Operative Management of Fifth Toe Contractures and Angulation Deformities
Key Takeaway
Congenital contracture or angulation of the fifth toe is a common familial deformity that may require surgical intervention to restore foot biomechanics and alleviate shoewear limitations. Operative management ranges from soft-tissue releases, such as the cutaneous Z-plasty, to comprehensive procedures like the Butler arthroplasty. Successful correction relies on meticulous neurovascular preservation, precise capsular release, and strategic soft-tissue transposition to prevent recurrence and vascular compromise.
CONTRACTURE OR ANGULATION OF THE TOES
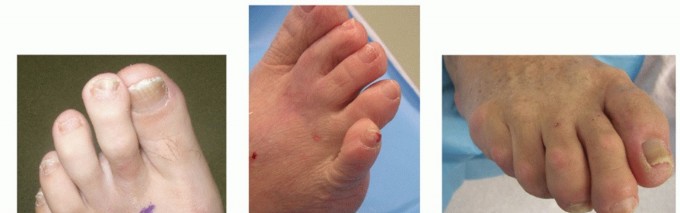
Congenital contracture, angulation, or subluxation of the fifth toe—frequently referred to as an overriding fifth toe or congenital crossover toe—is a fairly common familial deformity. Characterized by dorsiflexion, adduction, and varus rotation of the fifth digit, the condition is often bilateral and presents at birth. While the anomaly is rarely disabling in early childhood, progressive rigidity of the soft tissues and altered foot biomechanics can lead to significant symptoms in adolescence and adulthood.
Conservative management, including taping and splinting, is generally ineffective for rigid deformities. Surgery is usually indicated to improve the function of the foot, alleviate pain associated with shoewear friction (such as dorsal heloma durum formation), and correct the cosmetic appearance. The direction and severity of the angulation of the fifth toe dictate the appropriate operative procedure. Surgical interventions for the correction of an angulated toe encompass a spectrum of techniques, including soft-tissue correction alone, soft-tissue correction combined with proximal phalangectomy, and, in severe or recurrent cases, amputation.
Biomechanics and Pathoanatomy
The deformity is primarily driven by a contracture of the extensor digitorum longus (EDL) tendon, accompanied by secondary contractures of the dorsal and medial metatarsophalangeal (MTP) joint capsule. Over time, the skin overlying the dorsal aspect of the fourth web space becomes contracted, forming a restrictive tether. In long-standing deformities, the plantar capsule becomes adherent, preventing the proximal phalanx from reducing anatomically onto the metatarsal head. Successful surgical correction mandates addressing all three components: the cutaneous tether, the tendinous contracture, and the capsular restrictions.
SURGICAL TECHNIQUE: SOFT-TISSUE RELEASE AND CUTANEOUS Z-PLASTY
Thordarson described a highly effective soft-tissue release combined with a cutaneous Z-plasty for the correction of the congenital overriding fifth toe. In his series, patients reported high satisfaction with the appearance of their foot, with no recurrent deformities, no activity or shoewear limitations, and crucially, no shortening of the toe. This technique is particularly advantageous as it preserves the skeletal integrity of the digit while providing robust soft-tissue lengthening.
Clinical Pearl: The success of the Z-plasty relies on precise geometric design. A 60-degree angle for the Z-plasty limbs theoretically provides a 73% increase in length along the central axis, which is optimal for releasing the dorsal skin contracture without compromising the vascularity of the flaps.
Preoperative Preparation and Positioning
- Anesthesia: Administer a comprehensive ankle block anesthetic to ensure complete regional anesthesia without distorting the local anatomy of the forefoot.
- Hemostasis: Exsanguinate the foot and inflate a sterile ankle tourniquet to provide a bloodless surgical field, which is critical for identifying and protecting the delicate digital neurovascular bundles.
- Positioning: Place the patient supine with a bump under the ipsilateral hip to internally rotate the leg, bringing the lateral aspect of the foot into direct view.
Step-by-Step Surgical Approach
- Incision Design: Approach the fifth MTP joint through a meticulously planned Z-plasty incision. With the toe held manually in the fully corrected (plantarflexed and abducted) position, draw the central limb of the Z-plasty directly along the band of contracted skin extending to the fourth web space.
- Flap Creation: Create the proximal and distal limbs of the Z-plasty so they are of equal lengths to the central limb. Construct the angle of the Z-plasty at exactly 60 degrees. This specific angulation allows maximal elongation along the longitudinal axis of the Z-plasty when the limbs are transposed.
- Tendon Release: Deepen the incision through the subcutaneous tissue, taking care to retract and protect the dorsal cutaneous nerves. Identify the contracted extensor digitorum longus (EDL) tendon of the fifth toe. Release the EDL tendon in a long, oblique fashion (fractional lengthening) to allow for controlled elongation while maintaining continuity.
- Capsulotomy: Expose the MTP joint. Perform a thorough release of the dorsal and medial capsule. Once released, place the toe in the corrected position. Assess for any residual plantar capsular adhesions; if the toe does not rest naturally in the corrected position, further capsular release is required.
- Flap Transposition and Closure: Transpose the two triangular limbs of the Z-plasty. The transposition will reorient the central limb transversely, effectively lengthening the dorsal skin. Suture the flaps with interrupted chromic or nylon sutures, ensuring minimal tension on the apical tips to prevent marginal necrosis.
SURGICAL TECHNIQUE: BUTLER ARTHROPLASTY
For more rigid or severe dorsally overriding fifth toes, the Butler arthroplasty provides a comprehensive release and realignment. Black et al. reported good to excellent results in 34 of 36 (94%) Butler arthroplasties performed for this specific deformity. The procedure utilizes a double racquet incision that acts as a V-Y advancement flap, combined with extensive capsular and tendinous releases.
Surgical Warning: A primary complication of the Butler arthroplasty is the potential for vascular damage caused by excessive tension on the neurovascular bundle during derotation and plantarflexion of the toe. Ischemia can lead to partial or complete loss of the digit.
To prevent vascular complications, the surgeon must adhere to three critical principles:
1. Avoid any longitudinal tension on the neurovascular bundle during dissection.
2. Take extreme care not to manipulate or exert excessive traction on the toe during the capsular release.
3. Strictly avoid the use of circumferential taping or rigid splinting postoperatively.
Step-by-Step Surgical Approach (Butler Technique)
- Incision and Exposure: After preparing and draping the foot and applying a tourniquet, make a double racquet incision. The dorsal handle of the racquet should follow the course of the extensor longus tendon, while the plantar handle is inclined laterally to provide a circumferential incision around the base of the fifth toe.
- Flap Elevation: To expose the contracted extensor tendon, elevate the skin flaps by careful blunt dissection. It is imperative to identify and protect the digital neurovascular bundles, which lie in close proximity to the plantar aspect of the incision.
- Deep Dissection: Transect the extensor tendon to the fifth toe. Proceed to divide the dorsal aspect of the metatarsophalangeal joint capsule completely.
- Derotation and Plantar Release: Following the dorsal release, the toe should partially rotate downward and laterally into the correct position. However, in long-standing deformities, the plantar aspect of the capsule becomes highly adherent and prevents full reduction of the proximal phalanx onto the metatarsal head during derotation.
- Plantar Capsulotomy: If necessary, separate the adherent plantar capsule from the metatarsal head by blunt dissection. Divide it transversely to allow the toe to lie freely in a fully corrected, neutral position without any springing back.
- Closure: The design of the double racquet incision allows the dorsal skin defect to close in a V-Y fashion, accommodating the new plantarflexed position of the toe. Close the skin with multiple interrupted non-absorbable sutures.
- Dressing: Apply a light, non-constricting dressing to the suture line. No rigid splint or cast is necessary, and circumferential wraps must be strictly avoided.
COMPLEX CONGENITAL DEFORMITIES: CLEFT FOOT CLOSURE
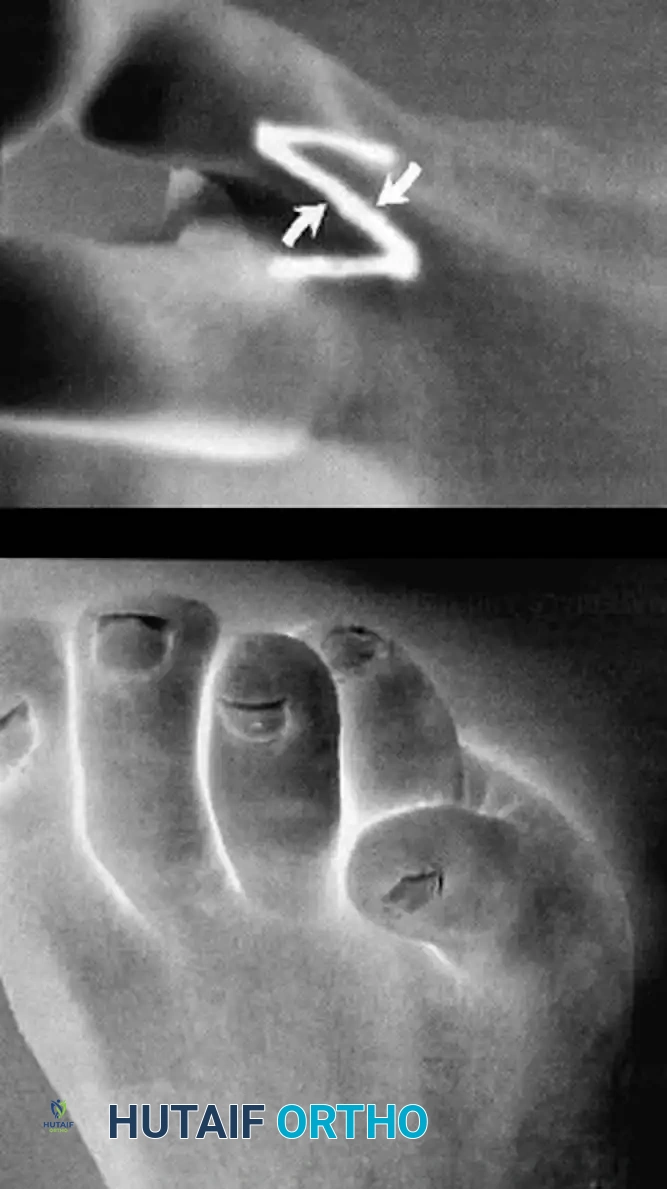
While contractures of the fifth toe represent a common isolated anomaly, orthopedic surgeons must also be prepared to manage complex syndromic or structural forefoot deformities, such as the cleft foot (ectrodactyly). Cleft foot is a rare congenital anomaly characterized by the absence of one or more central rays, resulting in a deep V-shaped cleft that severely impairs both foot biomechanics and aesthetics.
Wood, Peppers, and Shook described a simplified, highly effective technique for cleft foot closure that restores the transverse metatarsal arch and creates a functional, cosmetically acceptable web space.
Step-by-Step Surgical Approach (Cleft Foot Closure)
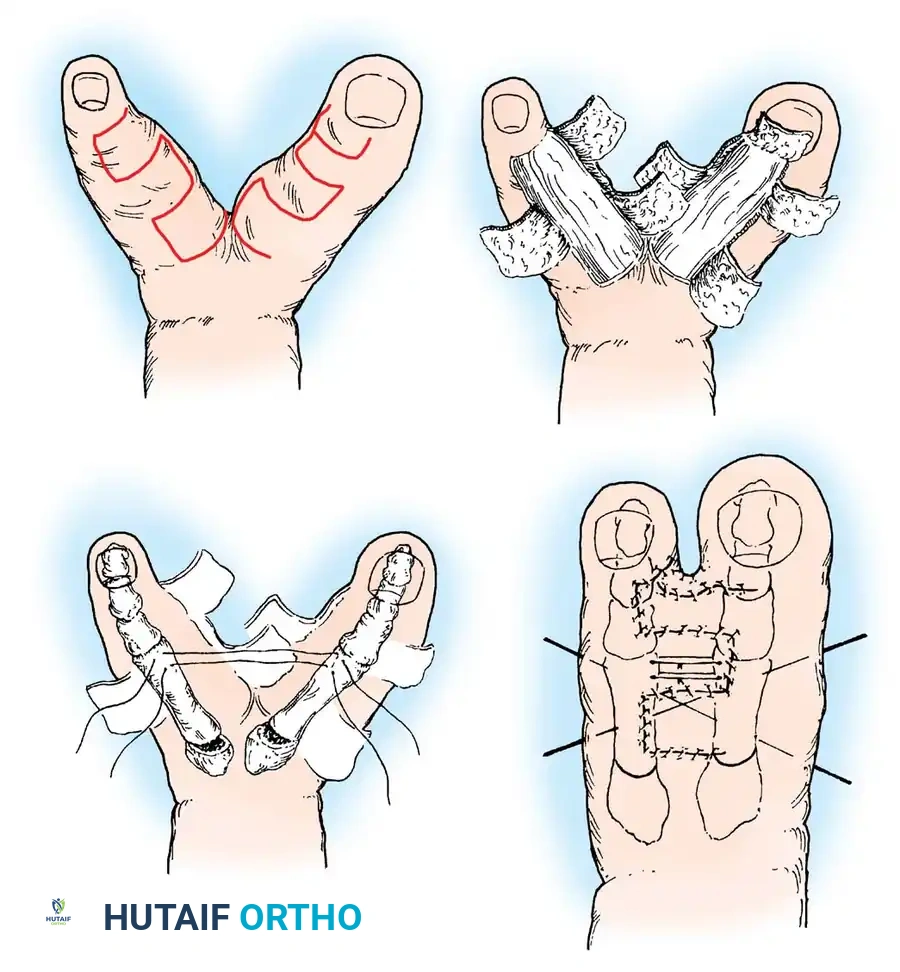
- Flap Design: Rectangular flaps are meticulously raised on the opposing surfaces of the rays bordering the cleft. The design must account for the final web space depth to prevent distal migration of the commissure (syndactylization).
- Cleft Excision: The flaps are raised proximally until the skin of the entire cleft is completely removed. At the distal tip of the longer toe bordering the cleft, a specialized flap is raised to suture to the adjacent toe, ensuring the creation of a wide, natural-appearing toe web.
- Osseous Realignment: Soft-tissue closure alone is often insufficient due to the divergent vector forces of the remaining metatarsals. If the toes spring apart upon attempted closure, a closing wedge osteotomy is made at the base of each bordering metatarsal. This centralizes the bones and narrows the forefoot.
- Fixation: Smooth Kirschner wires (K-wires) are inserted longitudinally across the osteotomy sites and transversely across the metatarsal heads to maintain the centralized position during osseous union and soft-tissue healing.
Clinical Pearl: When performing closing wedge osteotomies for cleft foot closure, ensure the plantar cortices of the metatarsals remain intact to act as a hinge. This enhances the stability of the osteotomy and promotes rapid primary bone healing.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management following surgical correction of toe contractures is designed to protect the soft-tissue reconstruction while preventing vascular compromise.
- Immediate Postoperative Care: A short leg cast or a rigid postoperative surgical shoe is applied. For isolated fifth toe procedures (Z-plasty or Butler arthroplasty), only a light, non-adherent dressing is placed over the digit.
- Vascular Monitoring: Capillary refill and toe turgor must be assessed immediately after tourniquet deflation and monitored closely in the recovery room. If vascular compromise is noted, all dressings must be loosened, and the toe may need to be slightly plantarflexed to relieve tension on the digital arteries.
- Weight-Bearing Status: Protected weight-bearing activity is allowed as tolerated in a hard-soled surgical shoe. For patients who underwent cleft foot closure with metatarsal osteotomies, strict non-weight-bearing status is maintained for 4 to 6 weeks until radiographic evidence of bone healing is observed.
- Suture Removal: Skin sutures are typically removed at 14 to 21 days, depending on the tension of the closure and the patient's healing capacity.
- Long-Term Follow-Up: Patients are advised to wear wide-toe-box footwear to prevent extrinsic pressure on the surgical site. Recurrence is rare if the capsular and tendinous releases were comprehensive, but patients should be monitored for hypertrophic scarring or residual rotational malalignment.
You Might Also Like