Clinical Evaluation and History in Recurrent Shoulder Instability
Key Takeaway
A meticulous clinical history is the cornerstone of diagnosing recurrent shoulder instability. By evaluating the mechanism of initial trauma, the position of dislocation, and the presence of secondary rotator cuff impingement, orthopedic surgeons can differentiate between traumatic (TUBS) and atraumatic (AMBRII) etiologies. This comprehensive assessment dictates the necessity for advanced imaging and guides the definitive surgical or rehabilitative management of glenohumeral instability.
INTRODUCTION TO GLENOHUMERAL INSTABILITY
The glenohumeral joint possesses the greatest range of motion of any articulation in the human body, a biomechanical advantage achieved at the direct expense of intrinsic osseous stability. Consequently, it relies heavily on a complex interplay of static stabilizers (the capsulolabral complex, glenohumeral ligaments, and negative intra-articular pressure) and dynamic stabilizers (the rotator cuff musculature and periscapular stabilizers). When this delicate equilibrium is disrupted, recurrent instability ensues.
In the evaluation of recurrent instability of the shoulder joint, a meticulous and structured clinical history is paramount. It not only dictates the trajectory of the physical examination and advanced imaging but also serves as the primary determinant in formulating a definitive surgical or rehabilitative strategy. The history must systematically deconstruct the initial index event, the pattern of recurrence, associated neurological symptoms, and the specific functional limitations imposed upon the patient.
THE INDEX EVENT: MECHANISM OF INITIAL TRAUMA
The amount of initial trauma, if any, must be precisely determined. The etiology of the first dislocation provides critical prognostic information regarding the underlying capsulolabral and osseous pathology.
High-Energy Trauma
High-energy traumatic events, such as collision sports (e.g., rugby, American football, ice hockey) and motor vehicle accidents, are strongly associated with an increased risk of significant structural damage.
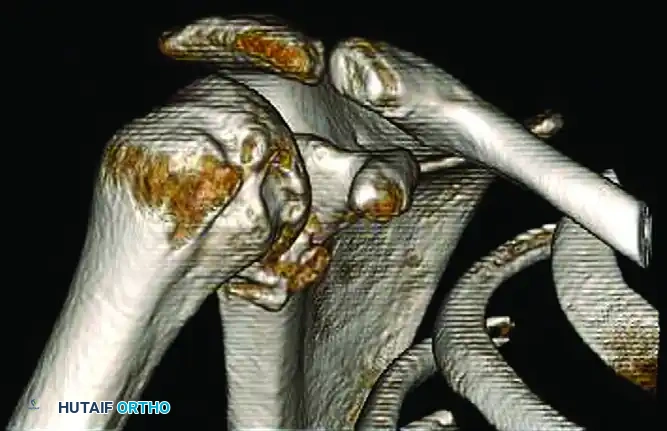
* Osseous Lesions: High-velocity impacts frequently result in glenoid bone loss (bony Bankart lesions) or substantial humeral head impaction fractures (Hill-Sachs lesions).
* Soft Tissue Disruption: These events typically cause catastrophic failure of the anterior-inferior capsulolabral complex, often necessitating surgical intervention to restore stability.
Surgical Warning: A history of a high-energy index dislocation should immediately raise the surgeon's index of suspicion for bipolar bone loss. Failure to recognize and address critical glenoid bone loss (typically >13.5% to 20%) or an off-track Hill-Sachs lesion will result in an unacceptably high rate of failure following an isolated arthroscopic soft-tissue Bankart repair.
Low-Energy and Atraumatic Events
Conversely, an initial dislocation occurring with minimal trauma, or insidiously without a discrete traumatic event, suggests underlying generalized ligamentous laxity, capsular redundancy, or connective tissue disorders (e.g., Ehlers-Danlos or Marfan syndrome).
CHRONICITY AND RECURRENCE PATTERNS
The characteristics of subsequent instability episodes are equally critical. The surgeon must elicit the specific arm positions that provoke instability, the frequency of events, and the ease of reduction.
Provocative Positioning
The position in which the dislocation or subluxation occurs provides a direct biomechanical vector for the instability:
* Anterior Instability: Typically occurs with the arm in abduction and external rotation (ABER).
* Posterior Instability: Typically occurs with the arm in flexion, adduction, and internal rotation (FADIR), often combined with an axial load.
* Inferior Instability: Provoked by carrying heavy objects at the side or during hyperabduction.
Mid-Range Instability
Recurrence with minimal trauma in the midrange of motion is a highly concerning historical feature. Mid-range instability implies a catastrophic loss of the static osseous restraints. It is almost exclusively associated with significant bony lesions (large glenoid defects or engaging Hill-Sachs lesions) that have compromised the "glenoid track." These structural deficits must be treated surgically, often requiring bone-grafting procedures such as the Latarjet procedure, iliac crest bone grafting, or distal tibial allografting.
Sleep and Overhead Dislocations
Dislocations that occur during sleep or with the arm resting in an overhead position are hallmark indicators of profound structural incompetence. These events are often associated with a significant anterior glenoid defect or severe capsular insufficiency that requires surgical treatment. The inability of the shoulder to maintain concentric reduction at rest or during unconscious, low-stress states precludes successful non-operative management.
The Mechanics of Reduction
In complete dislocations, the ease with which the shoulder is relocated must be determined.
* Self-Reduction: Dislocations that are reduced spontaneously by the patient often represent subluxations rather than true complete dislocations, or they are associated with profound generalized ligamentous laxity.
* Emergency Department Reduction: Episodes requiring intravenous sedation, intra-articular analgesia, or closed reduction by a physician typically indicate a true traumatic dislocation with robust muscle spasm and a competent, albeit torn, capsular hinge.
SUBLUXATION VS. DISLOCATION: THE CLINICAL SPECTRUM
Recurrent subluxation of the shoulder is commonly overlooked by physicians because the symptoms are often vague, and there is no history of an actual, documented dislocation requiring formal reduction.
Patient Presentation of Subluxation
The patient may complain of a transient sensation of the shoulder "sliding in and out of place," or they may not be consciously aware of any overt shoulder instability. Instead, they may present with secondary symptoms that mask the underlying micro-instability. It is imperative to document the specific physical limitations caused by this instability, such as the inability to throw, serve in tennis, or perform occupational overhead tasks.
The "Dead Arm" Syndrome
A classic presentation of recurrent subluxation is the "dead arm" syndrome. The patient complains of a sudden, sharp pain accompanied by profound weakness and a heavy, paralyzed sensation in the affected extremity, typically occurring during the acceleration or late cocking phase of throwing. This phenomenon is primarily the result of:
1. Neurological Traction: Transient stretching or neurapraxia of the axillary nerve or the cords of the brachial plexus as the humeral head subluxates anteriorly.
2. Secondary Rotator Cuff Inhibition: Reflexive inhibition of the rotator cuff musculature secondary to capsulolabral pain and micro-trauma.
Clinical Pearl: Always elicit the signs and symptoms of any nerve injury following an instability event. Axillary nerve neuropraxia is the most common neurological complication, presenting as numbness over the lateral deltoid (regimental badge area) and weakness in shoulder abduction. While most cases resolve spontaneously, baseline documentation is medicolegally and clinically mandatory.
ROTATOR CUFF PATHOLOGY IN THE UNSTABLE SHOULDER
A nuanced history is required to differentiate primary rotator cuff disease from secondary rotator cuff symptoms induced by underlying instability. Rotator cuff symptoms frequently develop secondary to ligamentous dysfunction and capsular laxity.
Primary vs. Secondary Impingement
- Primary Impingement: Typically occurs in older patients (>40 years) due to structural narrowing of the subacromial space (e.g., acromial spurring, osteoarthritis of the acromioclavicular joint).
- Secondary Impingement: Occurs in younger patients (<35 years). Anterior capsular laxity allows the humeral head to translate anteriorly and superiorly during overhead motion, causing the rotator cuff to impinge against the coracoacromial arch. Treating the rotator cuff without addressing the underlying instability will lead to surgical failure.
Internal Impingement
Internal impingement is a distinct pathological entity characterized by the abutment of the undersurface of the posterior rotator cuff (supraspinatus and infraspinatus) against the posterior-superior glenoid and labrum.
* Mechanism: It is caused by anterior humeral micro-subluxation with the shoulder in extreme external rotation and abduction (the late cocking phase of throwing).
* Demographics: This secondary impingement is significantly more common than primary subacromial impingement in patients younger than 35 years old who are involved in upper extremity–dominant sports (e.g., baseball pitchers, volleyball players, tennis players).
POSTERIOR SHOULDER INSTABILITY
Posterior shoulder instability is far less common than anterior instability, accounting for approximately 2% to 10% of all shoulder instability cases. Because it rarely presents as an acute, locked dislocation (unless associated with seizures, electrocution, or high-energy trauma), it is frequently misdiagnosed.
Clinical Presentation
Posterior instability typically presents insidiously as posterior shoulder pain, deep joint aching, or fatigue with repeated activity, rather than a frank sensation of instability.
At-Risk Populations
The history will often reveal participation in sports or occupations requiring repetitive posterior-directed forces on a flexed, internally rotated arm. Classic examples include:
* Blocking in American football (offensive linemen).
* Swimming (particularly the catch phase of the freestyle or butterfly stroke).
* Weightlifting (specifically the bench press).
* Rowing.
* Occupations requiring heavy pushing or overhead arm movement.
CLASSIFICATION SYSTEMS AND DIAGNOSTIC AMBIGUITY
To synthesize the historical data, orthopedic surgeons have historically relied on several classification systems. The two most ubiquitous acronyms in shoulder instability are TUBS and AMBRII, originally popularized by Thomas Matsen.
The TUBS and AMBRII Dichotomy
- TUBS: Traumatic etiology, Unilateral presentation, Bankart lesion is the defining pathology, and Surgery (Bankart repair) is the definitive treatment.
- AMBRII: Atraumatic etiology, Multidirectional instability, Bilateral findings (generalized laxity), Rehabilitation is the first-line treatment, and if surgery is required, an Inferior capsular shift and Rotator interval closure are necessary.
While conceptually elegant, modern orthopedic practice recognizes that many patients fall into a "gray zone" between these two extremes (e.g., a patient with underlying hyperlaxity who sustains a traumatic dislocation).
Variations in Defining Multidirectional Instability (MDI)
The diagnosis of Multidirectional Instability (MDI) remains highly dependent on the specific classification system utilized by the clinician. A landmark study by McFarland et al. (2003) highlighted the profound effect of variation in definition on the diagnosis of MDI.
Neer's Classification
In the classification system proposed by Charles Neer, MDI was not explicitly defined as a separate, isolated group. Instead, etiological factors were used as the defining criteria for a three-category system: Atraumatic, Traumatic, and Acquired. When applying Neer's strict original criteria to a cohort of 168 patients, only 1.2% (2 patients) met the diagnosis for MDI.
Alternative Classification Systems
When the same cohort of 168 patients was analyzed using other established classification systems, the prevalence of MDI varied significantly:
* Matsen et al.: Categorized 80 patients as TUBS, 7 patients (4.2%) as AMBRII, and 81 patients did not fit either strict category.
* Allen's Classification: Divided instability into Anterior (108), Posterior (10), and Multidirectional (13). Allen further subclassified MDI into Type I (global), Type II (anterior-inferior with hyperlaxity), Type III (posterior-inferior with hyperlaxity), and Type IV (anterior-posterior). Under Allen's criteria, 7.7% of the cohort had MDI.
* Gerber's Classification: A highly granular system that separates unidirectional instability (with or without hyperlaxity) from multidirectional instability (with or without hyperlaxity). Using Gerber's criteria, 8.3% of the cohort was diagnosed with MDI.
Academic Insight: The statistical differences between the classification system of Neer and Foster compared to Allen’s classification (P = 0.004) and Gerber’s classification (P = 0.001) were highly significant. This underscores a critical clinical reality: MDI is a heterogeneous spectrum rather than a monolithic diagnosis. The surgeon must rely on a comprehensive history of laxity, trauma, and functional deficit rather than forcing a patient into a rigid diagnostic algorithm.
CONCLUSION
The history of a patient with recurrent shoulder instability is a rich, diagnostic roadmap. By meticulously detailing the energy of the initial trauma, the biomechanical position of recurrence, the presence of mid-range or sleep dislocations, and the subtle symptoms of secondary rotator cuff impingement or "dead arm" syndrome, the orthopedic surgeon can accurately predict the underlying pathoanatomy. Understanding the nuances between traumatic structural failure and atraumatic capsular redundancy—and recognizing the limitations of historical classification systems—is essential for formulating a successful, patient-specific management plan.
You Might Also Like