Posterolateral Surgical Approaches: Achieve Optimal Hip Replacement

Key Takeaway
Your ultimate guide to Posterolateral Surgical Approaches: Achieve Optimal Hip Replacement starts here. Surgical approaches posterolateral for total hip arthroplasty provide complete exposure of the proximal femur and acetabulum. This technique, typically with the patient in a lateral decubitus position, aims to reduce tissue trauma, enhance posterior soft tissue repair, and facilitate multimodal pain management, crucial for proper component positioning during hip replacement surgery.
Introduction and Epidemiology
Total hip arthroplasty represents one of the most successful and cost-effective surgical interventions in modern medicine, providing profound pain relief and functional restoration for patients with end-stage hip pathology. Historically, Charnley popularized the transtrochanteric approach for his low-friction arthroplasty, which provided excellent exposure but was fraught with complications related to trochanteric nonunion and hardware failure. Consequently, the orthopedic community evolved toward alternative exposures, including the anterior (Smith-Petersen), direct lateral (Hardinge), anterolateral (Watson-Jones), and posterior (Gibson and Moore) approaches.
The posterolateral approach remains the most frequently utilized surgical exposure for primary and revision total hip arthroplasty globally. Its enduring popularity is attributed to its extensile nature, excellent visualization of both the femoral and acetabular anatomy, and preservation of the hip abductor mechanism. Unlike the direct lateral approach, which violates the gluteus medius and minimus and can lead to postoperative Trendelenburg gait, the posterolateral approach relies on a muscle-splitting technique through the gluteus maximus and tenotomy of the short external rotators.

The current trend in adult reconstruction emphasizes tissue-sparing techniques and rapid rehabilitation. While the direct anterior approach has gained traction for its internervous plane, the posterolateral approach has been simultaneously refined. Modern iterations utilize smaller incisions, meticulous hemostasis, and, critically, an enhanced posterior soft tissue repair. This meticulous repair of the capsule and short external rotators has drastically reduced the historical Achilles heel of the posterior approach—postoperative dislocation—bringing dislocation rates to parity with anterior and lateral approaches.

Epidemiologically, the demand for total hip arthroplasty is projected to grow exponentially due to an aging population and expanding indications in younger, highly active patients. Osteoarthritis remains the primary diagnosis driving surgical volume, followed by avascular necrosis, inflammatory arthropathies, and post-traumatic arthritis. Mastery of the posterolateral approach is therefore an essential competency for any orthopedic surgeon, providing a reliable, extensile, and safe pathway to the hip joint for both straightforward primary cases and complex reconstructive challenges.
Surgical Anatomy and Biomechanics
A profound understanding of the topographical and deep anatomy of the hip is paramount for executing a safe and efficient posterolateral approach. The hip is a highly constrained ball-and-socket joint, stabilized by a robust capsuloligamentous complex and a dynamic muscular envelope.

The posterolateral approach does not utilize a true internervous plane. The superficial dissection involves splitting the fibers of the gluteus maximus, which is entirely innervated by the inferior gluteal nerve. Because the muscle fibers are separated longitudinally rather than transected, denervation is avoided provided the split does not extend excessively medial into the main trunk of the nerve.

Deep to the gluteus maximus lies the abductor complex superiorly and the short external rotators posteriorly. The short external rotators, from superior to inferior, include the piriformis, superior gemellus, obturator internus, inferior gemellus, obturator externus, and quadratus femoris. These structures serve as the primary dynamic posterior stabilizers of the hip. The piriformis and the conjoined tendon of the gemelli and obturator internus insert on the medial aspect of the greater trochanter and must be released to access the posterior capsule.
Neurovascular proximity is a critical consideration. The sciatic nerve exits the greater sciatic foramen typically inferior to the piriformis muscle. However, anatomical variants exist wherein the nerve or its peroneal division pierces or exits superior to the piriformis. The nerve lies embedded in fat superficial to the short external rotators and posterior to the quadratus femoris. The medial circumflex femoral artery is the primary blood supply to the femoral head; its terminal branches traverse deep to the quadratus femoris. When releasing the quadratus femoris, the surgeon must remain meticulous to avoid severing this vessel, which can result in profound hemorrhage.

Biomechanically, the goal of total hip arthroplasty is to restore the native center of rotation, femoral offset, and leg length. The posterolateral approach provides direct visualization of the posterior acetabular wall and the transverse acetabular ligament, which are critical landmarks for establishing appropriate acetabular component version and inclination.
Indications and Contraindications
The indications for total hip arthroplasty via a posterolateral approach encompass a wide spectrum of degenerative, inflammatory, and traumatic conditions of the hip joint. The approach is particularly advantageous in cases requiring extensive femoral exposure, such as complex primary arthroplasty with proximal femoral deformity, retained hardware removal, or revision arthroplasty.

Contraindications are generally related to systemic instability, active infection, or specific local anatomical constraints. While the posterior approach has historically been relatively contraindicated in patients with severe neuromuscular disorders or cognitive impairment due to the perceived higher risk of posterior dislocation, the advent of dual-mobility articulations and enhanced capsular repair techniques has largely mitigated this concern.

| Category | Operative Indications | Non-Operative Indications or Contraindications |
|---|---|---|
| Degenerative | End-stage primary osteoarthritis with failed conservative management | Mild to moderate osteoarthritis responsive to NSAIDs and physical therapy |
| Traumatic | Displaced femoral neck fractures in elderly patients; post-traumatic arthritis | Undisplaced or valgus-impacted femoral neck fractures amenable to in-situ fixation |
| Avascular | Ficat Stage III/IV avascular necrosis with subchondral collapse | Ficat Stage I/II avascular necrosis (core decompression or conservative care) |
| Infectious | Sequelae of childhood septic arthritis (healed) | Active periprosthetic joint infection or systemic sepsis (Absolute Contraindication) |
| Neuromuscular | Degenerative joint disease in controlled Parkinson disease (with dual mobility) | Uncontrolled spasticity or severe cognitive decline precluding rehab adherence |
| Systemic | Inflammatory arthropathies (Rheumatoid, Ankylosing Spondylitis) | Severe medical comorbidities (ASA IV/V) making anesthesia prohibitive |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the foundation of a successful total hip arthroplasty. Clinical evaluation must assess leg length discrepancy (both apparent and true), abductor strength, spinal mobility, and the presence of any fixed pelvic obliquity. These factors directly influence the intraoperative goals for offset and limb length restoration.
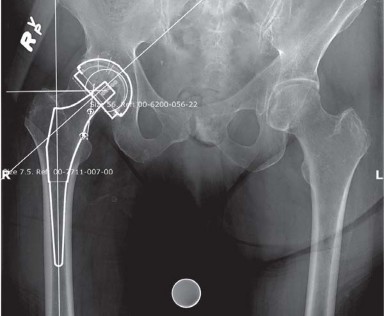
Radiographic templating is performed on standardized weight-bearing anteroposterior pelvic radiographs and lateral views of the affected hip. Digital templating software allows the surgeon to estimate the optimal center of rotation, determine the required acetabular component size, and plan the femoral neck osteotomy level. The templating process also aids in selecting the appropriate femoral stem size, offset, and neck length to restore the native biomechanics.

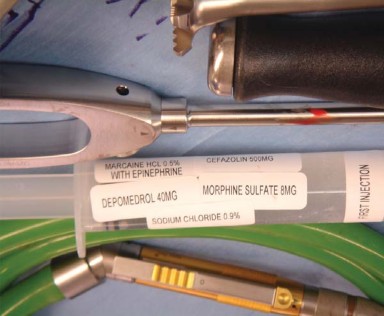
Anesthetic management typically involves regional techniques, such as spinal or epidural anesthesia. Regional anesthesia is preferred as it provides excellent muscle relaxation, decreases intraoperative blood loss through controlled hypotension, and reduces the risk of deep vein thrombosis compared to general anesthesia. Preoperative optimization includes the administration of prophylactic intravenous antibiotics within one hour of incision and the initiation of appropriate multimodal analgesia and tranexamic acid protocols.
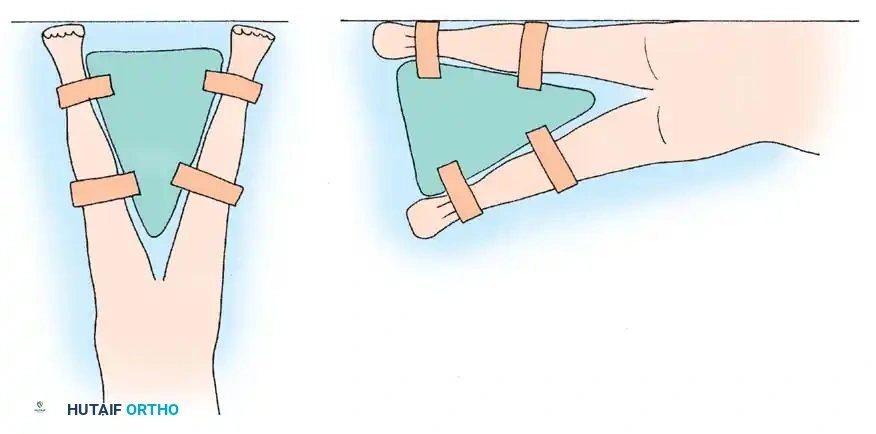
Patient positioning for the posterolateral approach requires the lateral decubitus position. The patient is placed on a standard or custom-designed fracture table, with the operative hip facing superiorly. Rigid pelvic fixation is mandatory to ensure accurate intraoperative assessment of component position.

The pelvis is stabilized using padded anterior and posterior supports. The anterior post is positioned at the level of the pubic symphysis, while the posterior post is placed against the sacrum. It is critical that the pelvis is perfectly perpendicular to the floor; any unappreciated pelvic roll will translate directly into malposition of the acetabular component (e.g., retroversion if the pelvis is rolled forward).

All bony prominences, including the dependent axilla, fibular head, and greater trochanter of the non-operative leg, must be meticulously padded to prevent neuropraxia and pressure necrosis. The operative leg is draped free to allow for full range of motion during the procedure, which is essential for dislocation, trialing, and stability testing.



Detailed Surgical Approach and Technique
Incision and Superficial Dissection
The surgical incision is centered over the posterior aspect of the greater trochanter. The landmark for the proximal extent of the incision is approximately midway between the posterior superior iliac spine and the tip of the greater trochanter. The incision extends distally over the lateral aspect of the femoral shaft.
Following skin incision, the subcutaneous tissues are divided in line with the wound to expose the fascia lata distally and the gluteus maximus fascia proximally. The fascia lata is incised longitudinally over the center of the greater trochanter. Proximally, this fascial incision is extended in line with the fibers of the gluteus maximus. Blunt dissection is used to split the gluteus maximus fibers, minimizing bleeding by coagulating bridging vessels. A Charnley or similar self-retaining retractor is placed to maintain the superficial exposure.
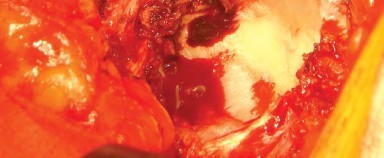
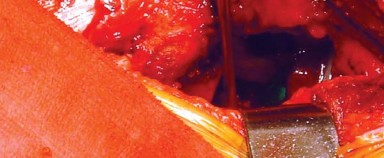
Deep Dissection and Capsular Exposure
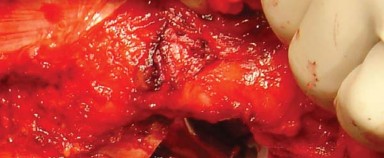
Deep to the gluteus maximus, the trochanteric bursa is excised to expose the short external rotators. The leg is internally rotated to place the short external rotators on stretch. The piriformis tendon and the conjoined tendon of the obturator internus and gemelli are identified.

These tendons are tagged with heavy non-absorbable suture and transected close to their insertion on the greater trochanter. The quadratus femoris is partially or fully released depending on the necessary exposure, taking great care to identify and coagulate the terminal branches of the medial circumflex femoral artery located at the inferior border of the muscle. The short external rotators are reflected posteriorly, which serves to protect the sciatic nerve during the remainder of the procedure.

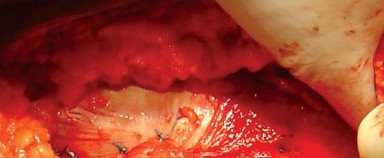
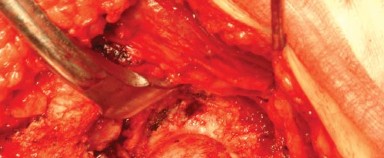
The posterior capsule of the hip joint is now visible. A capsulotomy is performed, typically in an I-shaped, T-shaped, or inverted T-shaped fashion. The capsular flaps are tagged for later repair.
Hip Dislocation and Femoral Neck Osteotomy
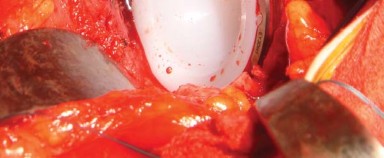
With the capsule open, the hip is dislocated using a maneuver of flexion, adduction, and progressive internal rotation. A bone hook may be utilized to assist with dislocation, particularly in stiff hips. Once dislocated, the femoral neck is exposed.
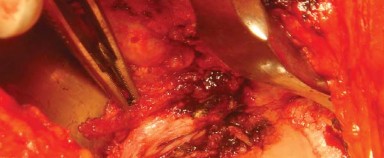
The femoral neck osteotomy is performed according to the preoperative template. The level and angle of the cut are referenced from the lesser trochanter and the saddle of the greater trochanter. An oscillating saw is used to complete the osteotomy, and the femoral head is removed and passed off the field.

Acetabular Preparation and Component Implantation
Optimal exposure of the acetabulum requires precise retractor placement. Typically, a blunt retractor is placed anteriorly over the anterior rim of the acetabulum, a second retractor is placed inferiorly beneath the transverse acetabular ligament, and a posterior retractor is placed to retract the femur anteriorly. The labrum and osteophytes are excised to define the true bony rim of the acetabulum.
Sequential reaming is performed, starting with a small reamer directed medially to establish the true medial wall (cotyloid fossa), followed by progressively larger reamers directed in the intended position of the final component (typically 40-45 degrees of abduction and 15-20 degrees of anteversion).

Once bleeding subchondral bone is achieved and a hemispherical bed is prepared, the definitive acetabular shell is impacted into place. Adjunctive screw fixation may be utilized if initial press-fit stability is suboptimal. The appropriate polyethylene liner is then impacted into the shell.

Femoral Preparation and Trialing
Attention is then turned to the femur. The operative leg is placed in a position of flexion, adduction, and marked internal rotation. The proximal femur is elevated using a retractor placed under the proximal femoral metaphysis.

A box osteotome is used to open the femoral canal, taking care to lateralize into the greater trochanter to avoid varus malalignment of the stem. Sequential broaching is performed to shape the cancellous bone of the proximal femur to match the geometry of the selected implant.

Once axial and rotational stability are achieved with the final broach, a trial neck and head are placed. The hip is reduced, and a comprehensive assessment of stability, leg length, and offset is conducted.

Stability is tested in flexion, adduction, and internal rotation (simulating the position of posterior dislocation) as well as extension and external rotation (simulating anterior dislocation). Leg length is assessed by comparing the relationship of the medial malleoli or utilizing intraoperative referencing pins.
Definitive Implantation and Enhanced Posterior Repair
Following satisfactory trialing, the hip is redislocated, and the trial components are removed. The definitive femoral stem is impacted into the canal, and the final modular head is seated onto the trunnion after ensuring the taper is clean and dry. The hip is reduced for the final time.




You Might Also Like