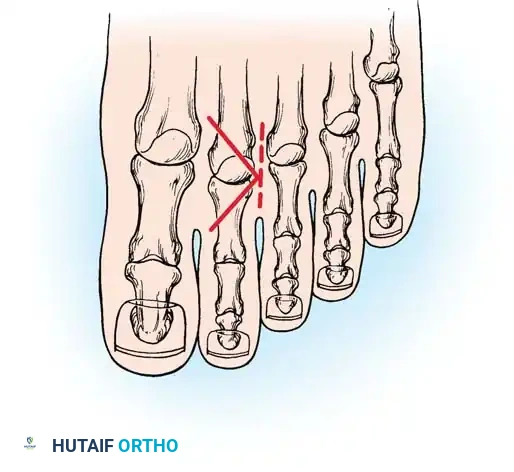
Step 1: Incision and Exposure
Make an elliptical incision over the dorsal aspect of the PIP joint. The ellipse should measure 5 to 6 mm in width, with a 2- or 3-mm lateral extension on either side to facilitate a subsequent dermodesis (skin shortening).
Remove the elliptical skin island carefully, preserving the underlying superficial venous network where possible, and achieve meticulous hemostasis using bipolar electrocautery.

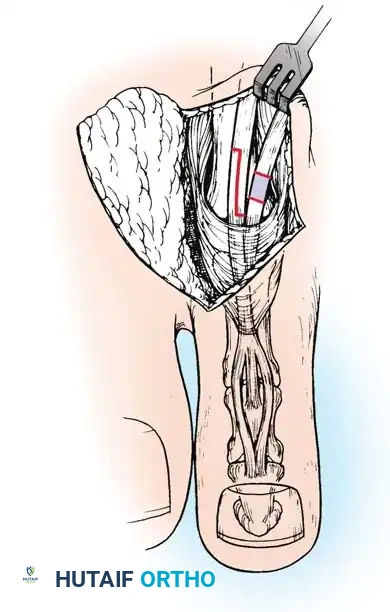
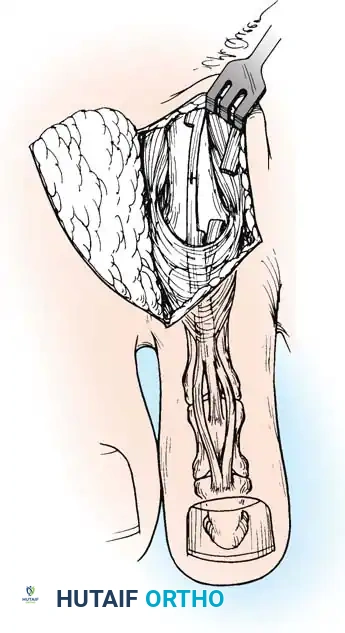
Step 2: Capsulotendinous Resection
Excise a slightly smaller segment of the underlying extensor tendon and dorsal capsule of the PIP joint. It is critical to leave a 2-mm remnant of the extensor tendon attached to the dorsal base of the middle phalanx to facilitate later repair. The proximal stump of the extensor tendon will retract beneath the proximal skin flap but can be easily retrieved.
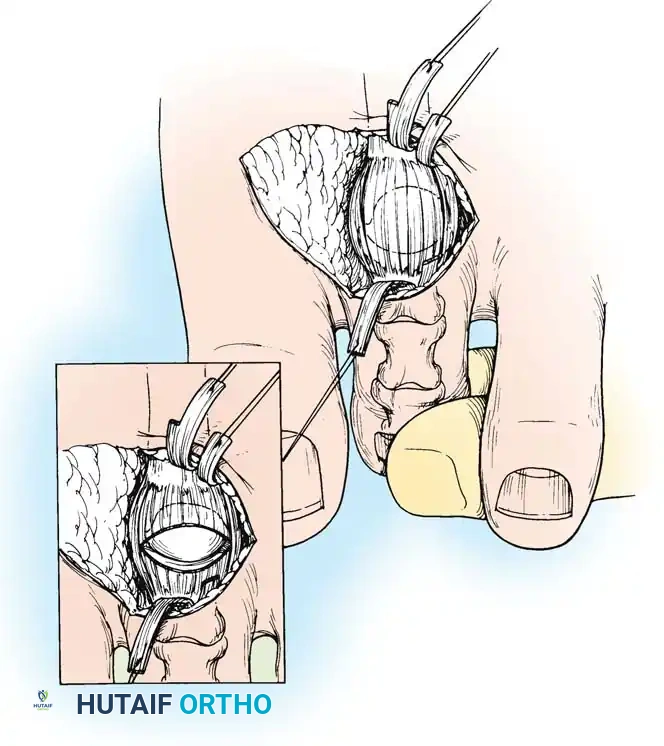
Step 3: Collateral Ligament Release
Apply longitudinal traction to the distal and middle phalanges while flexing the PIP joint to approximately 20 degrees. Using a #15 blade, section the collateral ligaments from outside-in. Place the blade between the skin and the ligament, turning the cutting edge inward toward the joint space to avoid neurovascular injury.

Once the collaterals are released, the PIP joint can be acutely flexed to 90 degrees, fully exposing the condyles of the proximal phalanx.
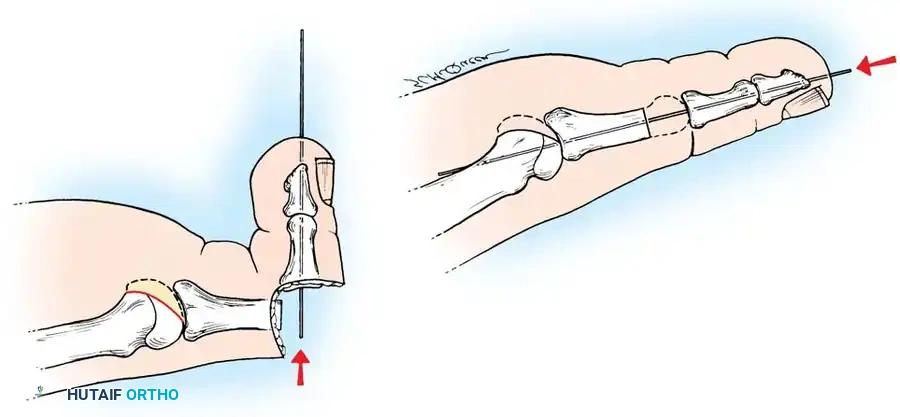
Step 4: Osseous Resection
Using a microsagittal saw or a sharp bone cutter, resect the head and surgical neck of the proximal phalanx.


Ensure the cut is perpendicular to the long axis of the shaft. Use a rongeur or rasp to smooth any sharp cortical edges that could irritate the overlying soft tissues.

Step 5: Closure and Dermodesis
Approximate the extensor tendon ends using a 4-0 absorbable suture. Close the skin with a non-absorbable suture (e.g., 4-0 nylon) using a horizontal mattress technique. Because an ellipse of skin was removed, closing this defect creates a dermodesis—a skin tightening effect that acts as a dynamic splint to hold the toe in extension.
Management of Severe Deformity (MTP Joint Subluxation)
When the hammer toe is accompanied by a fixed MTP extension contracture or dorsal subluxation, PIP resection alone will fail. The MTP joint must be systematically decompressed.
Sequential MTP Release:
1. Extensor Lengthening: Perform a Z-lengthening of the EDL tendon and a tenotomy of the EDB tendon.
2. Dorsal Capsulotomy: Release the dorsal capsule of the MTP joint.
3. Collateral Ligament Release: If the joint remains subluxated, release the medial and lateral collateral ligaments off the metatarsal head. Use a McGlamry elevator to release any plantar plate adhesions.

You Might Also Like
