Comprehensive Physical Examination of Shoulder Instability

Key Takeaway
A systematic physical examination is paramount in diagnosing shoulder instability. This comprehensive guide details the biomechanical evaluation of the glenohumeral joint, including provocative testing for anterior, posterior, and multidirectional instability. By mastering techniques such as the Jobe relocation test, sulcus sign, and dynamic scapular assessment, orthopedic surgeons can accurately differentiate capsulolabral pathology from structural bone loss, guiding precise surgical interventions.
INTRODUCTION TO THE UNSTABLE SHOULDER
The physical examination of a patient presenting with glenohumeral instability is a highly nuanced, dynamic process that requires a profound understanding of shoulder biomechanics, capsuloligamentous anatomy, and compensatory neuromuscular patterns. The glenohumeral joint inherently sacrifices osseous constraint for a maximized global range of motion, relying heavily on the dynamic stabilization of the rotator cuff and periscapular musculature, alongside the static restraints of the labrum and glenohumeral ligaments.
A masterful clinical examination not only confirms the diagnosis of instability but precisely delineates the direction, severity, and underlying pathoanatomy—be it soft-tissue capsulolabral failure, critical osseous defects, or generalized hyperlaxity. This systematic evaluation forms the cornerstone of surgical decision-making, dictating whether a patient requires an arthroscopic Bankart repair, a rotator interval closure, or a bony augmentation procedure such as a Latarjet.
INITIAL ASSESSMENT AND PATIENT HISTORY
The clinical evaluation begins before the examiner even touches the patient. A meticulous history provides critical clues regarding the etiology and direction of the instability. The surgeon must ascertain the specific arm position that provokes the instability, the perceived direction of the subluxation, and whether the patient can safely and voluntarily demonstrate the phenomenon.
Clinical Pearl: Always utilize the contralateral, asymptomatic shoulder as the patient’s physiologic baseline. Generalized ligamentous laxity is highly variable among individuals; what constitutes pathologic translation in one patient may represent normal physiologic translation in another.
Visual Inspection and Scapular Kinematics
Both shoulders must be thoroughly exposed and examined. The evaluation commences with a rigorous inspection for muscular atrophy or structural asymmetry. Particular attention should be paid to the deltoid, the supraspinatus, and the infraspinatus fossae.
Scapular dyskinesia or winging must be meticulously documented during both active range of motion and strength testing. Scapular winging frequently indicates profound weakness or neurologic deficit of the periscapular stabilizers (e.g., serratus anterior or trapezius).
* Dynamic Scapular Evaluation: Winging can be dynamically provoked and evaluated by instructing the patient to perform a press-up maneuver from the examination table or an incline-type push-up against a wall.
* Surgical Implication: Scapular dysfunction is a potent contributor to secondary impingement and functional instability. It must be identified early, as it often necessitates a dedicated preoperative physical therapy protocol focusing on periscapular rehabilitation prior to any surgical intervention.
PALPATION AND RANGE OF MOTION (ROM)
Following inspection, systematic palpation is performed to localize capsular or tendinous pathology. The examiner must determine the precise degree and anatomical location of tenderness across the anterior capsule, posterior capsule, rotator cuff insertions, and the acromioclavicular (AC) joint.
Kinematic Evaluation
Active and passive ranges of motion must be evaluated with the patient in both the upright (seated or standing) and supine positions.
* Upright Evaluation: Assesses the patient's functional biomechanics and compensatory scapulothoracic motion.
* Supine Evaluation: Crucial for isolating true glenohumeral motion by stabilizing the scapula against the examination table, thereby eliminating scapulothoracic substitution.
Motion must be accurately recorded in all planes: forward flexion, abduction, and external/internal rotation at both 0 degrees and 90 degrees of abduction.
Neuromuscular Strength Profiling
The strength of the deltoid, rotator cuff, and scapular stabilizers must be systematically evaluated, recorded, and graded on the standard Medical Research Council (MRC) scale from 0 to 5 (with 5 representing normal physiological strength). Weakness may indicate concomitant nerve injury (e.g., axillary nerve palsy following an anterior dislocation) or a massive rotator cuff tear, particularly in older patients presenting with instability.
PROVOCATIVE TESTING FOR GLENOHUMERAL INSTABILITY
Stability testing is the crux of the physical examination. It requires a relaxed patient and a methodical approach to isolate specific capsuloligamentous structures.
The Shift and Load Test
Stability is initially evaluated with the patient in the upright position. The "shift and load" test is designed to assess the integrity of the glenoid concavity and the labral bumper.
1. Positioning: The examiner places one hand firmly along the medial border and spine of the scapula to stabilize it.
2. Execution: The contralateral hand grasps the proximal humerus, applying a controlled, axially directed compressive force to center the humeral head within the glenoid fossa.
3. Translation: With the arm resting at 0 degrees of abduction, anterior and posterior translational forces are applied.
4. Interpretation: The examiner observes the amount of translation. Easy, frictionless subluxation of the humeral head over the glenoid rim strongly indicates a loss of the glenoid concavity (e.g., a significant bony Bankart lesion or severe labral deficiency), which almost universally mandates surgical reconstruction.
Inferior Instability: The Sulcus Test
The sulcus test evaluates the superior capsular structures and the inferior glenohumeral ligament complex. It must be performed at two distinct angles of abduction to isolate different anatomical restraints.
- Technique: The examiner applies a firm, distally directed traction force to the arm while observing the subacromial space for the appearance of a "sulcus" or dimple between the lateral edge of the acromion and the humeral head.
- Testing at 0 Degrees Abduction: A positive sulcus sign here primarily indicates laxity of the superior glenohumeral ligament (SGHL), the coracohumeral ligament (CHL), and the rotator interval.
- Testing at 45 Degrees Abduction: The test is repeated with the arm abducted to 45 degrees. If the sulcus persists and does not reduce with the addition of 45 degrees of external rotation, it indicates profound laxity of the inferior glenohumeral ligament (IGHL) complex.
Grading the Sulcus Sign:
The distance between the lateral acromion and the humeral head is objectively graded:
* Grade 0: No significant translation.
* Grade 1+: Less than 1 cm of inferior translation (mild subluxation).
* Grade 2+: 1 to 2 cm of inferior translation.
* Grade 3+: Greater than 2 cm of inferior translation, indicating severe multidirectional instability or profound capsular incompetence.
Anterior Instability Testing
Anterior Apprehension Test
The anterior apprehension test is the most sensitive clinical maneuver for diagnosing anterior glenohumeral instability.
1. Positioning: The patient's shoulder is placed in 90 degrees of abduction, and the elbow is flexed to 90 degrees.
2. Execution: The examiner applies a gentle, progressive external rotation force to the extremity while simultaneously applying an anteriorly directed stress to the proximal humerus.
3. Interpretation: A positive test is not merely the elicitation of pain, but a distinct, involuntary apprehension reaction or muscle guarding from the patient, anticipating an impending dislocation.
Surgical Warning: Absolute control of the proximal humerus must be maintained throughout all apprehension and stress tests. The examiner must be prepared to instantly release the external rotation stress to prevent an iatrogenic dislocation in the clinic setting.
The Jobe Relocation Test
The Jobe relocation test is an indispensable adjunct to the apprehension test, particularly valuable in evaluating overhead athletes (e.g., baseball pitchers, tennis players) who present with vague shoulder pain.
- Execution: With the patient supine and the shoulder in the apprehension position (90 degrees of abduction and maximal external rotation), anterior stress is applied to the posterior aspect of the proximal humerus.
- Provocation: If this maneuver produces pain or a feeling of apprehension, the examiner immediately applies a posteriorly directed force to the anterior humerus.
- Relocation: This posterior force effectively "relocates" the subluxated humeral head back into the center of the glenoid fossa.
- Interpretation: If the posteriorly directed stress abolishes the patient's pain and apprehension, it confirms that the primary pathology is anterior microinstability (often leading to secondary internal impingement), rather than primary rotator cuff tendinitis. If the posterior stress is suddenly released, the immediate return of apprehension or the sensation of subluxation definitively confirms anterior instability.
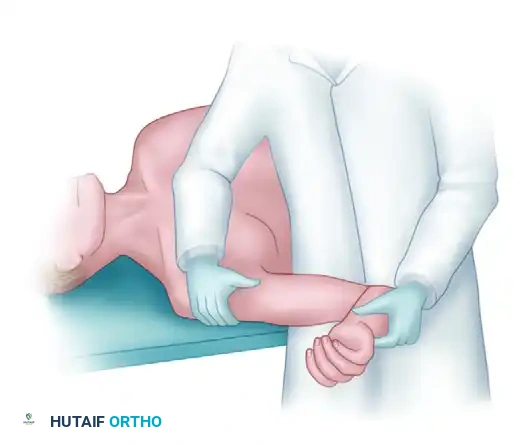
Supine Anterior Drawer Test
The anterior drawer test allows for a highly controlled assessment of anterior translation.
1. Positioning: The patient lies supine. The extremity is positioned in various degrees of abduction and external rotation within the plane of the scapula.
2. Execution (Right Shoulder Example): The examiner uses their left hand to firmly grasp the proximal humerus, while the right hand lightly supports the patient's elbow. Anterior stress is applied directly to the proximal humerus.
3. Assessment: The examiner evaluates both the absolute amount of translation and the quality of the capsular "end point."
Standardized Grading System for Translation (Anterior and Posterior):
* Grade 0: Normal physiologic translation.
* Grade 1: The humeral head translates up to, but not over, the glenoid rim.
* Grade 2: The humeral head translates over the glenoid rim (labrum) but spontaneously relocates once the stress is removed.
* Grade 3: The humeral head translates over the rim and remains dislocated, requiring manual reduction.
Clinical Pearl: A Grade 3 instability pattern should almost never be exhibited in an awake, unanesthetized patient due to involuntary muscle guarding. If Grade 3 translation is easily achieved in the clinic, it suggests profound, chronic capsular incompetence or massive structural bone loss.
Posterior Instability Testing
Posterior instability is less common but frequently missed. It requires specific provocative maneuvers designed to stress the posterior band of the IGHL and the posterior capsule.
Posterior Clunk Test
- Positioning: The patient's arm is initially placed in 90 degrees of abduction.
- Execution: The examiner brings the arm into a forward flexed, internally rotated position while simultaneously applying a posteriorly directed axial load through the elbow.
- Interpretation: A palpable or audible "clunk" is felt as the humeral head subluxes over the posterior glenoid rim. This maneuver reproduces the patient's pain or subjective feeling of instability.
Supine Posterior Drawer Test
- Execution (Right Shoulder Example): The patient is supine. The examiner's left hand is placed beneath the patient to stabilize the scapula and palpate the posterior joint line, acting as a buttress to prevent frank dislocation.
- Stress Application: The right hand grasps the patient's arm. Starting at 0 degrees of forward flexion and internal rotation, the arm is progressively elevated to 110 degrees of flexion. Throughout this arc, a posteriorly directed stress is applied.
- Interpretation: The degree of posterior translation is graded (0 to 3) using the same criteria as the anterior drawer test.
EVALUATING FOR HYPERLAXITY AND BONY DEFORMITY
Differentiating between traumatic structural instability and atraumatic multidirectional hyperlaxity is critical for surgical planning.
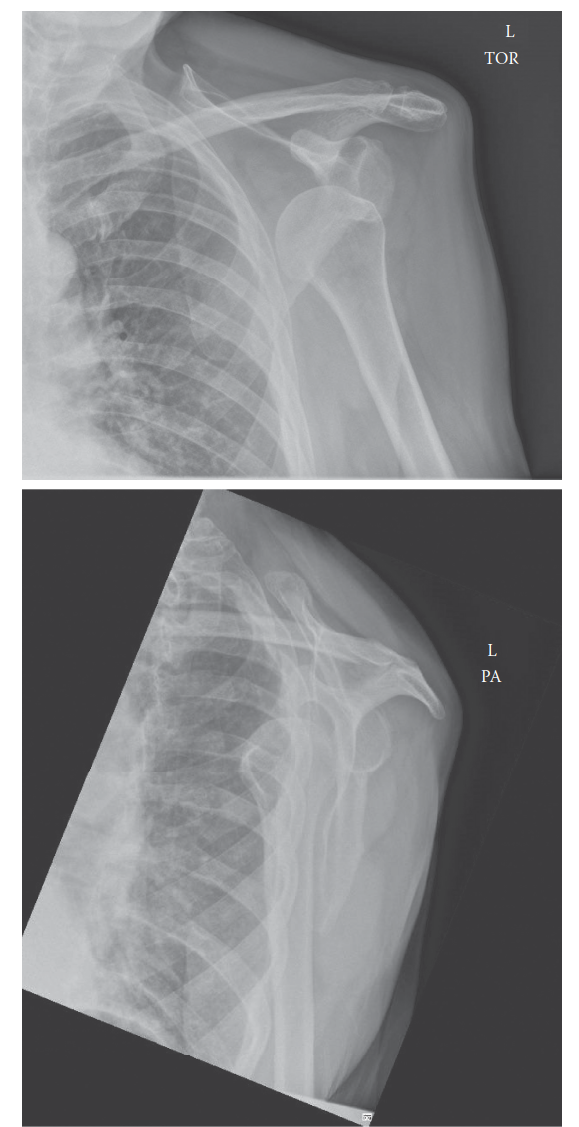
Indicators of Structural Bony Deformity
Bony deformity of the glenoid (e.g., an inverted pear glenoid) or the humerus (e.g., a massive engaging Hill-Sachs lesion) should be highly suspected if the patient exhibits apprehension or frank instability at low ranges of motion (specifically, less than 90 degrees of abduction). When inferior instability is disproportionately prominent alongside low-angle anterior apprehension, severe osseous deficiency must be ruled out via advanced imaging (3D CT scan).
Assessment of Generalized Hyperlaxity
Hyperlaxity is a systemic collagenous variance that profoundly impacts surgical success rates. It is indicated by:
1. A Positive Sulcus Test: As detailed previously.
2. The Gagey Hyperabduction Test: The examiner firmly stabilizes the scapula with one hand placed superiorly over the acromion, preventing scapulothoracic motion. The other hand passively abducts the patient's arm. A side-to-side difference of more than 20 degrees of passive abduction is highly suggestive of inferior capsular laxity.
3. Excessive External Rotation: Passive external rotation exceeding 85 degrees while the arm is resting at 0 degrees of abduction indicates profound anterior capsular and rotator interval laxity.
* Surgical Implication: Patients exhibiting this specific finding frequently require a formal rotator interval closure during arthroscopic stabilization to prevent recurrent instability.
4. The Beighton Hyperlaxity Scale: A systemic evaluation assessing hyperextension of the elbows, knees, fifth metacarpophalangeal joints, thumb-to-forearm apposition, and the ability to place palms flat on the floor with straight knees. A score of 4 or higher out of 9 indicates generalized joint hypermobility.
DIFFERENTIAL DIAGNOSIS AND PITFALLS
The unstable shoulder can mimic several other pathologies. It is imperative to distinguish secondary rotator cuff impingement (caused by the humeral head translating anteriorly and superiorly due to instability, impinging the cuff against the coracoacromial arch) from primary structural impingement (e.g., a type III hooked acromion). The Jobe relocation test is the definitive clinical tool for making this distinction in young athletes.
Furthermore, the examiner must maintain a high index of suspicion for cervical spine pathology. Although rarely the direct cause of true mechanical shoulder instability, cervical radiculopathy (e.g., degenerative disc disease or facet arthropathy) can cause profound pain radiating into the posterior or lateral aspect of the shoulder, accompanied by secondary muscle weakness that mimics instability-related dysfunction. A thorough neurologic examination of the upper extremities and a Spurling's test should be routinely incorporated to rule out cervical etiology.
You Might Also Like