Radiographic Evaluation of Shoulder Instability | Orthopaedic Masterclass
Key Takeaway
Accurate radiographic evaluation is paramount in diagnosing and managing shoulder instability. While history and clinical examination establish the foundation, precise imaging—ranging from specialized plain radiographs like the West Point and Stryker notch views to advanced 3D CT and MR arthrography—dictates surgical decision-making. This guide details the indications, patient positioning, and biomechanical rationale for quantifying glenoid bone loss and identifying capsulolabral defects to optimize postoperative outcomes.
INTRODUCTION TO RADIOGRAPHIC EVALUATION IN SHOULDER INSTABILITY
The diagnosis of an unstable shoulder is fundamentally established through a meticulous clinical history and physical examination; however, the definitive documentation, quantification of pathology, and subsequent surgical planning rely entirely on a comprehensive radiographic evaluation. The glenohumeral joint, possessing the greatest range of motion of any articulation in the human body, achieves this mobility at the expense of intrinsic osseous stability. Consequently, when stabilizing mechanisms fail, the resulting capsulolabral and osseous defects must be precisely mapped.
Initial radiographic examinations serve as the baseline to rule out gross dislocations, fractures, and degenerative changes. When standard views are inconclusive, the orthopaedic surgeon must employ specialized radiographic projections, gadolinium-enhanced Magnetic Resonance Imaging (MRI), or Computed Tomography (CT) arthrography. These advanced modalities are critical for identifying posttraumatic changes—such as bipolar bone loss (Hill-Sachs and bony Bankart lesions)—that dictate whether a soft-tissue stabilization (e.g., arthroscopic Bankart repair) or a bony augmentation procedure (e.g., Latarjet) is indicated.
Clinical Pearl: Failure to recognize and quantify critical glenoid bone loss is the leading cause of recurrent instability following isolated arthroscopic soft-tissue repair. A high index of suspicion and appropriate advanced imaging are mandatory in the preoperative workup.
CLINICAL CORRELATION: THE BEIGHTON HYPERLAXITY SCORE
Before delving into imaging, the radiographic findings must be contextualized within the patient's intrinsic collagenous makeup. Generalized ligamentous laxity significantly alters the surgical approach, often necessitating robust capsular plication or shift alongside labral repair. The Beighton Hyperlaxity Score is the gold standard for quantifying systemic laxity.
A score of ≥ 4 points on this 9-point scale is diagnostic of hyperlaxity. The scoring system is evaluated as follows:
- Passive dorsiflexion of the little finger beyond 90 degrees: 1 point for each hand.
- Passive apposition of the thumb to the ipsilateral flexor forearm: 1 point for each hand.
- Active hyperextension of the elbow beyond 10 degrees: 1 point for each elbow.
- Active hyperextension of the knee beyond 10 degrees: 1 point for each knee.
- Forward flexion of the trunk: 1 point if the knees are fully extended and the palms of the hands rest flat on the floor.
Patients exhibiting high Beighton scores often present with multidirectional instability (MDI) or atraumatic subluxations. In these cohorts, imaging may reveal a patulous, voluminous inferior capsule without a discrete Bankart lesion, guiding the surgeon toward a capsular shift rather than a standard labral repair.
STANDARD RADIOGRAPHIC SERIES
The initial radiographic evaluation of any patient presenting with shoulder instability must include, at minimum, a true anteroposterior (Grashey) view and an axillary lateral view.
The True Anteroposterior (Grashey) View
Unlike a standard AP of the shoulder, the Grashey view is taken with the patient rotated 30 to 45 degrees toward the affected side, aligning the X-ray beam perpendicular to the glenoid fossa. This provides a clear view of the glenohumeral joint space, allowing for the assessment of joint congruency, subtle subluxations, and the presence of glenoid rim fractures.
The Axillary Lateral View
The axillary lateral view is non-negotiable in the trauma setting. It definitively establishes the relationship of the humeral head to the glenoid (anterior vs. posterior dislocation) and can identify large Hill-Sachs lesions or anterior glenoid rim deficiencies.
SPECIALIZED RADIOGRAPHIC PROJECTIONS
When routine views fail to fully delineate the extent of osseous injury, specialized views obtained in the office setting become invaluable. The most common and clinically relevant special views include the AP in internal rotation, the apical oblique (Garth) view, the West Point view, and the Stryker notch view.
Anteroposterior View in Internal Rotation
An AP radiograph of the shoulder taken in maximal internal rotation profiles the posterolateral aspect of the humeral head. This view frequently unmasks a Hill-Sachs lesion—an impaction fracture caused by the humeral head striking the anterior glenoid rim during an anterior dislocation—that may remain entirely occult on standard external rotation or neutral views.
The Apical Oblique (Garth) View
Described by Garth et al., the apical oblique radiograph is highly effective for visualizing posterior humeral head defects and evaluating the anteroinferior glenoid rim.
Positioning and Technique:
With the patient seated and the injured shoulder adjacent to a vertical cassette, the chest is rotated into a 45-degree oblique position. The X-ray beam is directed 45 degrees caudally, passing longitudinally through the scapula, which rests at a 45-degree angle on the thorax while the extremity is adducted.
Surgical Warning: The origin of the coracoid process, appearing midway between the anterior and posterior margins of the glenoid on this view, serves as a critical landmark for orientation. This view is particularly useful in the acute trauma setting for patients who cannot tolerate the abduction required for an axillary view, easily identifying locked posterior dislocations.
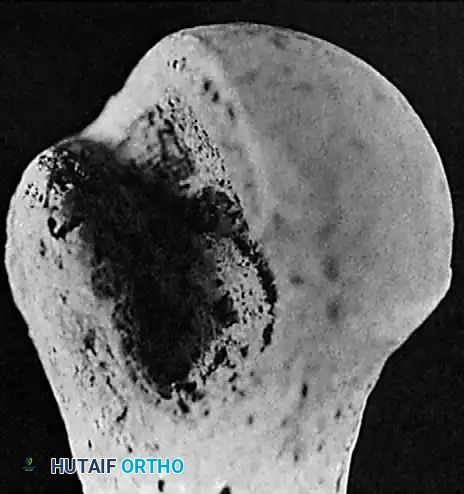
The West Point (Rokous) View
The West Point view is a specialized projection specifically designed to identify calcification, heterotopic ossification, or small fractures at the anteroinferior glenoid rim (the classic bony Bankart lesion).
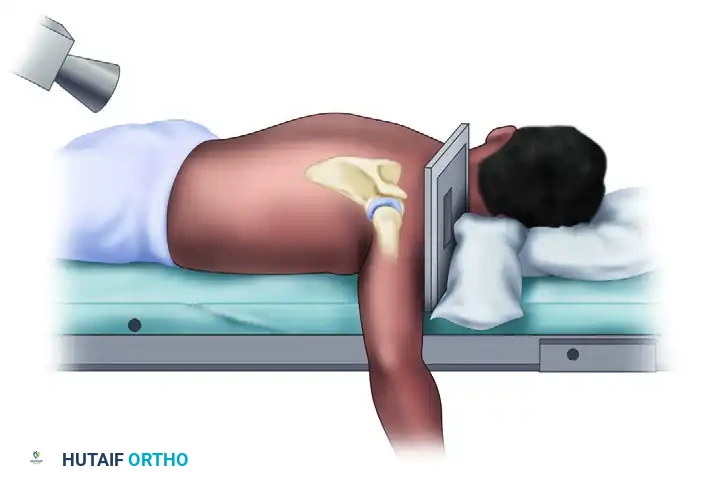
Positioning and Technique:
This is a modified, prone, axillary lateral view. The patient is placed prone with a pillow beneath the shoulder to elevate it. The shoulder is abducted 90 degrees, and the elbow is flexed with the arm hanging over the side of the examination table. The cassette is placed superior to the shoulder, perpendicular to the table. The X-ray beam is directed 25 degrees medially (toward the midline) and 25 degrees cephalad (toward the head).
This tangential projection perfectly profiles the anteroinferior quadrant of the glenoid, making it highly sensitive for detecting subtle bone loss that might be missed on a standard axillary view.
The Stryker Notch View
The Stryker notch view is the definitive plain radiograph for identifying and characterizing posterolateral humeral head defects (Hill-Sachs lesions).
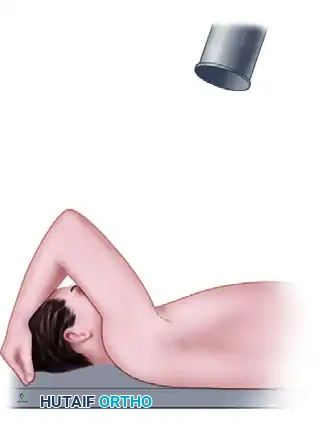
Positioning and Technique:
The patient is positioned supine on the radiography table. The affected arm is elevated, and the elbow is flexed so that the patient's hand rests on top of their head. The X-ray beam is directed 10 degrees cephalad, centered over the coracoid process.
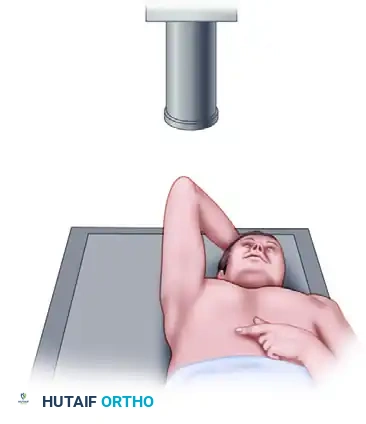
By elevating the arm, the posterolateral aspect of the humeral head is brought into profile. This view allows the surgeon to assess the depth and width of the Hill-Sachs lesion, which is critical for determining if the lesion is "engaging" and whether a remplissage procedure (capsulotenodesis of the infraspinatus into the defect) is required.
ADVANCED CROSS-SECTIONAL IMAGING
While plain radiographs provide excellent initial data, advanced cross-sectional imaging is mandatory for precise preoperative planning, particularly in cases of recurrent instability, failed prior stabilization, or suspected significant bone loss.
Computed Tomography (CT) and 3D Reconstruction
CT, particularly with three-dimensional (3D) surface-rendered reconstructions and humeral head subtraction, is the most sensitive and accurate test for detecting and measuring bone deficiency. It is the gold standard for evaluating the version of the glenoid and humerus.
Indications for CT Imaging:
* Blunting or loss of the sclerotic line of the anterior glenoid cortical outline on plain radiographs.
* Obvious bone defects noted on initial X-rays.
* Recurrent instability occurring with trivial trauma or during sleep.
* Low-angle instability (dislocation occurring with the arm in adduction).
* Evaluation of failed prior surgical stabilization procedures.
Quantification of Glenoid Bone Loss
Accurate quantification of glenoid bone loss is paramount. The "glenoid track" concept dictates that if the combined bipolar bone loss exceeds critical thresholds (historically >20%, but modern literature suggests >13.5% in high-demand athletes), soft-tissue repair alone carries an unacceptably high failure rate, necessitating a coracoid transfer (Latarjet procedure) or iliac crest bone grafting.
The Provencher Method (Best-Fit Circle):
Glenoid bone loss is best estimated using an en face view of the glenoid on a 3D CT scan with the humerus digitally subtracted.
- The longitudinal axis and the widest anteroposterior diameter of the lower half of the glenoid are identified.
- The intersection of these axes approximates the "bare spot" of the glenoid fossa.
- A best-fit circle, centered at the bare-spot approximation, is drawn outlining the inferior two-thirds of the glenoid.
- Distances from the bare spot to the anterior rim (A) and the posterior rim (B) are measured.
The percentage of bone loss is calculated using the following equation:
Percent Bone Loss = [(B – A) / (2 × B)] × 100%
Surgical Pearl: Always evaluate the glenoid en face. Relying solely on axial 2D CT slices can lead to overestimation or underestimation of bone loss due to variations in scapular tilt and version. The 3D reconstruction provides a true anatomical representation of the articular surface available for humeral head articulation.
Double-Contrast CT Arthrography
Standard double-contrast arthrography of the shoulder may be useful if excessive capsular capacity with an enlarged axillary pouch is suspected. However, Double-Contrast CT Arthrography represents a significant upgrade. It is especially useful in patients without clear-cut clinical signs of frank subluxation or dislocation, but who present with pain, clicking, and vague discomfort suggestive of microinstability.
CT arthrography effectively demonstrates bony lesions (Hill-Sachs, glenoid rim fractures) while simultaneously highlighting soft tissue abnormalities. It is easier to perform than a standard fluoroscopic arthrogram, and the radiation dose is 5 to 10 times less. It is highly sensitive for showing labral defects, capsular stripping, and articular cartilage damage.
MAGNETIC RESONANCE IMAGING (MRI) AND MR ARTHROGRAPHY (MRA)
MRI, particularly when enhanced with intra-articular gadolinium (MRA), provides the best minimally invasive visualization of capsular, ligamentous, and labral damage.
Indications and Findings
MRI obtained within a few days of an acute dislocation generally shows a large hemarthrosis. This intra-articular blood acts as a natural contrast agent, often making an invasive MRA unnecessary in the acute setting.
In the chronic setting, MRA is the modality of choice for evaluating soft tissue lesions associated with instability, including:
* Classic Bankart Lesions: Avulsion of the anteroinferior labrum and capsule from the glenoid rim.
* ALPSA Lesions: Anterior Labroligamentous Periosteal Sleeve Avulsion. The labrum remains attached to the periosteum but is displaced medially and inferiorly down the glenoid neck.
* Perthes Lesions: The labrum is detached from the glenoid but the periosteal sleeve remains intact, often requiring an ABER (Abduction External Rotation) view to visualize the stripping.
* HAGL Lesions: Humeral Avulsion of the Glenohumeral Ligament. MRA is highly helpful in evaluating HAGL lesions, which present as a "J-sign" on coronal oblique images. These lesions require specific surgical repair, often necessitating an open approach or advanced arthroscopic techniques.
Pitfall: While MRA is excellent for HAGL lesions, the injected contrast may occasionally extravasate and obscure the exact details of the tear site. Close consultation with a musculoskeletal radiologist is recommended to ensure protocols include ABER views, which place the inferior glenohumeral ligament under tension, unmasking subtle anteroinferior labral detachments.
Sensitivity Considerations
It is important for the orthopaedic surgeon to recognize the limitations of imaging. Recent literature comparing preoperative MRI with gold-standard arthroscopic examination has shown that the sensitivity of MRI for detecting certain subtle labral defects may be lower than previously cited. Therefore, imaging must always be correlated with the patient's history, physical examination (e.g., apprehension and relocation tests), and examination under anesthesia (EUA) prior to making the final surgical incision.
CONCLUSION AND SURGICAL DECISION-MAKING
The radiographic evaluation of the unstable shoulder is a highly structured, stepwise process. It begins with standard AP and axillary views to rule out gross pathology. When subtle instability or bone loss is suspected, specialized views such as the West Point and Stryker notch projections provide critical diagnostic data in the clinic.
Ultimately, advanced imaging dictates the surgical algorithm. 3D CT is the undisputed gold standard for quantifying glenoid and humeral bone loss, directly influencing the choice between soft-tissue stabilization and bony augmentation. Concurrently, MR Arthrography maps the soft-tissue landscape, identifying complex capsulolabral tears and HAGL lesions. By mastering these radiographic modalities, the orthopaedic surgeon ensures a precise, evidence-based approach to restoring stability, biomechanics, and function to the glenohumeral joint.
You Might Also Like