Extensor Tendon Transfer: Fix Your Flexible Hammer Toe
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Extensor Tendon Transfer: Fix Your Flexible Hammer Toe. A hammer toe deformity is defined by a flexion deformity of the proximal interphalangeal (PIP) joint, often with associated metatarsophalangeal (MTP) joint hyperextension. This results from an imbalance between the foot's static and dynamic stabilizers, including the extrinsic extensor tendons. An **extensor tendon transfer** is a surgical approach that can be considered to rebalance these forces, aiming to correct the deformity and restore proper toe function.
Definition
A hammer toe deformity is defined by a flexion deformity of the proximal interphalangeal (PIP) joint, typically with associated metatarsophalangeal (MTP) joint hyperextension. The distal interphalangeal (DIP) joint may be flexed, extended, or in a neutral position.
Anatomy
The plantar plates of the MTP and PIP joints of the toes provide insertion points for ligaments, tendons, and soft tissue septa.
- At the MTP Joint: The plantar plate originates from the periosteum of the shaft of the metatarsal and inserts onto the base of the proximal phalanx. Plantar plate dysfunction has been associated with hammer toes and claw toes.
- At the PIP Joint: The plantar plate attaches in a similar way, lying immediately plantar to the joint.
- Collateral Ligaments: Insert to the plantar plate at both the PIP and MTP joints.
The final position of the toe depends on the delicate balance between the static stabilizers of the MTP and PIP joints (plantar plate, collateral ligaments) and the dynamic stabilizers (extrinsic and intrinsic tendons).
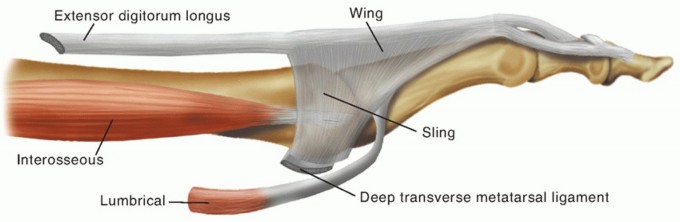
FIG 1: Lateral view of the normal anatomy of the MTP and PIP joints of the lesser toes.
The Dynamic Stabilizers
The extensor digitorum longus (EDL) tendon is the primary extensor of the MTP joint; it attaches to the lateral four toes. The extensor digitorum brevis (EDB) tendon is the only dorsal intrinsic muscle of the foot, and it attaches to the medial four toes. These two tendons maintain their orientation in part due to the fibroaponeurotic extensor hood.
Extension of the PIP and DIP joints is achieved by the coordinated action of the extrinsic extensor tendons and the intrinsic flexor muscles. With paralysis of the intrinsic muscles, the extensor muscles would extend only the MTP joints.
- Extrinsic Flexors: The flexor digitorum brevis (FDB) and flexor digitorum longus (FDL) muscles. The FDB and FDL tendons unite to the base of the middle and distal phalanx, respectively. They flex the PIP and DIP joints and are weak flexors of the MTP joint.
- Intrinsic Flexors: The interossei and lumbrical muscles. The lumbricals flex the MTP joints and extend the interphalangeal (IP) joints; they have a stronger effect over the extension of the PIP and DIP joints due to their distal attachment compared to the interossei, which are weak extensors of the toes.
Pathogenesis
Any disruption of the foot's complex and delicate balance between the static stabilizers (ligaments, plantar plate) and dynamic stabilizers (intrinsic and extrinsic tendons) creates a lesser toe deformity.
With diminished intrinsic muscle flexion power, the extrinsic extensor tendons will extend the MTP joints. With MTP joint extension, the long flexor tendons flex the PIP and DIP joints, resulting in the intrinsic tendons being insufficient in flexing the MTP joint or extending the PIP or DIP joints. This imbalance creates deformity. Plantar plate disruption may also compromise the balance of the toes and promote MTP joint hyperextension.
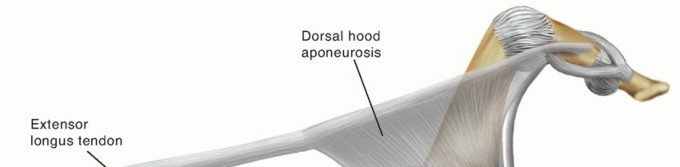
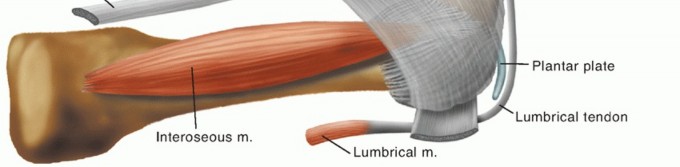
FIG 2: Lateral view of the pathologic anatomy of a hammer toe. Notice how MTP extension renders the lumbricals insufficient and dorsally subluxates the interosseous tendon.
Relative Anatomic Contributions to Deformity
Cadaveric dissections have shown the relative contributions of structures to the deformity, guiding surgical release strategy:
-
For MTP joint hyperextension:
The skin provides ~9% of total deformity, extensor tendons (EDL + EDB) 25%, dorsal capsule 19%, and collateral ligaments 47%.
-
For PIP joint flexion:
The skin accounts for ~20% of deformity, FDB tendon 40%, and plantar capsule 40%; the FDL tendon has no contribution.
With clawing (hyperextension of the MTP joint), the interossei become subluxated in relation to the MTP joint and their line of pull becomes dorsally situated. The lumbricals normally have an angle of 35 degrees with respect to the metatarsal axis; with clawing, they can subtend an angle of 90 degrees, rendering them insufficient to flex the MTP joint.
Etiology
- Posttraumatic: Sequelae of leg injuries, fractures, soft tissue injuries, and compartment syndromes. A scarring or contracture of the deep compartment of the leg can lead to flexion deformities.
- Inflammatory: Rheumatoid arthritis causes capsular inflammation and disruption. Plantar plate attenuation may lead to MTP joint hyperextension.
- Neuromuscular & Congenital: Cerebral palsy, Charcot-Marie-Tooth disease, Friedreich ataxia, spinal dysraphism, idiopathic cavovarus foot, clubfoot sequelae, and arthrogryposis.
- Postsurgical: Dorsiflexion of the metatarsal head after distal metatarsal osteotomies, or secondary to undesired lengthening of tendons.
- Nonspecific: Age-related deficiencies of plantar structures, muscular imbalance, and poor shoe wear (buckling effect in short toe boxes).
Natural History
The natural history is a slow progression to a claw toe, where extension of the MTP joint increases with an increase in PIP flexion.
If the deformity is flexible, the prognosis is good as conservative options may be successful, or simple surgical techniques yield satisfactory outcomes. As the deformity becomes fixed, the chance of successful nonsurgical treatment decreases, and surgery requires more complex reconstructive procedures with an increased risk for postoperative stiffness.
Patient History and Physical Findings
The chief complaint is pain and tenderness on the dorsal PIP joint, typically due to pressure from the shoe. A progressive hammer toe deformity may lead to an extended MTP joint and eventually a plantar callus under the corresponding metatarsal head. Occasionally, with associated PIP and DIP flexion, a plantar callus at the tip of the toe will develop.
Clinical Evaluation:
-
Weight-bearing assessment:
Toe position must be evaluated with weight bearing to appreciate the full extent of the deformity.
-
Push-up test (MTP):
If the deformity is flexible, the MTP joint will flex to normal position. If not, it is a fixed deformity. Semiflexible deformities correct partially.
-
PIP joint stiffness:
Fixed deformities cannot obtain full extension. Flexible deformities allow full passive extension.
-
MTP joint stability staging:
-
Stage 0:
No laxity to dorsal translation.
-
Stage 1:
Base of the proximal phalanx can be subluxated with dorsal stress.
-
Stage 2:
Proximal phalangeal base can be dislocated and relocated.
-
Stage 3:
Base of the proximal phalanx is fixed in a dislocated position.
**Vascular Warning:** A comprehensive neurovascular examination is mandatory. Correction of lesser toe deformities will place digital vessels and nerves on stretch; preoperative neurovascular compromise must be identified before surgery.
Imaging and Other Diagnostic Studies
- Plain Radiographs: Evaluate for periarticular erosions (inflammatory arthritis) and characterize the extent of the deformity (subluxation, dislocation, or deviation). Dislocation of the MTP joint shows an overlap of the base of the proximal phalanx on the metatarsal head on the AP view.
- Magnetic Resonance Imaging (MRI): Reliable for evaluating the extent of plantar plate damage and can guide treatment alternatives for MTP instability, though not routinely needed.

FIG 3: AP view of a foot with hammer toe deformity with MTP joint subluxation. Notice the overlap between the base of the proximal phalanx and the metatarsal head.
Differential Diagnosis
- Fixed hammer toe or claw toe deformities (not amenable to treatment with tendon transfer alone)
- MTP synovitis (absence of deformity warranting tendon transfer)
- Posttraumatic toe deformities
- Soft tissue tumors of the toes
Nonoperative Management
For flexible deformities, an initial conservative approach is recommended:
-
Shoe wear modifications:
Wider, deeper toe box to give more room.
-
Padding:
Metatarsal pads to relieve metatarsal head pressure and toe sleeves to cushion pressure on the PIP joints.
Note: Orthotics must be used judiciously because elevating the toes may lead to greater dorsal PIP joint pressure.
-
Orthoses/Taping:
Hammer toe sling orthoses that hold the proximal phalanx in a more physiologic position.




FIG 4: Hammer toe orthosis designed to hold the proximal phalanx in a plantarflexed position.
Surgical Management
A toe flexor to extensor tendon transfer is rarely performed in isolation; typically, it is an adjunct to a more comprehensive correction. The goal is to reposition the proximal phalanx into a more physiologic alignment ("taping of the toe under the skin").
Despite a flexible deformity, a tendon transfer may need to be performed with dorsal capsulotomy and collateral ligament release of the MTP joint. As the deformity becomes more fixed, a PIP arthroplasty/arthrodesis with or without metatarsal shortening osteotomy is warranted, but the tendon transfer avoids residual elevation ("floating toe").
Preoperative Planning
- MTP Joint Hyperextension: Progressive releases are made (dorsal skin $\rightarrow$ extensor tendons $\rightarrow$ dorsal capsule $\rightarrow$ collateral ligaments) until aligned. For transfer, suture the FDL to the EDL proximal to the middle of the proximal phalanx to obtain more flexion power over the MTP joint. Bone-shortening can be considered if metatarsalgia is present.
- PIP Joint Flexion: FDB releases are considered. If FDB tenotomy is insufficient, add a PIP joint arthroplasty or arthrodesis. Suture the FDL to the EDL distal to the middle of the proximal phalanx to obtain more extension power over the PIP joint. Resection of the proximal aspect of the proximal phalanx should be avoided due to high risk of MTP joint instability.
Positioning & Approach
A supine position is preferred. When performing the flexor to extensor transfer, ensure enough distance between the foot and the distal end of the table so the surgeon can work comfortably from a plantar approach.


FIG 5: Patient positioning ensuring adequate room to comfortably approach the toe distally.
For the MTP approach, a longitudinal or curvilinear dorsal incision is performed. To gain access to the flexor tendons, two plantar incisions are made: one transverse along the proximal skin crease and an oblique/transverse incision over the DIP joint for FDL tenotomy.
Techniques
1. Flexor to Extensor Tendon Transfer
Exposure: Make a plantar incision along the proximal skin crease. Carry the dissection through the subcutaneous layer, identify the flexor tendon sheath, and open it longitudinally.

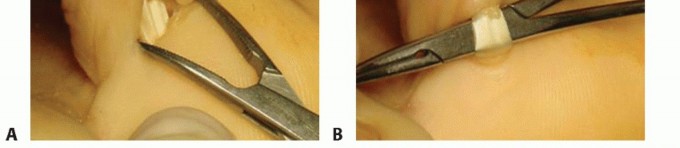
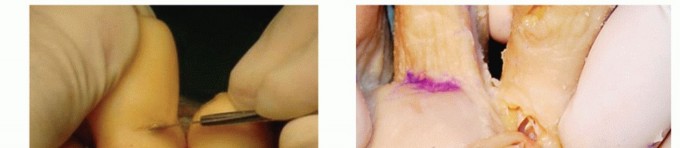
TECH FIG 1: Plantar view of the proximal plantar incision showing flexor tendon sheath identification.
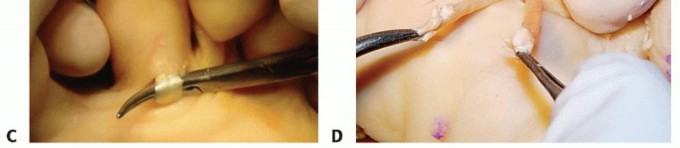
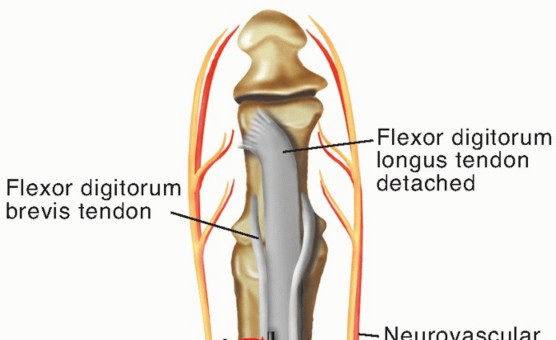
Preparing the FDL: Identify the FDL tendon between the slips of the FDB. Retract it with a hemostat to the surface. Place a second oblique/transverse plantar incision over the DIP. Detach the FDL percutaneously, taking care to direct the scalpel proximally at 45-degrees to avoid the plantar plate. Pull the FDL from the proximal incision, split it into two slips along its midline raphe, and hold each with a hemostat.


TECH FIG 2: Identifying, percutaneously detaching, and splitting the FDL tendon.
Preparing the Extensor Tendon: Place a dorsal longitudinal incision over the dorsum of the proximal phalanx. Identify the extensor tendon and split it in line with the long axis. Carry the dissection in a subperiosteal manner deep to the neurovascular bundle.


TECH FIG 3: Dorsal incision over the proximal phalanx, splitting the extensor tendon along the longitudinal axis.
Performing the Transfer: Pass a small hemostat from the dorsal aspect, between the bone and the periosteum, to the plantar aspect. The tip must pass through the slips of the FDB tendon. Pull half of the FDL tendon dorsal, maintaining relative position (lateral to lateral, medial to medial). With the ankle neutral, MTP joint in 20° plantarflexion, and PIP neutral, secure both slips of the FDL over the extensor tendon with 4-0 absorbable sutures. Deflate tourniquet to ensure revascularization before breaking sterility.
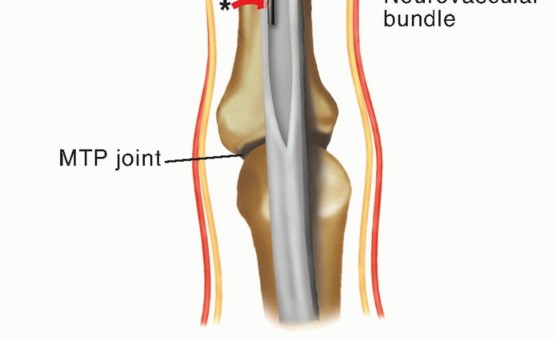
TECH FIG 4: Passing the hemostat deep to the neurovascular bundle to retrieve the FDL tendon halves.
2. Flexor to Extensor Tendon Transfer through a Drill Hole
The technique is similar, but instead of routing around the bone, a 2.0-mm drill hole is placed dorsal to plantar in the junction of the middle and distal third of the proximal phalanx. Pass the tendon through the hole, tension appropriately, and suture it to the extensor sheath.
Pearls and Pitfalls
- Indications: Always correct the deformity going proximal to distal. If there is no metatarsalgia, perform soft tissue procedures before adding a bone shortening (Weil osteotomy) to avoid a floating toe.
- PIP Resection Arthroplasty/Arthrodesis: Common adjuncts. Failure to resect enough of the proximal phalanx head can lead to pain or recurrence.
- Tendon Transfer Execution: Hold the toe down to 20° of plantarflexion at the MTP joint and the ankle at 90° during suturing. If tissues are of poor quality, a Kirschner wire may be used to temporarily fix the joint and protect the repair.
Postoperative Care
- Immediate: Individual soft compressive dressings are placed. Small "tie-down" straps hold each toe in plantarflexion for 6 weeks. Immediate weight bearing as tolerated in a rigid rocker-bottom postoperative shoe.
- Weeks 2 to 4: Once soft tissues allow and stitches are removed, passive plantar flexion exercises of the MTP joint begin to stretch dorsal structures.
- Week 6 onwards: Return to normal shoes is permitted depending on comfort and edema.
Outcomes
Historically, Parrish (1973) described using only the FDL and achieved 83% good to excellent results. Recent series (Boyer and DeOrio) report 89% satisfaction rates in both fixed and flexible hammer toes. Our experience yields good to excellent results in 83% of cases.
Most postoperative complaints are related to stiffness of the PIP joint. Recurrence of deformity (up to 9-20%) is often due to an incomplete preoperative evaluation of MTP joint stiffness, leading to insufficient soft tissue releases.
Complications
- Swelling and Numbness: Usually subside with time. If vascularity is lost intraoperatively due to traction, use warm gauze, remove Kirschner wires if over-distracting, and inject lidocaine around the bundle to assist vasodilation. Nitropaste can also be applied.
- PIP Stiffness: Reported in up to 60% of cases (excluding fusions). It is a main reason for dissatisfaction in flexible corrections.
- Hyperextension Deformities: DIP hyperextension results from excessive volar dissection during FDL harvest. MTP hyperextension results from positioning the transfer too distally or failing to recognize fixed preoperative stiffness.
Scientific References
- 1. Barbari SG, Brevig K. Correction of clawtoes by the Girdlestone-Taylor flexor-extensor transfer procedure. Foot Ankle 1984;5:67-73. [View Source / PubMed]
- 2. Boyer ML, DeOrio JK. Transfer of the flexor digitorum longus for the correction of lesser-toes deformities. Foot Ankle 2007;28:422-430. [View Source / PubMed]
- 3. Coughlin M. Lesser toes abnormalities. J Bone Joint Surg Am 2002;84A: 1446-1469. [View Source / PubMed]
- 4. Cyphers SM, Feiwell E. Review of the Girdlestone-Taylor procedure for clawtoes in myelodysplasia. Foot Ankle 1988;8:229-233. [View Source / PubMed]
- 5. Hurwitz S. Hammertoe deformity following forefoot surgery. Foot Ankle Clin 1998;3:269-277. [View Source / PubMed]
- 6. Kirchner J, Wagner E. Girdlestone-Taylor flexor-extensor tendon transfer. Tech Foot Ankle Surg 2004;3:91-99. [View Source / PubMed]
- 7. Marks R. Anatomy and pathophysiology of lesser toes deformities. Foot Ankle Clin 1998;3:199-213. [View Source / PubMed]
- 8. Myerson M, Shereff M. The pathological anatomy of claw and hammer toes. J Bone Joint Surg Am 1989;71(1):45-49. [View Source / PubMed]
- 9. Nery C, Coughlin M, Baumfeld D, et al. Lesser metatarsophalangeal joint instability: prospective evaluation and repair of plantar plate and capsular insufficiency. Foot Ankle Int 2012;33(4):301-311. [View Source / PubMed]
- 10. Nery C, Coughlin M, Baumfeld D, et al. MRI evaluation of the MTP plantar plates compared with arthroscopic findings: a prospective study. Foot Ankle Int 2013;34(3):315-322. [View Source / PubMed]
- 11. Parrish TF. Dynamic correction of clawtoes. Orthop Clin North Am 1973;4:97-102. [View Source / PubMed]
- 12. Schuh R, Trnka HJ. Metatarsalgia: distal metatarsal osteotomies. Foot Ankle Clin 2011;16:583-595. [View Source / PubMed]
- 13. Thompson FM, Hamilton WG. Problem of the second metatarsophalangeal joint. Orthopedics 1987;10:83-89. [View Source / PubMed]
You Might Also Like


