How to Perform the Modified Ober's Test: A Complete Guide

Key Takeaway
For anyone wondering about How to Perform the Modified Ober's Test: A Complete Guide, The modified Obers test is a special hip examination technique designed to assess tightness in the iliotibial (IT) band and tensor fasciae latae (TFL) muscle. Classified under muscle and tendon tests, its purpose is to help diagnose conditions like IT band syndrome by evaluating hip abduction and extension limitations. It aids in comprehensive musculoskeletal assessment.
HIP EXAMINATION SPECIAL TESTS
CHAPTER
5
HIP
● A ARTICULAR TESTS
152
FAIR test 152
McCarthy test 156
FABER test 160
Torque test 163
Active straight leg raise (SLR) test 165
●
B
MUSCLE AND TENDON TESTS
166
Thomas’s test 166
Modified Ober’s test 170
Trendelenburg test 172
●
C
OTHER TESTS
175
Craig’s test 175
Sign of the buttock 177
151
●
A
ARTICULAR TESTS
FAIR test

Aka
Impingement test Posterior labral tear test Apprehension sign Piriformis test
Psoas test
Purpose
To reproduce pain and/or apprehension and increase the likelihood of detecting a range of conditions such as articular pathology (e.g. femoro-acetabular impingement (FAI), labral and hip joint pathology and instability), piriformis syndrome and psoas bursitis.
Technique
Patient position
Lying supine.
Clinician position
Standing on the affected side.
Action
The hip and knee are taken into 90° of flexion and then full internal rotation is added by applying a stabilizing pressure on the outside at the knee with the cephalic hand and drawing the lower leg outwards by using the heel as a lever with the caudal hand. The final component is adduction, achieved by passively moving the knee towards the opposite hip.
Positive test
Reproduction of the patient’s pain can be considered to be a positive test although the site of this will vary depending on the pathology.
1. ####
Articular pathology/psoas bursitis : pain in the groin which may be accompanied by a click if the labrum is involved.
2. ####
Piriformis syndrome : buttock or radicular pain.

Fig. 5.1 ● Flexion, adduction and internal rotation (FAIR) test.
Clinical context
The FAIR test gets its name from the acronym generated by the principal elements of this test (Flexion, Adduction and Internal Rotation). The list of possible structures that can be incriminated by a positive FAIR test naturally results in a test with low specificity. There is some evidence, however, that demonstrates its sensitivity in the diagnosis of labral pathology/impingement and piriformis syndrome (
Burnett et al
2006
,
Fishman et al
2002
,
Fitzgerald
1995
,
Hase & Ueo
1999
,
Jaberi & Parvizi
2007
,
Lewis & Sahrmann
2006
,
Mitchell et al
2003
,
Narvani et al
2003).
Most of the research comprises of small case series or larger retrospective studies of patients with known acetabular pathology or femoro-acetabular impingement (FAI). While the precise prevalence and cause of labral pathology is unknown, the population most likely to present is the younger patient with groin or hip pain (see McCarthy test, p. 156;
McCarthy & Busconi
1995
,
Narvani et al
2003
). A typical presentation would be a female patient in her mid-thirties with groin pain which is provoked by flexion activities such as driving or squatting and where certain movements are accompanied by a click. Some patients may also report lumbar or buttock pain provoked by activity, impact or load-bearing. There is a general lack of consensus concerning the significance of other findings such as a history of trauma, congenital or developmental hip abnormalities, movement impairment and radiological changes (
Burnett et al
2006
,
Fitzgerald
1995
,
Hase & Ueo
1999
,
Jaberi & Parvizi
2007
,
Lewis & Sahrmann
2006
,
Mitchell et al
2003
,
Narvani et al
2003).
Impingement, scour/quadrant (see Variations) and FABER tests (see p. 160) are all additional tests used to help the clinician determine the necessity of further investigation such as magnetic resonance arthrography (MRA) and arthroscopy.
The absence of an agreed ‘gold standard’ diagnostic tool for labral injury introduces uncertainty when attempting to measure the sensitivity of the test, as the significance of a positive finding on examination cannot always be confirmed definitively by means other than surgery, with investigations such as MRI and MRA being of limited value (
Standaert et al
2008
). In a retrospective study of 66 patients, the FAIR test was positive in 95% of patients with an arthroscopically confirmed labral tear compared to only 79% detected by MRA (
Burnett et al
2006
). These findings were confirmed in two separate case series (
Hase & Ueo
1999
,
Ito et al
2004). The lack of false negatives in these current studies prevents specificity being calculated. Although the FAIR test is part of the suggested examination for FAI there are several variations (see p. 155).
The use of the test for piriformis syndrome has been evaluated in
a large cohort trial of 918 patients which found that a positive FAIR test was a valid predictor of the response to physiotherapy, injection or surgical treatment for this condition (
Fishman et al
2002
). A study of 15 cases of surgically proven piriformis/sciatic nerve compression following blunt trauma concluded that the combination of a positive FAIR test along with a history of trauma, buttock pain and/ or radicular pain, intolerance to sitting and tenderness over the sci-atic notch were highly indicative of piriformis adhesions and should guide the need for referral for EMG (
Benson & Schutzer
1999).
TABLE 5.1 FAIR TEST
Author and year
|
LR +
|
LR —
|
Target condition
Fishman et al 2002
| 5.2
★★
| 0.14
★★
| Piriformis syndrome
Clinical tip
Placing the hip in flexion, adduction and internal rotation will cause either compression or stretch of many hip structures including the ischiofemoral ligament of the hip, iliopsoas tendon and bursa, pectineus, adductor longus, sartorius, tensor fascia lata, piriformis and the glutei. Inevitably the hip joint itself is tested and the findings
may help to isolate the first signs of joint pathology, such as Perthes’ disease in children for example (
Woods & Macnicol
2001). The FAIR test is not capable of distinguishing between specific structures or pathology and the clinician is reliant on other information gleaned from the patient including the history, other physical findings and the results of pertinent investigations.
EXPERT OPINION
|
COMMENTS
| ---|---|
★★
|
FAIR test
Useful as a non-specific test for a range of hip pathology. A diagnosis of femoro-acetabular impingement is likely if the patient’s symptoms are typical, the test is positive and they have a ‘C’ sign (when asked to indicate the area of pain, they grasp the area of the greater trochanter with their thumb and index finger).
Variations
The
scour/quadrant/flexion adduction test
is a modification where the hip is passively flexed to 90° and adducted. The clinician’s hands

Fig. 5.2 ● Scour test. The arrow indicates the direction of axial compression.
are interlocked and placed over the patient’s flexed knee. Leaning over the knee so that the examiner’s body weight can be used to good effect, a compressive force is applied through the longitudinal axis of the femur. Small passive movements are made into flexion and extension in order to ‘scour’ the joint (
Fig.
5.2). A positive test is indicated by reproduction of the patient’s symptoms.
TABLE 5.2 SCOUR TEST
Author and year
|
LR +
|
LR —
|
Target condition
Narvani et al 2003
| 1.32
| 0.58
| Labral tears

McCarthy test
-
Purpose
To reproduce pain and/or a ‘click’ in order to detect an acetabular labral tear. -
Technique
Patient position
Lying supine with the hips and knees flexed and both feet resting on the couch.
Clinician position
The affected hip is taken into full passive flexion, with one hand supporting the flexed knee and the other supporting the foot (see Fig. 5.3).
Action
External rotation is then added as the affected hip is gradually taken down towards extension (see Fig. 5.4). If this does not elicit a positive response, the manoeuvre is repeated with the addition of internal rotation instead.
Positive test
Reproduction of the patient’s hip pain or click. -
Clinical context
The role of the labrum in the symptomatic hip and the diagnosis of femoro-acetabular impingement (FAI) are comparatively new

Fig. 5.3 ● McCarthy test. Start position.

Fig. 5.4 ● McCarthy test. End position in external rotation. The test can then be repeated moving the hip into internal rotation.
areas of study and the evidence concerning the clinical diagnosis and the most appropriate investigations and treatment is uncertain. The labrum does have a propensity to degenerate with age and this was demonstrated in a cadaver study where degenerative
tears were identified in 90% of specimens ( McCarthy et al 2003 ). Interestingly, it is not the ageing population that report labral problems as the accompanying joint disease inevitably takes precedence. The younger patient with groin or hip pain is most likely to present and 22–55% of patients with this profile were found to have labral tears ( Narvani et al 2003). A typical presentation would be a female patient in her mid-thirties with groin pain which is provoked by flexion activities such as driving or squatting and where certain movements are accompanied by a click. Some patients may also report lumbar or buttock pain provoked by activity, impact or load-bearing.
Apart from surgical confirmation, there is no agreed ‘gold stand-ard’ diagnostic tool, with neither MR arthrography nor MRI showing sufficient sensitivity or specificity to confirm FAI ( Standaert et al 2008 ). The detection of FAI, labral tears or chondral lesions at the hip therefore largely relies on a combination of the history, signs and symptoms, the outcome of physical tests and imaging studies to guide both diagnosis and management. There has been shown to be some correlation, however, between acetabular tears and preoperative reports of clicking and giving way ( McCarthy & Busconi 1995 , Narvani et al 2003). -
Clinical tip
Acetabular tears may present in young, athletic patients where the predominant symptoms are groin pain, often accompanied by clicking, a catching sensation and/or giving way. A traumatic history involving hip flexion, abduction and knee extension is common ( DeAngelis & Busconi 2003 ), although not essential, as a significant proportion of patients in one study reported an insidious onset ( Burnett et al 2006).
EXPERT OPINION
| COMMENTS
| ---|---|
★★
| McCarthy test
Useful as a non-specific test for hip joint pathology. A positive test is not sensitive or specific for labral lesions. However, patients who report reproduction of their click and pain on this test seem to get better outcomes post surgery. -
Variations
The snapping hip test (sometimes known as the clicking hip test or the extension test ) is an active version of the McCarthy test and used to distinguish extra-articular snapping of the iliopsoas tendon as it passes over the femoral head or the iliopectineal eminence anteriorly. Iliopsoas syndrome is a source of groin pain and clicking and is most commonly encountered in young, athletic patients. It may also be associated with inflammatory or degenerative arthritis in the hip, or present post hip arthroplasty. The patient lies supine and actively brings the affected hip into a flexed, adducted and internally rotated position. The clinician places one hand over the anterior aspect of the hip joint to palpate for snapping. The other hand is then free to guide the movement of the patient’s leg downwards. The patient actively extends, abducts and externally rotates the hip from the starting position. A positive test is indicated by pain and reproduction of the patient’s familiar snapping sensation ( Magee 2008). Alternative causes of extra-articular snapping are the tensor fascia lata/gluteus maximus slipping over the greater trochanter and the iliofemoral ligament movement over the anterior joint capsule. -
Related tests
Other labral tests have attempted to identify the location of the tear ( Fitzgerald 1995). For the posterior labral tear test ( Fig. 5.5) the hip
A
B




Fig. 5.5 ● Start (A) and end position (B) of the posterior labral tear test.
is taken into in a flexed, adducted and internally rotated position ( Fig. 5.5A) and then passively moved into the reverse pattern of extension, abduction and external rotation ( Fig. 5.5B). The opposite manoeuvre is used for the anterior labral tear test . The hip starts in full flexion, external rotation and abduction and is then moved passively into extension, internal rotation and adduction. Pain and/ or clicking reproduced with either of these manoeuvres would be suggestive of a labral tear. Fitzgerald’s (1995) study prospectively examined patients with surgically verified labral pathology and although 54 of 55 patients reported a positive finding (pain and/or a click) on one of these tests, it was not possible to specifically isolate the exact site of the lesion.
EXPERT OPINION
| COMMENTS
| ---|---|
★
| Posterior labral tear test
The posterior labral tear test can be adapted so that the hip is taken into extension over the edge of the couch.
The log roll test can also be used to detect pathology of the acetabular labrum or identify hip joint laxity. The patient lies supine with the lower limbs relaxed in a neutral position. Standing on the affected side, the hands are positioned over the anterior aspect of the patient’s thigh, just above the knee. The thigh is then passively rolled into full internal rotation and then full external rotation. The test may elicit a click in the presence of a labral tear. An increase in the range of movement of the affected hip can indicate laxity ( Austin et al 2008; see torque test, p. 163).
EXPERT OPINION
| COMMENTS
| ---|---|
★★
| Log roll test
The log roll test can be useful as a general assessment for hip pathology. As the patient lies supine, excess external rotation caused by hip instability/laxity is indicated by the foot of the affected leg rolling outwards.

FABER test
-
Aka
The ‘4’ test Patrick’s test Jansen’s test -
Purpose
To test primarily for articular pathology in the hip joint. Also stresses the sacro-iliac joint (SIJ), iliopsoas tendon and the lumbar spine. -
Technique
Patient position
The patient lies supine and the affected leg is flexed and externally rotated so that the lateral aspect of the ankle is positioned just above the opposite knee joint. If this starting position is uncomfortable for the patient, the knee can be brought more into the midline to reduce hip abduction.
Clinician position
Standing at the patient’s affected side, the pelvis is stabilized by applying gentle pressure over the opposite anterior superior iliac spine.
Action
The patient is asked to lower the knee towards the couch and if full range is achieved, gentle overpressure can be applied to the medial aspect of the knee to assess full passive range and end-feel.

Fig. 5.6 ● Flexion, abduction and external rotation (FABER) test.
Positive test
A positive test is indicated by the reproduction of the patient’s pain or reduced range of movement. If the knee lowers to a point which is level to the opposite knee or the range is equivalent to the con-tralateral side, range is considered to be normal. -
Clinical context
The test position places the hip in Flexion, ABduction and External Rotation, giving the acronym FABER. Interpretation of the test can be difficult as the position adopted not only tensions the hip joint capsule and neighbouring iliopsoas tendon but also the anterior sacroiliac ligaments ( Atkins et al 2010).
The FABER test was evaluated in a study examining the correlation between clinical examination, imaging investigations and arthroscopy in a prospective study of 25 patients with hip pain. A range of hip joint pathologies was found including labral lesions, chondromalacia, loose bodies, synovitis and acetabular rim lesions. Of the 17 patients who recorded a positive FABER test pre-operatively, 15 were found to have hip pathology, although there was no correlation between a positive test and a specific lesion, rendering the test 88% sensitive. In contrast, magnetic resonance arthrography was 100% specific in 13 patients but lower levels of sensitivity were reported because of failure in some cases to identify pathology later verified by arthroscopy. The findings on clinical examination, including positive FABER (see p. 160) and FAIR tests (see p. 152), should alert the clinician to the possibility of hip pathology (particularly involving the labrum) and provide the basis for further investigations ( Mitchell et al 2003). -
Clinical tip
Groin pain and limitation of movement without the addition of overpressure is more likely to highlight a hip lesion, whereas unilateral lumbar/buttock pain reproduced with overpressure may be more attributable to a SIJ problem ( Atkins et al 2010). In addition to the site of pain, the patient’s age, history and other clinical findings will also help in the differential diagnosis but this is not universally the case and the possibility of co-existent dysfunction in both the hip and SIJ may need to be considered.
EXPERT OPINION
| COMMENTS
| ---|---|
★★
| FABER test
Useful as a non-specific test for assessing hip pathology.

Torque test
-
Purpose
To test the capsular ligaments and passive stability of the hip joint. -
Technique
Patient position
Lying supine to one side of the treatment couch with the buttock just off the edge.
Clinician position and action
The clinician stands between the couch and the patient’s affected leg with the cephalic hand placed over the anterior aspect of the thigh. The caudal hand supports the lower limb at the ankle. With the knee extended, the hip is taken to end-range extension over the edge of the couch until the pelvis just starts to rotate anteriorly. The hip is then taken to end-range internal rotation using the ankle to supply the leverage while simultaneously applying a strong posterolateral pressure over the anterior aspect of the upper thigh for 20 seconds.
Positive test
Reproduction of the patient’s pain suggests hip instability.

Fig. 5.7 ● Torque test. -
Clinical context
Hip instability is much less commonly encountered than instability at the shoulder largely because of the congruence of the pelvic and femoral architecture, although if this stable arrangement is altered due to congenital dysplasia, hip arthroplasty or capsular laxity (occurring as a result of connective tissue disorders such as Ehlers–Danlos syndrome), instability may ensue.
Significant trauma with the hip in a flexed position (typically a car collision where the knee impacts with the dashboard) is most likely to cause posterior instability and usually does so in combination with a fracture or dislocation. With this history a diagnosis of instability should be considered ( Byrd 2005 ). However, more subtle degrees of anterior instability have recently been reported in patients following comparatively minor trauma such as a fall onto a flexed hip or a sudden movement into abduction or external rotation. Damage to the ligamentum teres has been hypothesized as a possible cause for this instability ( Bardakos & Villar 2009). Symptoms and clinical signs are very similar to those reported in FAI i.e. groin pain related to activity, possibly accompanied by clicking, locking or giving way, positive impingement tests on examination (see McCarthy test, p. 156; FABER test, p. 160; FAIR test, p. 152; active SLR test,
p. 165) and further radiological investigations are required to aid the
differential diagnosis process ( Bardakos & Villar 2009). -
Clinical tip
The torque test can be modified to stress individual components of the capsular ligaments more specifically ( Lee 2004) by taking the hip into extension and full external rotation and adding abduction to focus stress on the iliofemoral ligament and adduction to test the pubofemoral ligament with the femoral distraction added in an identical manner. The ischiofemoral ligament is tested by the FAIR test (see p. 152).
EXPERT OPINION
| COMMENTS
| ---|---|
★
| Torque test
Hip instability can also be assessed using the log roll test. The torque test is also helpful to assess for psoas tightness and pain.

Active straight leg raise (SLR) test
-
Aka
Stinchfield resisted hip flexion test Mens test -
Purpose
To test for intra-articular hip pain (e.g. OA, labral tear, femoroacetabular impingement), fracture, pain stemming from a hip pros-thesis and contractile lesions of the hip flexors. -
Technique
Patient position
Lying supine.
Clinician position
Standing on the affected side.
Action
Keeping the knee extended, the patient performs a straight leg raise (SLR) to approximately 20–30°. The clinician then steadily resists the SLR by applying pressure to the lower aspect of the anterior thigh.
Positive test
Reproduction of the patient’s hip pain, which is usually in the groin or anterior aspect of the thigh.

Fig. 5.8 ● Active straight leg raise (SLR). -
Clinical context
Active lifting of a straight leg approximately 15 cm from the bed while in the supine position generates a reaction force through the hip of 1.8 body weight and can be used to indicate intra-articular
hip pathology. Adding a resistance to the leg will increase the force and make the test more sensitive for hip joint pathology but potentially less specific ( Callaghan et al 2007) as this will increase the stress on adjacent structures, namely the hip flexors (rectus femoris, sartorius and iliopsoas), the lumbar spine and sacro-iliac joint.
EXPERT OPINION
| COMMENTS
| ---|---|
★★
| Active SLR test
Groin pain on this test suggests hip pathology, with reproduction of buttock and/or low
back pain more suggestive of a lumbar or SI problem. The Ling test (see below), is a useful variation to discriminate between hip and spinal pathology. -
Clinical tip
The active SLR is also used as a validated test to measure effective load transfer between the trunk and lower limbs ( Lee 2004). Rather than assessing for pain, the effort required by the patient to maintain good pelvic stabilization throughout the test is noted. Excessive effort, loss of global and local muscle stabilization or compensatory movement of the pelvis into flexion, extension, rotation or lateral flexion during the test, indicates poor muscle control around the pelvis and spine. -
Variations
The Ling test is an adaptation of the SLR test. Active SLR to approximately 20° is performed on the affected leg and the patient is asked about the effect on their pain. The clinician then supports the patients heel and resists active hip extension. Pain which diminishes with resisted extension incriminates the hip, whilst unchanged symptoms should cast suspicion towards the spine.
● B MUSCLE AND TENDON TESTS
Thomas’s test

Aka
Hugh Owen Thomas (HOT) test Thompson test
Rectus femoris contracture test
Purpose
To test for a fixed flexion deformity at the hip and assess muscle length of the rectus femoris, iliacus, tensor fascia lata (TFL) and the iliotibial band (ITB).
Technique
Patient position
Lying supine.
Clinician position
Firstly, the clinician checks that the patient is able to maintain their normal lumbar lordosis with the legs comfortably resting on the couch. In patients with soft tissue tightness or flexion contracture, the affected hip(s) will be held in a degree of flexion (this may also present as an increased lumbar lordosis). One hand is then placed under the patient’s lumbar spine in order to assess the degree of lumbar movement during the test.
Action
The patient flexes the unaffected hip and knee towards the chest until the lumbar spine is flattened as assessed by the clinician’s hand. The patient then grasps the knee with both hands and maintains the hip in this position. Attention is then turned to the affected leg where the position of the thigh in relation to the couch is determined.
Positive test
In a normal hip, the affected thigh is able to remain extended, resting on the couch. In the presence of soft tissue tightness or a fixed flexion deformity, the affected hip will be drawn into a degree of flexion bringing the thigh away from the couch. If the clinician attempts to

Fig. 5.9 ● Thomas’s test.
passively extend the hip by pushing the thigh in a downwards direction, the patient will report a stretching sensation over the anterior hip and thigh and an attempt to increase their lumbar lordosis will be noted. If the hip gravitates more towards abduction than flexion during the test (the J sign), shortening of the ITB is likely (
Magee
2008
,
Placzek & Boyce
2006).
Clinical context
A fixed flexion deformity may occur for several reasons. Soft tissue shortening in the hip flexors can occur as a consequence of spasticity, pain or a habitually flexed posture and bony changes secondary to osteoarthritis or fracture may cause a physical block to hip extension. The test may appear positive if there is a fixed lumbar lordosis or significant posterior pelvic tilt which can give the illusion of a fixed hip flexion deformity.
Clinical tip
To differentiate between soft tissue tightness and joint restriction:
1. passively explore the end of available joint range and assess the end-feel as this can help to detect minor but significant differences
2. when testing muscle length, palpation for tightness within the muscle may help to distinguish between muscle contracture and tightness in the joint itself. If the muscle being tested feels comparatively relaxed, the joint is more likely to be involved
3. muscle energy techniques (e.g. hold/relax) can be used at the end of available range, with increasing extension indicating tightness of the hip flexors.
EXPERT OPINION
|
COMMENTS
| ---|---|
★★★
|
Thomas’s test
Used on most patients to assess for a fixed flexion deformity.
Variations
The
modified Thomas’s test
(
Fig.
5.10
) allows more effective analysis of the length of individual muscles (
Lee
2004). The patient ‘perches’ on the edge of the treatment couch at one end. The clinician stands adjacent to the affected side. The patient then flexes the opposite knee and hip towards the chest and slowly rolls backward
onto the couch as the clinician supports the patient’s head. Once lying, the affected thigh is allowed to hang off the end of the couch. Gentle overpressure can be applied to the anterior thigh to further assess the range of available hip extension (see
Fig.
5.10). Rectus femoris length is measured by recording the angle of knee flexion with the hip in a neutral position (the normal angle of knee flexion in this position is around 80°). TFL/ITB length is assessed in the same position but considered tight if the hip drifts into some abduction as it is extended (see Ober’s test, p. 171). Further evaluation of the ITB length can be achieved by observing the extent of tibial rotation at the knee, as the test position will have the tendency to pull the tibia into external rotation and consequently limit passive internal rotation if the ITB is tight.
A contracture of the rectus femoris can also be detected with
Ely’s test. The patient lies prone and the knee is passively flexed to approximately 90°. If there is shortening or contracture of the muscle, the hip on the same side will endeavour to flex as flexion is added at the knee.
*

Fig. 5.10 ● Modified Thomas’s test assessing the range of hip extension.

Modified Ober’s test
-
Purpose
To assess ITB and tensor fascia lata (TFL) extensibility. -
Technique
Patient position
Lying on the unaffected side with the hip and knee flexed to provide a stable base. The affected hip is uppermost and in a neutral position.
Clinician position
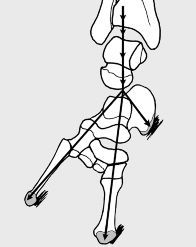
Standing behind the patient, the caudal hand crosses over the top of the uppermost leg and cups the medial aspect of the thigh just above the knee. The cephalic forearm stabilizes the pelvis by applying a firm downward and forward pressure onto the iliac crest. The affected hip is then drawn into an extended and abducted starting position ensuring that neutral femoral rotation is maintained.
Action
The pelvis must be prevented from tilting backwards by maintaining the downward and forwards pressure with the stabilizing arm. Maintaining the affected hip in extension the thigh is lowered towards an adducted position. The end-point of the test is either cessation of hip adduction as the leg reaches a resting position on the couch or the clinician detecting movement of the pelvis.
Positive test
A positive test is either reproduction of the patient’s lateral hip pain or reduced range of movement. The normal range of hip adduction

Fig. 5.11 ● Modified Ober’s test.
in the modified Ober’s test position is 10° beyond neutral and an inability to reach this range is therefore considered abnormal. -
Clinical context
The effects on the ITB of both the modified and original Ober’s tests (see below) have been evaluated using ultrasound imaging in healthy subjects. Both tests were shown to cause a reduction of the ITB width as the adduction stretch was gradually increased until a neutral adduction angle was reached. Beyond the neutral position, only the modified Ober’s test resulted in a further reduction in the ITB width (Wang et al 2006). Because the modified Ober’s test allows a greater range of adduction to be achieved and more effectively tensions the ITB, it is the preferred test for many clinicians ( Gajdosik et al 2003 , Reese & Bandy 2003). -
Clinical tip
To make sure that the ITB passes over the greater trochanter during the test, the clinician must ensure that the hip stays in the extended position throughout the manoeuvre.
EXPERT OPINION
| COMMENTS
| ---|---|
★★
| Modified Ober’s test
Useful in assessing lateral hip pain. If positive, along with tenderness over the greater trochanter, a diagnosis of trochanteric bursitis/ tendinopathy is likely. -
Variations
The original Ober’s test ( Fig. 5.12 ; Ober 1936 ) was described for use with patients suffering from low back pain and sciatica. The position of both clinician and patient is as described above. The affected knee is then flexed to 90° and the hip lowered into the adducted position. A reduced range (normal range 0° adduction) is anticipated when compared with the modified Ober’s test (see Fig 5.11). It has been suggested that the original test selectively stresses the TFL more than the ITB, while the modified version reverses this tendency. Ober’s test can also be limited by contracture of the rectus femoris muscle and this can be evaluated further with Thomas’s test (see p. 166). The position of hip extension and knee flexion adopted in the modified Ober’s test also tensions the femoral nerve and provocation of back pain or thigh pain/paraesthesiae during the test would guide the clinician to investigate the lumbar spine and neural tissue.

Fig. 5.12 ● Original Ober’s test.

Trendelenburg test
-
Purpose
To test for stability of the pelvic/hip complex and strength of the hip abductors. -
Technique
Patient position
Standing.
Clinician position
Standing facing the patient in order to observe the outcome of the test and provide some support to the patient with the hands if required.
Action
The patient is asked to transfer their weight onto the affected leg and lift the unaffected foot off the ground by flexing both the hip and knee. The clinician observes the movement as the weight is transferred onto the symptomatic side.
Positive test
A positive/abnormal test is recorded if the pelvis on the non-weight-bearing side drops because the gluteal muscles on the weight-bearing side cannot maintain the pelvis in a neutral position. Normally the glutei will produce a slight uplift of the pelvis on the non-weight-bearing side as weight is borne on the opposite leg. In a study of normal volunteers the change in position of the pelvis on the femur was measured at a barely detectable 4° and, that being the case, normal abductor performance could be assumed ( Youdas et al 2007).

Fig. 5.13 ● Trendelenburg test on a normal subject where the pelvis position is maintained as weight is borne through the supporting leg. -
Clinical context
There are several variations of the original test described by Trendelenburg in 1897 ( Hardcastle & Nade 1985 ). In an attempt to standardize the method and interpretation of the Trendelenburg test, normal subjects were compared to a group of symptomatic subjects with disorders of the hip or spine. Several factors were identified which commonly led to incorrect interpretation of the test, namely faulty technique because of poor understanding, use of the trunk muscles rather than the glutei to elevate the pelvis, shift of the trunk and body weight over the weight-bearing leg and using pain rather than weakness to distinguish a positive test ( Hardcastle & Nade 1985). This study led to a modified version (see Variations).
A positive test is not diagnostic of a specific pathology and, as with most tests, needs to be evaluated in the light of other presenting signs and symptoms. It has, however, been shown to be a useful predictor of gluteal tendon pathology or weakness in patients with lateral hip pain. In a sample of 24 female patients with lateral hip pain, the presence of both a positive Trendelenburg test and an accompanying Trendelenburg gait was found to be a better predictor of a gluteus medius tear than
pain found on either resisted hip abduction or internal rotation and served as a reasonable determinant for MRI referral ( Bird et al 2001).
In another small study where MRI was used as the reference standard to diagnose gluteal tendinopathy, patients were asked to adopt a modified Trendelenburg test position for 30 seconds. Provocation of pain (rather than weakness) in this position was found to be very sensitive and specific in detecting the presence of gluteal tendinopathy and/or bursitis ( Lequesne et al 2008).
TABLE 5.3 TRENDELENBURG TEST
Author and year
| LR +
| LR —
| Target condition
Bird et al 2001
| 3.2
| 0.35
| Gluteal tendon tear (weakness)
Lequesne et al 2008
| 37
| 0
| Gluteal tendinopathy +/—
bursitis (pain) -
Clinical tip
A trick movement (side-flexion towards the weight-bearing side) may be performed by the patient with gluteal weakness who is unable to achieve a normal response to Trendelenburg testing.
EXPERT OPINION
| COMMENTS
| ---|---|
★★★
| Trendelenburg test
Used with most patients. Most accurate if one-legged stance is maintained for 30 seconds. -
Variations
The Hardcastle and Nade method ( Hardcastle & Nade 1985) has the clinician standing behind the patient. If some support is required to allow the patient to balance, this should be provided on the weight-bearing side. The patient is asked to stand on the affected leg and lift the other foot off the floor. They then attempt to raise the pelvis on the unaffected side while the clinician observes the movement and transference of weight. A negative test (i.e. normal response) is found if the pelvis on the non-weight-bearing side can be raised and held for 30 seconds while the patient maintains a
straight, neutral position with the head aligned over the supporting hip and foot ( Fig. 5.14A ). A positive test (i.e. abnormal) is indicated by either the pelvis on the non-weight-bearing side dropping or an inability to raise the pelvis and maintain this position for 30 seconds, the so called ‘delayed Trendelenburg response’ ( Fig. 5.14B).
A
B




Fig. 5.14 ● Hardcastle and Nade method. A normal subject maintaining a raised position of the pelvis on the non-weight-bearing leg (A). A positive test is indicated if the patient is unable to achieve or maintain the raised position (B).

● C OTHER TESTS
Craig’s test
-
Aka
Ryder method for measuring femoral anteversion -
Purpose
To ascertain the degree of femoral anteversion. -
Technique
Patient position
Lying prone with the thighs and knees approximated and the affected knee flexed to 90°.
Clinician position and action
Using one hand, the lateral aspect of the greater trochanter on the affected side is palpated. The other hand uses the patient’s foot as a lever and passively internally rotates the hip until the greater trochanter reaches its most prominent point laterally. The angle that the line of the tibia makes with the vertical equates to the degree of femoral anteversion.
Positive test
The normal angle of femoral anteversion in the adult is between 8° and 15°. An angle greater than 15° indicates increased femoral anteversion; less than 8° indicates femoral retroversion.
8−15°

Fig. 5.15 ● The normal degree of femoral anteversion (8–15°) is indicated by the angle formed between the vertical axis and the line of the tibia. -
Clinical context
The femoral neck normally projects anteriorly from the shaft of the femur. This degree of anteversion (which simply means ‘leaning for-ward’) is measured by the angle formed between the axis of the neck of femur and an imaginary line through the femoral condyles at the knee. It is suggested that the degree of femoral and acetabular rotation is determined by intrauterine foetal position during pregnancy.
In 85% of cases the acetabular and femoral positions normalize after birth and the degree of anteversion gradually decreases from 30–40° in childhood to approximately 15° with skeletal maturity. There is also a gender variation, with an average angle of 14° in women compared to 7° in men ( Magee 2008).
An increased angle of anteversion is accompanied by excessive internal rotation (60° is abnormal) and reduced external rotation of the hip, a presentation often epitomized by bilateral ‘squint-ing’ patellae. Osteoarthritis of the knee or patellofemoral instability are both secondary problems that can also develop as a result. Decreased femoral anteversion can be found as a result of a slipped upper femoral epiphysis, coxa vara, a deep acetabulum or congenital dysplasia and there is increasing evidence to suggest that this retroversion also predisposes to hip ostearthritis (Giori & Trousdale 2003 , Kim et al 2006 , Tonnis & Heinecke 1999) and femoro-acetabu-lar impingement (Giori & Trousdale 2003).
EXPERT OPINION
| COMMENTS
| ---|---|
★★
| Craig’s test
An easily performed test to assess anteversion in children and adults.

Sign of the buttock
-
Purpose
To test for a serious lesion in the buttock or hip region, e.g. fracture, neoplasm or infection. -
Technique
Patient position
Lying supine.
Clinician position and action
Standing adjacent to the side being tested the clinician performs a straight leg raise (SLR) on the affected leg and the angle achieved is noted (see Fig. 5.16A ). At the point where increased pain is reported by the patient, the tension in the posterior thigh, buttock and sci-atic nerve is removed by flexing the knee while maintaining the hip at the same angle (see Fig. 5.16B). Further hip flexion is then
attempted. Under normal circumstances, it should then be possible to move the hip into further flexion.
Positive test
Once the knee is flexed, further hip flexion would be expected but in fact none is possible as this increases the patient’s buttock pain. This may be accompanied by voluntary muscle spasm and the patient stopping further movement taking place ( Atkins et al 2010).
A
B




Fig. 5.16 ● In a positive sign of the buttock, the degree of hip flexion achievable with a straight leg raise (A), remains unchanged when the knee is flexed (B). -
Clinical context
The sign of the buttock is an unusual finding and, if genuinely detected, indicates the presence of a serious injury or disease process such as fracture or neoplasm around the upper femur and pelvis, osteomyelitis, septic arthritis of the hip, ischiorectal abscess or septic bursitis.
In addition to the sign of the buttock, lumbar flexion will also be limited and reproduce the patient’s buttock pain. The degree of flexion achieved will be equal to the angle of flexion permitted with SLR and hip flexion testing. This is an important detail as there are many pathologies that can present simultaneously causing different degrees of limitation and pain but none that produce an identical loss of flexion ( Atkins et al 2010). Pain on a number of resisted tests around the hip may also be evident as well as a subjective history of ‘red flags’ such as unremitting pain, fever, weight loss or significant night pain. -
Clinical tip
The patient will register some apprehension to the examination, particularly in relation to the key elements of this test, and will instinctively withdraw from the movement, often before the pain is elicited. The anticipation of severe pain causes them to stop the movement either with their hand or verbally, at which point the examiner may
detect an ‘empty’ end-feel – characterized by a sense that more range is obtainable but unavailable due to the patient being unwilling to allow further excursion. The movement may also be limited by a combination of voluntary and involuntary muscle spasm which would further prevent movement if attempted.

Scientific References
-
Atkins, E., Kerr, E., Goodlad, J., 2010. A Practical Approach to Orthopaedic Medicine, third ed. Churchill Livingstone, Edinburgh.
Austin, A., Souza, R., Meyer, J., et al., 2008. Identification of abnormal hip motion associated with acetabular labral pathology. J. Orthop. Sport. Phys. Ther. 38 (9), 558–565.
Bardakos, N.V., Villar, R.N., 2009. The ligamentum teres of the adult hip. J. Bone Joint Surg. Br. 91 (1), 8–15.
Benson, E.R., Schutzer, S.F., 1999. Posttraumatic piriformis syndrome: diagnosis and results of operative treatment. J. Bone Joint Surg. 81 (7), 941–949.
Bird, P.A., Oakley, S.P., Shnier, R., et al., 2001. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum. 44 (9), 2138–2145.
Burnett, R.S., Della Rocca, G., Prather, H., et al., 2006. Clinical presentation of patients with tears of the acetabular labrum. J. Bone Joint Surg. Am. 88, 1448–1457.
Byrd, J.W., 2005. Hip arthroscopy in athletes. Oper. Techn. Sport. Med. 13, 24–36. Callaghan, J., Rosenberg, A., Rubash, H., 2007. The Adult Hip, second ed.
Lippincott Williams and Wilkins, Philadelphia.
DeAngelis, N.A., Busconi, B.D., 2003. Assessment and differential diagnosis of the painful hip. Clin. Orthop. Relat. Res. 406, 11–18.
Fishman, L.M., Dombi, G.W., Michaelsen, C., et al., 2002. Piriformis syndrome: diagnosis, treatment, and outcome – a 10-year study. Arch. Phys. Med. Rehab. 83 (3), 295–301.
Fitzgerald, R.H., 1995. Acetabular labrum tears diagnosis and treatment. Clin.
Orthop. Relat. Res. 311, 60–68.
Gajdosik, R.L., Sandler, M.M., Marr, H.L., 2003. Influence of knee positions and gender on the Ober test for length of the iliotibial band. Clin. Biomech. 18 (1), 77–79.
Giori, N.J., Trousdale, R.T., 2003. Acetabular retroversion is associated with osteoarthritis of the hip. Clin. Orthop. Relat. Res. 417, 263–269.
Hardcastle, P., Nade, S., 1985. The significance of the Trendelenburg test. J. Bone Joint Surg. Br. 67 (5), 741–745.
Hase, T., Ueo, T., 1999. Acetabular labral tear: arthroscopic diagnosis and treatment.
Arthroscopy: J. Arthroscopic Relat. Surg. 15 (2), 138–141.
Ito, K., Leunig, M., Ganz, R., 2004. Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin. Orthop. Relat. Res. 429 (12), 262–271.
Jaberi, F., Parvizi, J., 2007. Hip pain in young adults femoroacetabular impingement. J. Arthroplasty 22 (7/Suppl. 3), 37–42.
Kim, W.Y., Hutchinson, C.E., Andrew, J.G., 2006. The relationship between acetabular retroversion and osteoarthritis of the hip. J. Bone Joint Surg. Br. 88 (6), 727–729.
Lee, D., 2004. The Pelvic Girdle: An Approach to the Examination and Treatment of the Lumbopelvic-hip Region, third ed. Churchill Livingstone, Edinburgh.
Lequesne, M., Mathieu, P., Vuillemin-Bodaghi, V., et al., 2008. Gluteal tendinopathy in refractory greater trochanter pain syndrome: diagnostic value of two clinical tests. Arthritis Rheum. 59 (2), 241–246.
Lewis, C.L., Sahrmann, S.A., 2006. Acetabular labral tears. Phys. Ther. 86 (1), 110–121.
McCarthy, J.C., Busconi, B., 1995. The role of hip arthroscopy in the diagnosis and treatment of hip disease. Can. J. Surg. 38 (1), 13–17.
McCarthy, J., Noble, P., Aluisio, F.V., et al., 2003. Anatomy, pathologic features, and treatment of acetabular labral tears. Clin. Orthop. Relat. Res. 406, 38–47.
Magee, D.J., 2008. Orthopaedic Physical Assessment, fifth ed. Saunders, Philadelphia.
Mitchell, B., McCrory, P., Brukner, P., et al., 2003. Hip joint pathology: clinical presentation and correlation between magnetic resonance arthrography, ultrasound and arthroscopic findings in 25 consecutive cases. Clin. J. Sport Med. 13 (3), 152–156.
Narvani, A.A., Tsiridis, E., Kendall, S., et al., 2003. A preliminary report on prevalence of acetabular labrum tears in sports patients with groin pain. Knee Surg. Sports Traumatol. Arthrosc. 11 (6), 403–408.
Ober, F., 1936. The role of the iliotibial band and fascia lata as a factor in the causation of low back disabilities and sciatica. J. Bone Joint Surg. Am. 18, 105–110.
Placzek, J.D., Boyce, D.A., 2006. Orthopaedic Physical Therapy Secrets, second ed. Elsevier Health Sciences, Missouri.
Reese, N., Bandy, W., 2003. Use of an inclinometer to measure flexibility of the iliotibial band using the Ober test and the modified Ober test: differences in magnitude and reliability of measurements. J. Orthop. Sports Phys. Ther. 33 (6), 326–330.
Standaert, C.J., Manner, P.A., Herring, S.A., 2008. Expert opinion and controversies in musculoskeletal and sports medicine: femoroacetabular impingement. Arch. Phys. Med. Rehabil. 89, 890–893.
Tonnis, D., Heinecke, A., 1999. Acetabular and femoral anteversion: relationship with osteoarthritis of the hip. J. Bone Joint Surg. Am. 81 (12), 1747–1770.
Wang, T.G., Jan, M.H., Lin, K.H., et al., 2006. Assessment of stretching of the iliotibial tract with Ober and modified Ober’s tests: an ultrasonographic study. Arch. Phys. Med. Rehabil. 87 (10), 1407–1411.
Woods, D., Macnicol, M., 2001. The flexion–adduction test: an early sign of hip disease. J. Pediatr. Orthop. 10 (3), 180–185.
Youdas, J.W., Mraz, S.T., Norstad, B.J., et al., 2007. Determining meaningful changes in pelvic-on-femoral position during the Trendelenburg test. J. Sport Rehabil. 16 (4), 326–335.
You Might Also Like