Minimally Invasive THA: Navigating Techniques, Benefits & Pitfalls

Key Takeaway
This article provides essential research regarding Minimally Invasive THA: Navigating Techniques, Benefits & Pitfalls. Minimally invasive THA refers to less invasive surgical approaches for total hip arthroplasty, aiming for optimum visualization with reduced invasiveness. These techniques typically use smaller incisions, often 10-12 cm or less. Two main categories exist: modified single-incision and two-incision approaches. Proper patient selection is crucial due to potential challenges and ongoing studies regarding long-term outcomes.
Introduction ## P ITFALLS
1.
Some contraindications that can assist with patient selection generally include complicated primary THA, revision surgery, severe hip dysplasia (Crowe grade III or IV), body mass index considerably higher than 30 kg/ m
2
, very muscular patients, osteoporotic bone, and very stiff joints (Vail, 2005).
1.
Total hip arthroplasty (THA) has developed into one of the most frequently performed and successful procedures in orthopedic surgery. Although there have been numerous variations in implant design and biomaterials over the years, surgical approaches to the hip have remained relatively unchanged. Recently, with the development of minimally invasive techniques within other areas of surgery, orthopedic surgeons have revealed increased interest in less invasive approaches for THA, which balances the desire for optimum visualization with less invasive surgery.
2.
Two categories of minimally invasive THA have materialized: several modified single-incision approaches and a two-incision approach. Controversies
1.
The definition of minimally invasive is controversial, but the “mini-incision” used for these techniques is typically a length of 10 cm or less, with some using up to 12 cm (Vail, 2005). As with any surgery, the incision length should not be standardized, as several factors can alter the exposure needed to correctly perform the THA. The length of the incision(s) depends on the skill of the surgeon, patient weight, local subcutaneous tissue, muscle mass, and the individual joint and anatomy.
2.
THA utilizing minimally invasive surgical technique is a topic that has created much debate and attention from surgeons and patients alike. It is important to realize that longterm outcomes are still unknown, and the short-term outcomes have failed to reveal consistent results regarding its intended benefits.
1.
The single-incision techniques are alterations to the standard posterior, anterolateral, and direct anterior approaches. These can be developed on a graduated basis with progressive reduction of incision length at a rate comfortable for the surgeon. Similarly, the mini single-incision approaches allow extension into a standard incision if needed to gain additional exposure.
2.
The two-incision technique represents a drastically different approach for THA and utilizes separate incisions to insert the acetabular and femoral components.
3.
One key objective of any THA is to have well-positioned components without compromising soft tissues or neurovascular structures, allowing the patient to have a quick and functional recovery. To achieve this, it is crucial to gain sufficient access to both the acetabulum and proximal femur. Indications
4.
When considering minimally invasive THA, proper patient selection is important to avoid difficulties with exposure that ultimately may compromise the safety of the procedure.
5.
Another important consideration is surgeon inexperience and/or lack of training. Each case needs to be looked at individually, with both the surgeon and the patient examining the risks and benefits to determine if minimally invasive techniques are worth pursuing. 115
### Minimally Invasive THA
SINGLE-INCISION POSTERIOR APPROACH Positioning
1.
The patient is positioned in the lateral decubitus position. ## P EARLS
1.
Regardless of how this flap is created, it may be beneficial to tag it with sutures to help with anatomic repair at the end of the procedure.
Portals/Exposures
2.
The incision is a short, oblique incision centered over the acetabulum, or utilizing the middle third of what would be the standard incision for the posterior approach over the posterior greater trochanter (Fig. 1). The oblique nature of the incision can aid in acetabular reaming, as the incision is in that same direction.
3.
The dissection proceeds to the thin investing fascia of the gluteus maximus muscle and the tensor fascia lata.
4.
The gluteus maximus is split in line with its fibers, while trying to avoid cutting the iliotibial band. Trochanter (outline) Incision mini-posterior approach
---
FIGURE 1 ### Minimally Invasive THA
5. A Charnley retractor can be placed deep to the gluteus maximus to assist with exposure and identification of the trochanteric bursa, the posterior border of the gluteus medius (forceps in Fig. 2), the piriformis, and the short external rotators.
 ---
---
 116 A Gluteus medius Trochanter Femur Forceps Piriformis and short external rotators B
116 A Gluteus medius Trochanter Femur Forceps Piriformis and short external rotators B
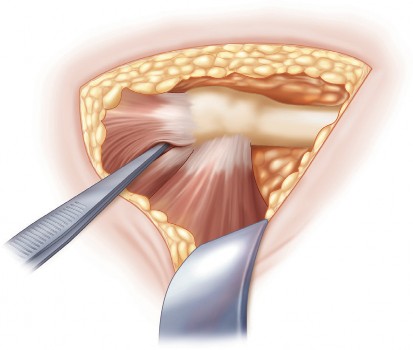 ---
FIGURE 2 117 ### Minimally Invasive THA
1. At this point, it is also crucial to palpate and protect the sciatic nerve as it leaves the greater sciatic notch and continues distally over the ischial tuberosity, although it is not necessary to expose the nerve.
2.
With a retractor pulling the gluteus medius anteriorly, the short external rotators, consisting of the piriformis and the conjoined tendon (superior gemellus, obturator internus, inferior gemellus, and quadratus femoris), should be incised from the femur and reflected posteriorly. A capsulotomy can now be performed exposing the femoral head and allowing posterior dislocation of the hip. Alternatively, the capsule and external rotators can be incised and reflected as a single layer. Instrumentation/ Implantation
1.
Angled reamers can be utilized to help avoid impingement on soft tissues. Procedure ## Step 1
3. The femoral neck is cut with an oscillating saw, the femoral head removed, and attention turned to preparation of the acetabulum.
4.
Ideally, an acetabular retractor with a sharp tip and a light to illuminate the acetabulum should be placed on the anterior rim.
5.
The inferior capsule may need to be divided, and the final step to gain maximum acetabular exposure is flexion and adduction of the femur.
6.
Before reaming, the labrum should be excised and any visible osteophytes removed. The acetabulum is then sequentially reamed under direct vision, making certain the femur does not force the reamer into the posterior column.
7.
Once reaming of the acetabulum is complete, the implant is inserted. ### Minimally Invasive THA
---
FIGURE 2 117 ### Minimally Invasive THA
1. At this point, it is also crucial to palpate and protect the sciatic nerve as it leaves the greater sciatic notch and continues distally over the ischial tuberosity, although it is not necessary to expose the nerve.
2.
With a retractor pulling the gluteus medius anteriorly, the short external rotators, consisting of the piriformis and the conjoined tendon (superior gemellus, obturator internus, inferior gemellus, and quadratus femoris), should be incised from the femur and reflected posteriorly. A capsulotomy can now be performed exposing the femoral head and allowing posterior dislocation of the hip. Alternatively, the capsule and external rotators can be incised and reflected as a single layer. Instrumentation/ Implantation
1.
Angled reamers can be utilized to help avoid impingement on soft tissues. Procedure ## Step 1
3. The femoral neck is cut with an oscillating saw, the femoral head removed, and attention turned to preparation of the acetabulum.
4.
Ideally, an acetabular retractor with a sharp tip and a light to illuminate the acetabulum should be placed on the anterior rim.
5.
The inferior capsule may need to be divided, and the final step to gain maximum acetabular exposure is flexion and adduction of the femur.
6.
Before reaming, the labrum should be excised and any visible osteophytes removed. The acetabulum is then sequentially reamed under direct vision, making certain the femur does not force the reamer into the posterior column.
7.
Once reaming of the acetabulum is complete, the implant is inserted. ### Minimally Invasive THA
Step 2
-
The femur is prepared under direct vision while protecting the posterior edge of the abductor muscles (
A
in Fig. 3) with a retractor. Positioning the femur in flexion in line with the skin incision and pushing the proximal femur up through the wound can aid greatly with proximal femur exposure (
B
in Fig. 3B).
 ---
---
 118 A Trochanter Femur Abductor muscles Cut femoral neck B
118 A Trochanter Femur Abductor muscles Cut femoral neck B
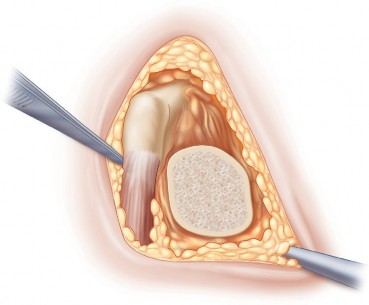 ---
FIGURE 3 119 ### Minimally Invasive THA
---
FIGURE 3 119 ### Minimally Invasive THA
- Four acetabular retractors can now be strategically placed around the anterior, superior, inferior, and posterior aspects of the acetabulum. 2. The labrum should be excised to help visualize the periphery of the acetabulum, and osteophytes removed. 3. Sequential reaming should be performed, ensuring proper placement of the retractors to protect the skin and soft tissue. 4. The cementless implant is inserted under direct visualization. ## Step 2
- To assist with preparation of the femur, one retractor is placed posterior to the femur, and one is placed lateral to it. These retractors can again assist with protecting the skin and soft tissues during reaming and broaching. 6. The femoral canal is prepared as usual, and with the final broach and a trial head and neck in place, a trial reduction is performed to assess limb length, stability, and signs of impingement. 7. The final components are inserted, and the wound is closed in layers, focusing on repair of the gluteus medius tendon back to the femur. ## P EARLS
- This approach obviates the need for special instrumentation, and many surgeons find that acetabular component positioning is easier with this approach. ## P ITFALLS
-
Traction on the limb may facilitate head removal.
Portals/Exposures
14.
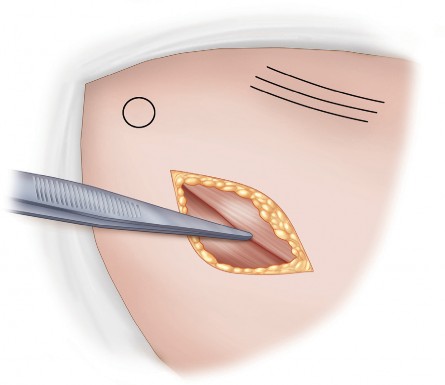
The incision is typically made along the medial border of the tensor fascia lata, and is parallel to a line that connects the anterior superior iliac spine (outlined proximal to the incision in Fig. 5) and the tip of the greater trochanter. The approximate location of the femoral neurovascular bundle should be kept in mind (outlined medial to the incision in Fig. 5). The remainder of the exposure should be done through a modified Smith-Peterson approach. ASIS (outlined) Femoral neurovascular bundle (outlined) Incision direct anterior approach
 ---
FIGURE 5 123 ### Minimally Invasive THA
---
FIGURE 5 123 ### Minimally Invasive THA
-
The initial dissection is through the internervous muscular plane between the sartorius and the tensor fascia lata (Fig. 6). The fascia is incised just lateral to that location to avoid injuring the lateral femoral cutaneous nerve.
 ---
---
 A Forceps Sartorius Tensor fascia lata B
A Forceps Sartorius Tensor fascia lata B
 ---
ASIS (outlined) Femoral neurovascular bundle (outlined) FIGURE 6 124 ### Minimally Invasive THA
---
ASIS (outlined) Femoral neurovascular bundle (outlined) FIGURE 6 124 ### Minimally Invasive THA
- Blunt dissection is used to establish the deep plane of dissection between the gluteus medius laterally and the rectus femoris medially, allowing the interval between the rectus and the hip capsule to be developed. The origin of the rectus femoris is not routinely detached. 16. A narrow Cobra retractor is placed superiorly to better expose the hip capsule. A second Cobra retractor is placed over the superolateral joint capsule, and a third is placed over the inferomedial joint capsule. The latter two retractors should be perpendicular to the femoral neck. 17. The anterior capsule is now excised, exposing the femoral neck, which needs to be osteotomized in situ to dislocate the hip. The neck cut is made and the head is removed using a corkscrew or threaded Steinmann pins. If it is difficult to deliver the entire head through the wound, an additional cut may need to be made at the head-neck junction. Procedure ## Step 1
- Three narrow Cobra retractors placed around the rim of the acetabulum are used to gain complete visualization for acetabular preparation. Any remaining labrum and osteophytes should be excised. 19. At this point, the sandbag, bump, or bolster can be either removed or deflated from underneath the buttock so that reaming is done in the anatomic supine position. 20. The acetabulum is sequentially reamed, and the acetabular component is impacted into place. ## Step 2
- The anterior incision and approach for exposure of the acetabulum is virtually identical to that in the direct anterior approach described above. The incision can be confirmed with fluoroscopy to be a line between the posterior acetabulum and the intertrochanteric line, in line with the femoral neck. 28. The remainder of the acetabular exposure should be done through a modified Smith-Peterson approach (see above). ## Femur
- The sandbag, bump, or bolster is reinserted or reinflated. 30. The location of the posterior incision is critical, and it should allow straight access to the femoral canal. There are two commonly used methods to ensure proper position of the posterior incision. 1. First, the axes of the femoral shaft in the anteroposterior and lateral planes are palpated and drawn with the femur in adduction and external rotation. The point at which these two lines intersect proximally is the location of the posterior incision. 127 ### Minimally Invasive THA
- An alternative method utilizes a curved instrument (awl) passed through the anterior incision and through the superior capsular opening. This tents the skin posteriorly in line with the femoral shaft, where a small incision is made. After the incision is made, the subcutaneous tissues are spread using long, curved scissors, and a soft tissue passage to the hip joint is blindly developed by aiming the scissors toward the surgeon’s opposite finger, which is in the anterior incision within the superior hip capsule. Spreading the tissues using this technique creates a pathway to the femoral canal posterior to the abductors. Procedure ## Step 1
- When it comes time for preparation of the acetabulum, fluoroscopy can be used to verify alignment and appropriate medialization of the reamers. 2. The cementless acetabular component is impacted into place using an offset inserter, again using fluoroscopy to ensure proper abduction and anteversion. ## Step 2
- With the two-incision technique, femoral instrumentation and implant insertion are done blindly, utilizing fluoroscopy and palpation through the anterior incision. It is important to keep the limb adducted with slight flexion to maintain the proper relationship between the soft tissue passage and the femoral canal. 4. After the opening is lateralized into the canal, reaming and broaching are performed under fluoroscopic guidance. Broach stability can be assessed with visual confirmation through the anterior incision. If the broach should get caught up on the hip capsule, the capsule can be released as necessary. 5. The femoral component is inserted under fluoroscopic guidance, and alignment and depth are confirmed visually through the anterior incision. ## Step 3
-
The neck of the prosthesis is delivered into the anterior incision, which is achieved with an assistant applying traction and the surgeon manipulating the neck using a large bone hook with gentle flexion, abduction, and external rotation of the femur. Trial A B
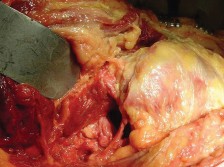 ---
FIGURE 8 reductions can now be performed, and limb length, stability, and signs of impingement are assessed as usual. 128 ### Minimally Invasive THA
---
FIGURE 8 reductions can now be performed, and limb length, stability, and signs of impingement are assessed as usual. 128 ### Minimally Invasive THA
- Once the appropriate neck length is determined, the trial head is removed, and the real component is impacted in place. The hip is reduced, and wounds are copiously irrigated. ## Step 4
- <a class="medical-citation-link" href="https://pubmed.ncbi.nlm.nih.gov/?term=Elderly%20and%20obese%20females%20are%20at%20greatest%20risk%20of%20developing%20a%20complication%20with%20this%20approach.%205.%20The%20technical%20difficulty%20of%20this%20approach%20is%20reflected%20in%20longer%20operative%20times%20and%20a%20greater%20variability%20in%20operative%20times%20when%20compared%20with%20traditional%20THA%20%28Pagnano%20et%20al.%2C%202005%29.%20In%20addition%2C%20reoperation%20rates%20as%20high%20as%2010%25%20have%20been%20reported%20%28Bal%20et%20al.%2C%202006%29.%206.%20The%20potential%20benefit%20of%20less%20soft%20tissue%20dissection%20certainly%20may%20not%20be%20the%20case%2C%20as%20significant%20damage%20has%20been%20shown%20to%20occur%20to%20the%20gluteus%20medius%20and%20gluteus%20minimus%20muscles%20%28Mardones%20et%20al.%2C%202005%29.%20Figure%208%20demonstrates%20gluteus%20medius%20muscle%20injury%20%28A%29%20in%20a%20cadaveric%20specimen%20that%20occurred%20with%20the%20two-incision%20approach%20%28B%20indicates%20the%20greater%20trochanter%29.%207.%20Most%20authors%20agree%20that%20the%20high%20complication%20rate%20is%20at%20least%20partly%20due%20to%20the%20so-called%20learning-curve%20effect%20%28Pagnano%20et%20al.%2C%202005%29.%20Slight%20modifications%20to%20the%20procedure%20may%20assist%20in%20bringing%20about%20more%20favorable%20outcomes.%20For%20example%2C%20one%20author%20has%20eliminated%20intraoperative%20fluoroscopy%2C%20stating%20that%20it%20may%20mislead%20the%20surgeon%20and%20provide%20a%20false%20sense%20of%20security%20%28Bal%20et%20al.%2C%202006%29.%20It%20is%20emphasized%20that%20implant%20position%20is%20dependent%20on%20adequate%20129%20%23%23%23%20Minimally%20Invasive%20THA%20visualization%2C%20anatomic%20landmarks%2C%20and%20instrument%20guides.%20The%20technique%20undoubtedly%20is%20technically%20challenging%2C%20and%20proper%20training%2C%20including%20cadaveric%20training%2C%20is%20necessary%20to%20minimize%20complications%20and%20ensure%20success%20%28Berger%20and%20Duwelius%2C%202004%29.%20Evidence%20Asayama%20I%2C%20Kinsey%20TL%2C%20Mahoney%20OM.%20Two-year%20experience%20using%20a%20limited-incision%20direct%20lateral%20approach%20in%20total%20hip%20arthroplasty.%20J%20Arthroplasty.%202006%3B21%3A1083%E2%80%9391.%20Retrospective%20early%20experience%20documenting%20satisfactory%20results%20with%20limited%20incision%20direct%20lateral%20approach.%20Bal%20BS%2C%20Haltom%20D%2C%20Aleto%20T%2C%20Barrett%20M.%20Early%20complications%20of%20primary%20total%20hip%20replacement%20performed%20with%20a%20two-incision%20minimally%20invasive%20technique%3A%20surgical%20technique.%20J%20Bone%20Joint%20Surg%20%5BAm%5D.%202006%3B88%28Suppl%201%20Pt%202%29%3A221%E2%80%9333.%20Retrospective%20case%20series%20review%20documenting%20substantial%20early%20complication%20rate%20with%20two-incision%20THA.%20Berger%20RA%2C%20Duwelius%20PJ.%20The%20two-incision%20minimally%20invasive%20total%20hip%20arthroplasty%3A%20technique%20and%20results.%20Orthop%20Clin%20North%20Am.%202004%3B35%3A163%E2%80%9372.%20This%20study%20showed%20rapid%20rehabilitation%2C%20quick%20return%20to%20activities%20of%20daily%20living%2C%20and%20a%20low%20prevalence%20of%20complications%20following%20minimally%20invasive%20THA%20done%20through%20two%20incisions.%20Chimento%20GF%2C%20Pavone%20V%2C%20Sharrock%20N%2C%20Kahn%20B%2C%20Cahill%20J%2C%20Sculco%20TP.%20Minimally%20invasive%20total%20hip%20arthroplasty%3A%20a%20prospective%20randomized%20study.%20J%20Arthroplasty.%202005%3B20%3A%20139%E2%80%9344.%20A%20prospective%2C%20randomized%20study%20showed%20a%20mini-posterior%20THA%20group%20to%20have%20less%20intraoperative%20and%20total%20blood%20loss%20and%20less%20of%20a%20limp%20at%206%20weeks%20when%20compared%20with%20standard%20THA%2C%20although%20there%20was%20no%20functional%20difference%20at%201%20and%202%20years%E2%80%99%20follow-up.%20Ciminiello%20M%2C%20Parvizi%20J%2C%20Sharkey%20PF%2C%20Eslampour%20A%2C%20Rothman%20RH.%20Total%20hip%20arthroplasty%3A%20is%20small%20incision%20better%3F%20J%20Arthroplasty.%202006%3B21%3A484%E2%80%938.%20Kennon%20RE%2C%20Keggi%20JM%2C%20Wetmore%20RS%2C%20Zatorski%20LE%2C%20Huo%20MH%2C%20Keggi%20KJ.%20Total%20hip%20arthroplasty%20through%20a%20minimally%20invasive%20anterior%20surgical%20approach.%20J%20Bone%20Joint%20Surg%20%5BAm%5D.%202003%3B85%28Suppl%204%29%3A39%E2%80%9348.%20Mardones%20R%2C%20Pagnano%20MW%2C%20Nemanich%20JP%2C%20Trousdale%20RT.%20The%20Frank%20Stinchfield%20Award%3A%20Muscle%20damage%20after%20total%20hip%20arthroplasty%20done%20with%20the%20two-incision%20and%20mini-posterior%20techniques.%20Clin%20Orthop%20Relat%20Res.%202005%3B%28441%29%3A63%E2%80%937.%20Vail%20TP.%20Mini-incision%20THA%3A%20posterior%20approach.%20In%20Lieberman%20JR%2C%20Berry%20DJ%20%28eds%29.%20Advanced%20Reconstruction%20Hip.%20Rosemont%2C%20IL%3A%20American%20Academy%20of%20Orthopaedic%20Surgeons%2C%202005%3A17%E2%80%9340.%20In%20a%20cadaveric%20study%2C%20there%20was%20measurable%20damage%20to%20the%20abductors%20and%20gluteus%20minimus%20when%20a%20mini-posterior%20approach%20was%20performed%2C%20although%20the%20damage%20to%20the%20abductor%20mechanism%20was%20less%20when%20compared%20to%20the%20two-incision%20approach%2C%20in%20which%20mean%20abductor%20and%20gluteus%20minimus%20muscle%20damage%20exceeded%2015%25%20and%2017%25%2C%20respectively.%20Meneghini%20RM%2C%20Pagnano%20MW%2C%20Trousdale%20RT%2C%20Hozack%20WJ.%20Muscle%20damage%20during%20MIS%20total%20hip%20arthroplasty%3A%20Smith-Petersen%20versus%20posterior%20approach.%20Clin%20Orthop%20Relat%20Res.%202006%3B%28453%29%3A293%E2%80%938.%20In%20a%20cadaveric%20study%2C%20a%20mean%20of%208%25%20of%20the%20gluteus%20minimus%20muscles%20and%2031.2%25%20of%20the%20tensor%20fasciae%20latae%20were%20damaged%20using%20the%20direct%20anterior%20approach%2C%20and%20in%2050%25%20of%20the%20cases%20the%20piriformis%20and/or%20conjoined%20tendon%20avulsed%20with%20mobilization%20of%20the%20femur.%20Muscle%20damage%20of%20some%20degree%20was%20found%20in%20all%20specimens.%20This%20study%20also%20showed%20that%2C%20in%20addition%20to%20the%20intentional%20detachment%20of%20the%20piriformis%20and%20conjoined%20tendon%2C%20there%20was%20also%20measurable%20damage%20to%20the%20abductors%20and%20gluteus%20minimus%20in%20each%20specimen%20in%20which%20a%20mini-posterior%20approach%20was%20performed.%20130%20%23%23%23%20Minimally%20Invasive%20THA%20O%E2%80%99Brien%20DA%2C%20Rorabeck%20CH.%20The%20mini-incision%20direct%20lateral%20approach%20in%20primary%20total%20hip%20arthroplasty.%20Clin%20Orthop%20Relat%20Res.%202005%3B%28441%29%3A99%E2%80%93103.%20This%20series%20retrospectively%20compared%20mini-anterolateral%20THA%20to%20standard%20anterolateral%20THA%20and%20showed%20signi%EF%AC%81cantly%20decreased%20operative%20time%20as%20well%20as%20length%20of%20hospital%20stay%20with%20the%20mini%20approach.%20The%20series%20showed%20no%20difference%20with%20regard%20to%20complications%2C%20need%20for%20blood%20transfusion%2C%20or%20component%20malposition.%20Ogonda%20L%2C%20Wilson%20R%2C%20Archbold%20P%2C%20Lawlor%20M%2C%20Humphreys%20P%2C%20O%E2%80%99Brien%20S%2C%20Beverland%20D.%20A%20minimal-incision%20technique%20in%20total%20hip%20arthroplasty%20does%20not%20improve%20early%20postoperative%20outcomes%3A%20a%20prospective%2C%20randomized%2C%20controlled%20trial.%20J%20Bone%20Joint%20Surg%20%5BAm%5D.%202005%3B87%3A701%E2%80%9310.%20A%20prospective%2C%20randomized%2C%20controlled%20trial%20showed%20no%20difference%20with%20respect%20to%20postoperative%20hematocrit%2C%20blood%20transfusion%20requirements%2C%20pain%20scores%2C%20early%20walking%20ability%2C%20length%20of%20hospital%20stay%2C%20femoral%20component%20cement%20mantle%2C%20functional%20outcome%20scores%20at%206%20weeks%2C%20or%20component%20positioning.%20Pagnano%20MW%2C%20Leone%20J%2C%20Lewallen%20DG%2C%20Hanssen%20AD.%20Two-incision%20THA%20had%20modest%20outcomes%20and%20some%20substantial%20complications.%20Clin%20Orthop%20Relat%20Res.%202005%3B%28441%29%3A86%E2%80%9390.%20In%20this%20series%2C%20most%20of%20the%20technical%20dif%EF%AC%81culties%20occurred%20on%20the%20femoral%20side%2C%20and%20placement%20of%20the%20acetabular%20component%20through%20the%20direct%20anterior%20approach%20was%20straightforward%20and%20presented%20few%20challenges.%20Fourteen%20percent%20of%20patients%20had%20a%20complication%2C%20with%205%25%20requiring%20reoperation.%20Pagnano%20MW%2C%20Trousdale%20RT%2C%20Meneghini%20RM%2C%20Hanssen%20AD.%20Patients%20preferred%20a%20mini-posterior%20THA%20to%20a%20contralateral%20two-incision%20THA.%20Clin%20Orthop%20Relat%20Res.%202006%3B%28453%29%3A156%E2%80%939.%20This%20study%20reported%20on%2026%20patients%20who%20had%20both%20a%20mini-posterior%20THA%20and%20a%20two-incision%20THA%20on%20the%20contralateral%20hip.%20There%20were%20no%20differences%20with%20respect%20to%20ambulation%2C%20return%20to%20driving%2C%20stair%20climbing%2C%20return%20to%20work%2C%20or%20walking%20%C2%BD%20mile.%20Sixteen%20of%20the%2026%20patients%20preferred%20their%20mini-posterior%20THA%20over%20their%20two-incision%20THA%2C%20and%20two%20had%20no%20preference.%20Rachbauer%20F.%20%5BMinimally%20invasive%20total%20hip%20arthroplasty%20via%20direct%20anterior%20approach.%5D%20Orthopade.%202005%3B34%3A1103%E2%80%934%2C%201106%E2%80%938%2C%201110.%20In%20a%20prospective%20study%2C%20it%20was%20shown%20that%20minimally%20invasive%20THA%20via%20the%20direct%20anterior%20approach%20allowed%20correct%20positioning%20of%20all%20components%2C%20little%20blood%20loss%20or%20postoperative%20pain%2C%20decreased%20hospital%20stays%2C%20and%20accelerated%20rehabilitation.%20Of%20the%20100%20patients%20in%20the%20series%2C%20there%20were%20six%20permanent%20lesions%20of%20the%20lateral%20femoral%20cutaneous%20nerve.%20Teet%20JS%2C%20Skinner%20HB%2C%20Khoury%20L.%20The%20effect%20of%20the%20%E2%80%9Cmini%E2%80%9D%20incision%20in%20total%20hip%20arthroplasty%20on%20component%20position.%20J%20Arthroplasty.%202006%3B21%3A503%E2%80%937.%20A%20series%20using%20the%20mini-posterior%20THA%20showed%20worrisome%20results%20regarding%20cemented%20femoral%20components%2C%20with%20a%20slight%20propensity%20toward%20varus%20malpositioning%20that%20could%20complicate%20long-term%20outcomes.%20Wenz%20JF%2C%20Gurkan%20I%2C%20Jibodh%20SR.%20Mini-incision%20total%20hip%20arthroplasty%3A%20a%20comparative%20assessment%20of%20perioperative%20outcomes.%20Orthopedics.%202002%3B25%3A1031%E2%80%9343.%20An%20early%20series%20showed%20that%20patients%20with%20mini-posterior%20THA%20had%20signi%EF%AC%81cantly%20earlier%20ambulation%20with%20less%20transfer%20assistance%20needed%2C%20as%20well%20as%20less%20blood%20transfusion%20requirements.%20Woolson%20ST%2C%20Mow%20CS%2C%20Syquia%20JF%2C%20Lannin%20JV%2C%20Schurman%20DJ.%20Comparison%20of%20primary%20total%20hip%20replacements%20performed%20with%20a%20standard%20incision%20or%20a%20mini-incision.%20J%20Bone%20Joint%20Surg%20%5BAm%5D.%202004%3B86%3A1353%E2%80%938.%20%20This%20series%20showed%20no%20difference%20with%20respect%20to%20variables%20such%20as%20blood%20loss%20and%20surgical%20time%2C%20but%20the%20mini-incision%20group%20was%20found%20to%20have%20a%20signi%EF%AC%81cantly%20higher%20risk%20of%20wound%20complications%2C%20higher%20percentage%20of%20acetabular%20component%20malposition%2C%20and%20poor%20%E2%80%9C%EF%AC%81t%20and%20%EF%AC%81ll%E2%80%9D%20of%20cementless%20femoral%20components." target="_blank" rel="noopener noreferrer" target="Elderly and obese females are at greatest risk of developing a complication with this approach. 5. The technical difficulty of this approach is reflected in longer operative times and a greater variability in operative times when compared with traditional THA (Pagnano et al., 2005). In addition, reoperation rates as high as 10% have been reported (Bal et al., 2006). 6. The potential benefit of less soft tissue dissection certainly may not be the case, as significant damage has been shown to occur to the gluteus medius and gluteus minimus muscles (Mardones et al., 2005). Figure 8 demonstrates gluteus medius muscle injury (A) in a cadaveric specimen that occurred with the two-incision approach (B indicates the greater trochanter). 7. Most authors agree that the high complication rate is at least partly due to the so-called learning-curve effect (Pagnano et al., 2005). Slight modifications to the procedure may assist in bringing about more favorable outcomes. For example, one author has eliminated intraoperative fluoroscopy, stating that it may mislead the surgeon and provide a false sense of security (Bal et al., 2006). It is emphasized that implant position is dependent on adequate 129 ### Minimally Invasive THA visualization, anatomic landmarks, and instrument guides. The technique undoubtedly is technically challenging, and proper training, including cadaveric training, is necessary to minimize complications and ensure success (Berger and Duwelius, 2004). Evidence Asayama I, Kinsey TL, Mahoney OM. Two-year experience using a limited-incision direct lateral approach in total hip arthroplasty. J Arthroplasty. 2006;21:1083–91. Retrospective early experience documenting satisfactory results with limited incision direct lateral approach. Bal BS, Haltom D, Aleto T, Barrett M. Early complications of primary total hip replacement performed with a two-incision minimally invasive technique: surgical technique. J Bone Joint Surg [Am]. 2006;88(Suppl 1 Pt 2):221–33. Retrospective case series review documenting substantial early complication rate with two-incision THA. Berger RA, Duwelius PJ. The two-incision minimally invasive total hip arthroplasty: technique and results. Orthop Clin North Am. 2004;35:163–72. This study showed rapid rehabilitation, quick return to activities of daily living, and a low prevalence of complications following minimally invasive THA done through two incisions. Chimento GF, Pavone V, Sharrock N, Kahn B, Cahill J, Sculco TP. Minimally invasive total hip arthroplasty: a prospective randomized study. J Arthroplasty. 2005;20: 139–44. A prospective, randomized study showed a mini-posterior THA group to have less intraoperative and total blood loss and less of a limp at 6 weeks when compared with standard THA, although there was no functional difference at 1 and 2 years’ follow-up. Ciminiello M, Parvizi J, Sharkey PF, Eslampour A, Rothman RH. Total hip arthroplasty: is small incision better? J Arthroplasty. 2006;21:484–8. Kennon RE, Keggi JM, Wetmore RS, Zatorski LE, Huo MH, Keggi KJ. Total hip arthroplasty through a minimally invasive anterior surgical approach. J Bone Joint Surg [Am]. 2003;85(Suppl 4):39–48. Mardones R, Pagnano MW, Nemanich JP, Trousdale RT. The Frank Stinchfield Award: Muscle damage after total hip arthroplasty done with the two-incision and mini-posterior techniques. Clin Orthop Relat Res. 2005;(441):63–7. Vail TP. Mini-incision THA: posterior approach. In Lieberman JR, Berry DJ (eds). Advanced Reconstruction Hip. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2005:17–40. In a cadaveric study, there was measurable damage to the abductors and gluteus minimus when a mini-posterior approach was performed, although the damage to the abductor mechanism was less when compared to the two-incision approach, in which mean abductor and gluteus minimus muscle damage exceeded 15% and 17%, respectively. Meneghini RM, Pagnano MW, Trousdale RT, Hozack WJ. Muscle damage during MIS total hip arthroplasty: Smith-Petersen versus posterior approach. Clin Orthop Relat Res. 2006;(453):293–8. In a cadaveric study, a mean of 8% of the gluteus minimus muscles and 31.2% of the tensor fasciae latae were damaged using the direct anterior approach, and in 50% of the cases the piriformis and/or conjoined tendon avulsed with mobilization of the femur. Muscle damage of some degree was found in all specimens. This study also showed that, in addition to the intentional detachment of the piriformis and conjoined tendon, there was also measurable damage to the abductors and gluteus minimus in each specimen in which a mini-posterior approach was performed. 130 ### Minimally Invasive THA O’Brien DA, Rorabeck CH. The mini-incision direct lateral approach in primary total hip arthroplasty. Clin Orthop Relat Res. 2005;(441):99–103. This series retrospectively compared mini-anterolateral THA to standard anterolateral THA and showed significantly decreased operative time as well as length of hospital stay with the mini approach. The series showed no difference with regard to complications, need for blood transfusion, or component malposition. Ogonda L, Wilson R, Archbold P, Lawlor M, Humphreys P, O’Brien S, Beverland D. A minimal-incision technique in total hip arthroplasty does not improve early postoperative outcomes: a prospective, randomized, controlled trial. J Bone Joint Surg [Am]. 2005;87:701–10. A prospective, randomized, controlled trial showed no difference with respect to postoperative hematocrit, blood transfusion requirements, pain scores, early walking ability, length of hospital stay, femoral component cement mantle, functional outcome scores at 6 weeks, or component positioning. Pagnano MW, Leone J, Lewallen DG, Hanssen AD. Two-incision THA had modest outcomes and some substantial complications. Clin Orthop Relat Res. 2005;(441):86–90. In this series, most of the technical difficulties occurred on the femoral side, and placement of the acetabular component through the direct anterior approach was straightforward and presented few challenges. Fourteen percent of patients had a complication, with 5% requiring reoperation. Pagnano MW, Trousdale RT, Meneghini RM, Hanssen AD. Patients preferred a mini-posterior THA to a contralateral two-incision THA. Clin Orthop Relat Res. 2006;(453):156–9. This study reported on 26 patients who had both a mini-posterior THA and a two-incision THA on the contralateral hip. There were no differences with respect to ambulation, return to driving, stair climbing, return to work, or walking ½ mile. Sixteen of the 26 patients preferred their mini-posterior THA over their two-incision THA, and two had no preference. Rachbauer F. [Minimally invasive total hip arthroplasty via direct anterior approach.] Orthopade. 2005;34:1103–4, 1106–8, 1110. In a prospective study, it was shown that minimally invasive THA via the direct anterior approach allowed correct positioning of all components, little blood loss or postoperative pain, decreased hospital stays, and accelerated rehabilitation. Of the 100 patients in the series, there were six permanent lesions of the lateral femoral cutaneous nerve. Teet JS, Skinner HB, Khoury L. The effect of the “mini” incision in total hip arthroplasty on component position. J Arthroplasty. 2006;21:503–7. A series using the mini-posterior THA showed worrisome results regarding cemented femoral components, with a slight propensity toward varus malpositioning that could complicate long-term outcomes. Wenz JF, Gurkan I, Jibodh SR. Mini-incision total hip arthroplasty: a comparative assessment of perioperative outcomes. Orthopedics. 2002;25:1031–43. An early series showed that patients with mini-posterior THA had significantly earlier ambulation with less transfer assistance needed, as well as less blood transfusion requirements. Woolson ST, Mow CS, Syquia JF, Lannin JV, Schurman DJ. Comparison of primary total hip replacements performed with a standard incision or a mini-incision. J Bone Joint Surg [Am]. 2004;86:1353–8. This series showed no difference with respect to variables such as blood loss and surgical time, but the mini-incision group was found to have a significantly higher risk of wound complications, higher percentage of acetabular component malposition, and poor “fit and fill” of cementless femoral components.</a>
You Might Also Like


