Mastering Complications in Total Hip Arthroplasty: Prevention, Diagnosis, and Evidence-Based Management

Key Takeaway
Complications in total hip arthroplasty (THA) range from intraoperative challenges to late postoperative systemic events. Effective management requires rigorous preoperative optimization, meticulous surgical hemostasis, and targeted prophylaxis. This guide details evidence-based protocols for mitigating mortality, hematoma formation, heterotopic ossification, and thromboembolic disease, ensuring orthopedic surgeons can optimize patient outcomes and implant longevity.
COMPLICATIONS IN TOTAL HIP ARTHROPLASTY
Complications associated with total hip arthroplasty (THA) can be broadly stratified into those directly related to the surgical procedure—occurring in the intraoperative, early postoperative, and late postoperative periods—and systemic events that affect nonmusculoskeletal organ systems within the perioperative time frame. As with any major orthopedic intervention, the prevention of complications must remain the consistent focus of the operating surgeon and the multidisciplinary care team. Rigorous surveillance and the rapid, effective treatment of complications have a dramatic effect on patient satisfaction, implant survivorship, and overall functional outcomes.

PERIOPERATIVE MORTALITY
Reported mortality rates following total hip arthroplasty vary significantly depending on the historical time period of the surgical cohort, the postoperative end point at which the rate was determined (e.g., 30-day vs. 90-day), and the specific patient population being evaluated.
In-hospital mortality rates generally range from 0.16% to 0.52% in modern cohorts. Mortality at 90 days postoperatively in the U.S. Medicare population has been reported at approximately 1% for primary total hip arthroplasty and elevates to 2.5% for revision surgery.
Risk Stratification and Optimization
Increased mortality rates have been consistently reported in specific demographic and clinical subsets:
* Male patients.
* Patients older than 70 years of age.
* Patients with preexisting cardiovascular disease, pulmonary compromise, or chronic kidney disease.
Clinical Pearl: Although careful preoperative medical evaluation is warranted in all patients, special attention and multidisciplinary optimization (Cardiology, Pulmonology, Geriatrics) must be directed to patients exhibiting these high-risk factors to mitigate perioperative mortality.


HEMATOMA FORMATION AND HEMORRHAGE
Preoperative Screening and Risk Factors
Careful preoperative screening is mandatory to identify patients with known risk factors for excessive hemorrhage. A comprehensive hematologic history must evaluate:
* Current antiplatelet, anti-inflammatory, or anticoagulant drug therapy.
* Use of herbal medications and supplements known to affect the coagulation cascade (e.g., Ginkgo biloba, Ginseng, Garlic, Vitamin E).
* Undiagnosed blood dyscrasias and coagulopathies (e.g., von Willebrand disease, Factor deficiencies).
* Family or patient history of excessive bleeding with previous surgical procedures or dental extractions.

Surgical Hemostasis and Vascular Anatomy
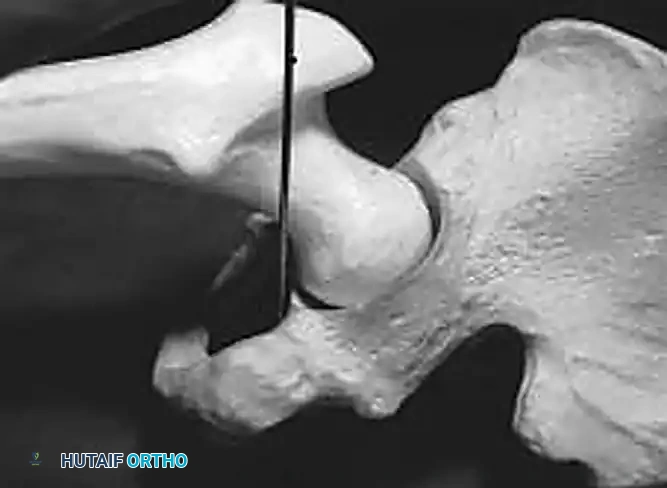
The most critical surgical factor in preventing postoperative hematomas is meticulous, proactive hemostasis. The surgeon must possess an intimate understanding of the periarticular vascular anatomy. Common sources of significant bleeding include:
- Obturator Vessels: Branches may be inadvertently transected when the ligamentum teres, transverse acetabular ligament, and inferior acetabular osteophytes are excised.
- Profunda Femoris: The first perforating branch of the profunda femoris, located deep to the gluteus maximus insertion, is highly vulnerable during femoral exposure and release.
- Femoral Vessels: Branches near the anterior capsule can be injured during anterior capsulectomy or retractor placement.
- Gluteal Vessels: Branches of the inferior and superior gluteal vessels may be compromised during posterior and lateral approaches.
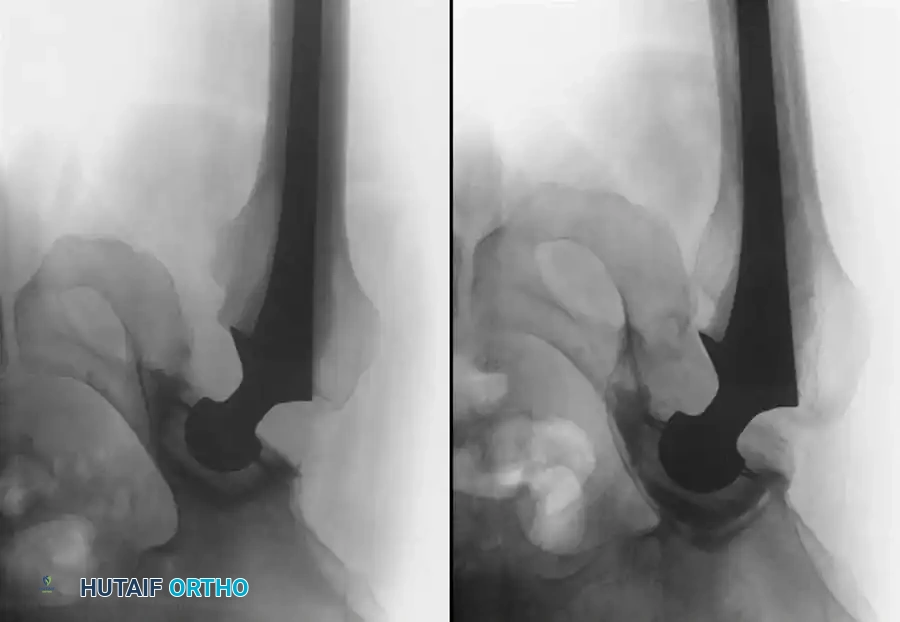
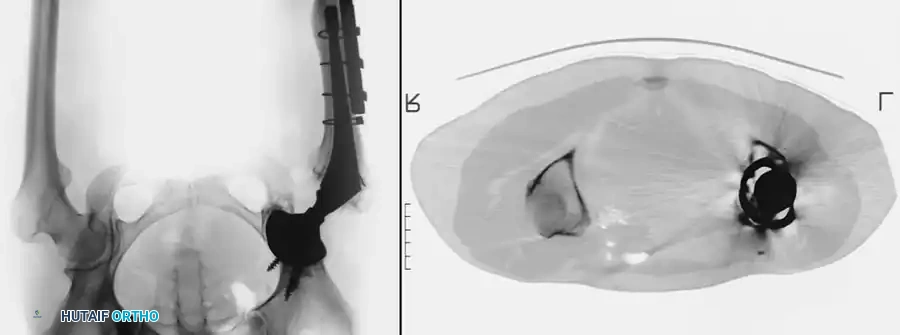
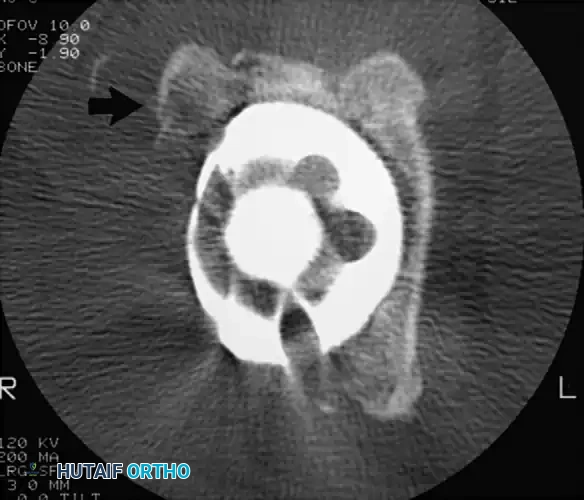
Surgical Warning: Injury to the major iliac vessels may result from catastrophic penetration of the medial wall of the acetabulum, particularly during the removal of a medially displaced or protrusio cup. Bleeding from a large vessel injury usually becomes apparent immediately during the operation and requires emergent vascular surgery consultation.
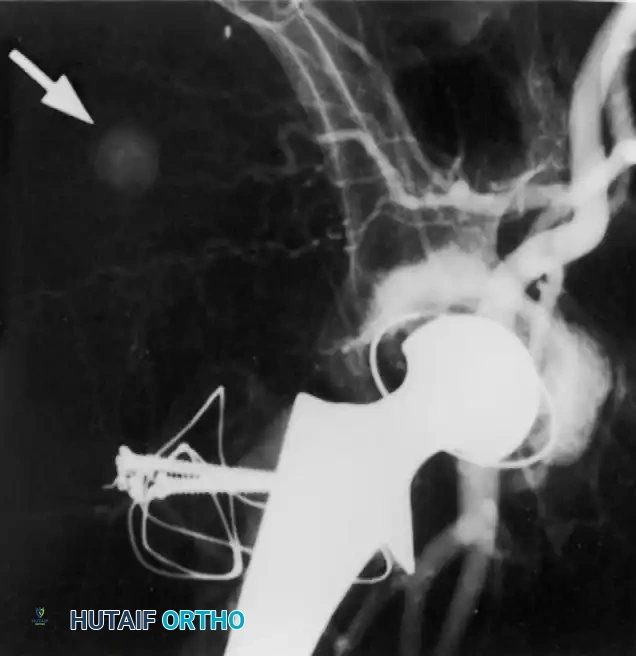
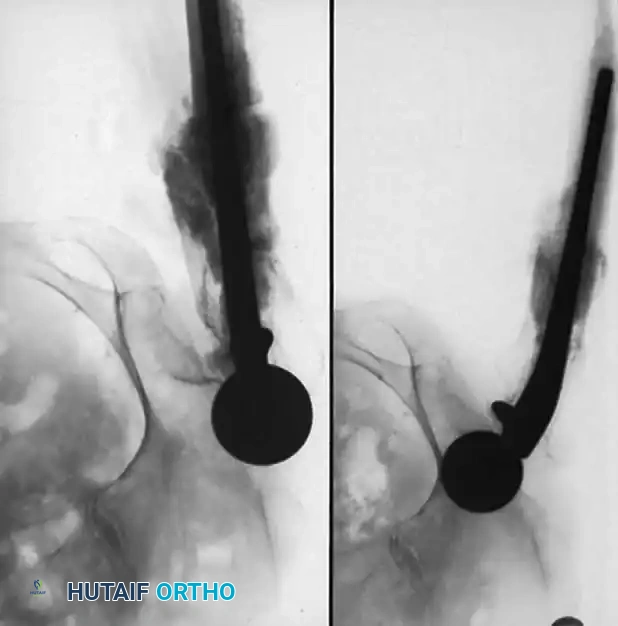
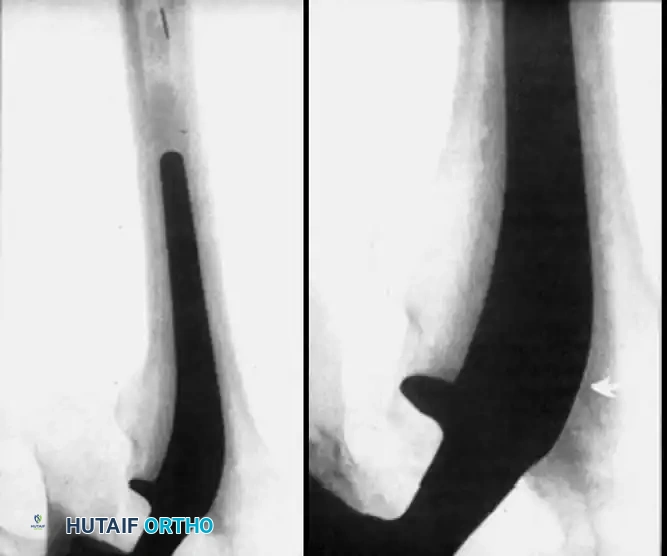
Late bleeding (≥ 1 week postoperatively) may occur secondary to a false aneurysm. In such cases, arteriography is required for the precise identification of the affected vessel, often followed by therapeutic embolization.


The Role of Closed Suction Drainage
The routine use of closed suction drainage remains a topic of debate. Historically, drains were placed deep to the fascia and removed in 24 to 48 hours. However, in patients without excessive bleeding at the time of surgery or specific risk factors for hemorrhage, drainage is generally not required after primary THA.
Drains are still routinely utilized for:
* Revision procedures.
* Primary surgeries with increased intraoperative hemorrhage.
* Patients with known coagulopathies.
The overall benefit of closed suction drainage in uncomplicated primary arthroplasties is unproven. Studies by Hallstrom and Steele, as well as Acus et al., demonstrated that drain usage actually increased the requirements for allogeneic transfusion and resulted in a higher incidence of superficial wound healing problems. Furthermore, a randomized prospective study by Niskanen et al. reported no significant difference in wound healing, transfusion requirements, complications, or range of motion in patients treated with or without closed suction drainage, though the undrained group did experience more soaked dressings requiring reinforcement.

Management of Postoperative Hematoma
Excessive hemorrhage leading to a tense hematoma uncommonly requires surgical intervention. Most patients can be successfully managed non-operatively through:
* Frequent sterile dressing changes.
* Temporary discontinuation or reversal of anticoagulants.
* Correction of underlying coagulopathy.
* Close clinical observation of the wound margins.
Indications for Surgical Evacuation:
Surgical treatment of a hematoma is strictly indicated in the presence of:
1. Wound dehiscence or marginal skin necrosis.
2. Impending or established compartment syndrome of the thigh.
3. Suspected infected hematoma.
Evacuation of the hematoma and the achievement of meticulous hemostasis must be accomplished in the operating room under strict aseptic conditions. The hematoma must be cultured (aerobic, anaerobic, acid-fast, and fungal) to assess for bacterial contamination. Broad-spectrum intravenous antibiotics should be initiated post-culture and continued until final results are available. Radical débridement of necrotic tissue and a watertight fascial closure are mandatory. Closed suction drainage is highly warranted in this specific revision setting to avoid recurrence.

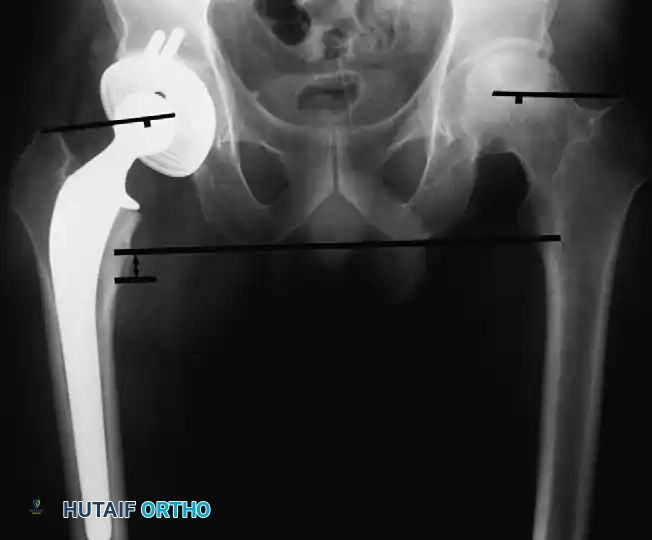
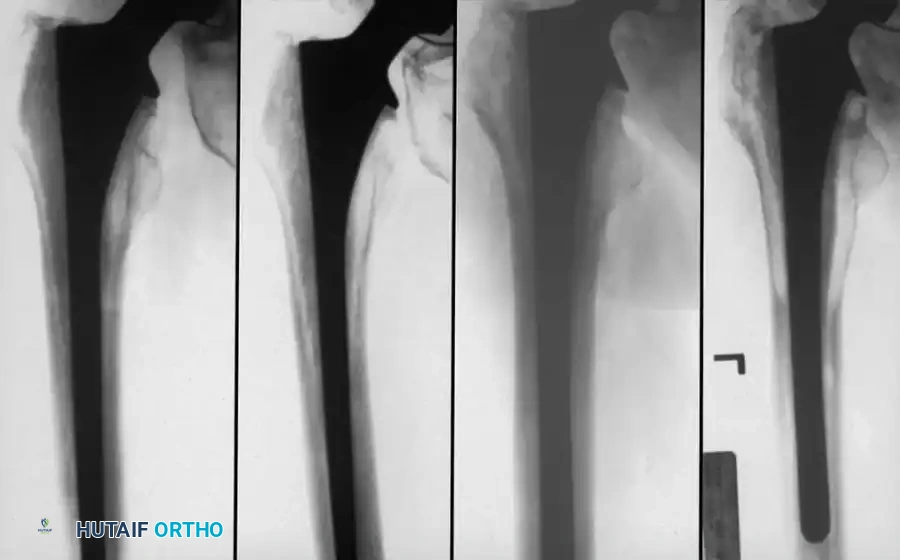
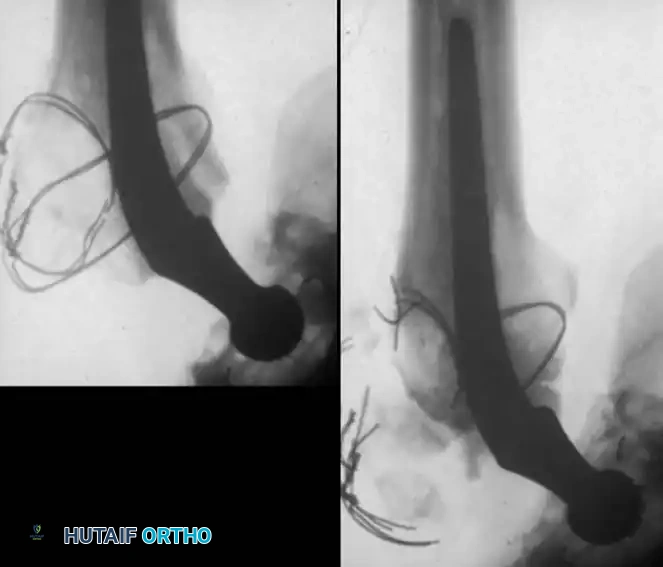
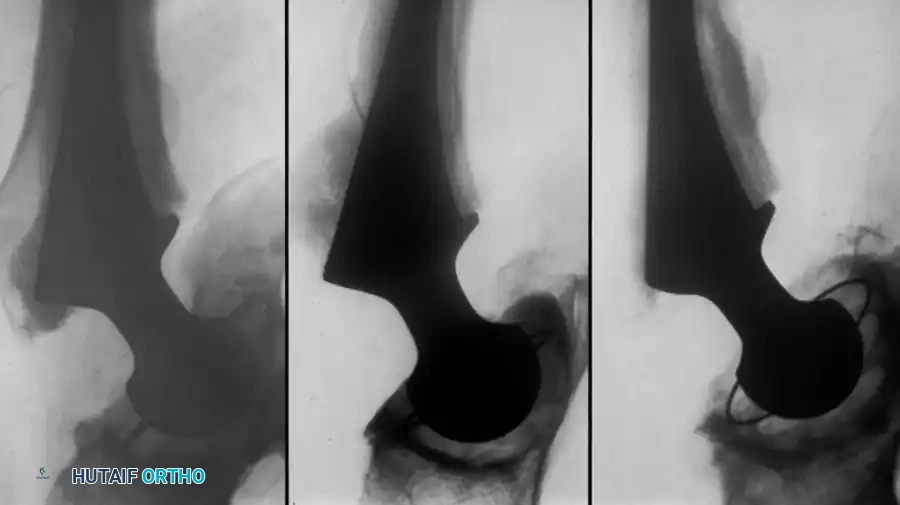
HETEROTOPIC OSSIFICATION (HO)
Postoperative heterotopic ossification (HO) varies dramatically in its clinical and radiographic presentation, ranging from a faint, indistinct density seen in the region of the abductors and iliopsoas to complete, debilitating bony ankylosis of the hip joint.
Pathophysiology and Risk Factors
According to Iorio and Healy, specific patient populations are at a significantly elevated risk for developing HO:
* High Risk: Male patients with hypertrophic osteoarthritis, patients with a prior history of heterotopic ossification, or those with posttraumatic arthritis accompanied by hypertrophic osteophytosis.
* Moderate Risk: Patients with ankylosing spondylitis, diffuse idiopathic skeletal hyperostosis (DISH), Paget disease, and unilateral hypertrophic osteoarthritis.
Surgical technique and approach also play a critical role. Anterior and anterolateral approaches carry a higher risk of heterotopic ossification compared to transtrochanteric or posterior approaches, likely due to the extent of direct muscle trauma to the gluteus minimus and medius. While cementless fixation was historically implicated as a risk factor, subsequent robust prospective randomized and matched-pair studies have definitively refuted this association.


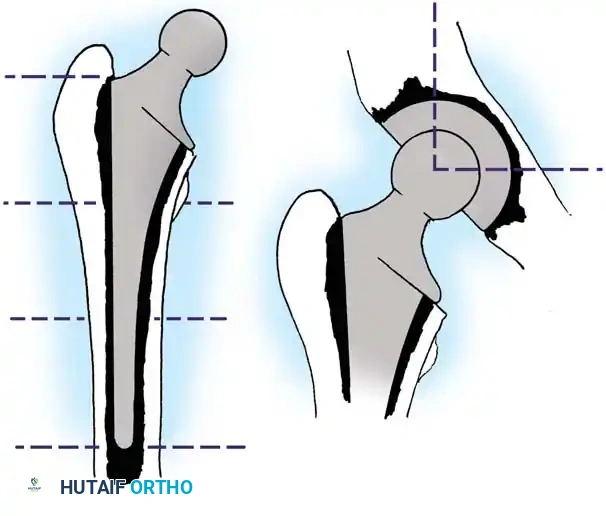
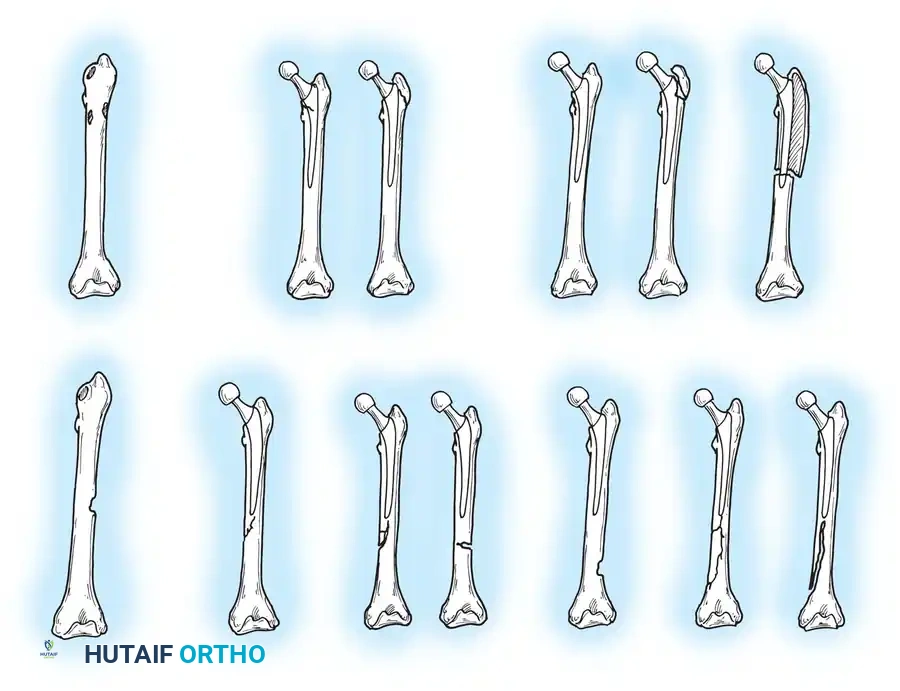
Brooker Classification System
Calcification can typically be visualized radiographically by the third or fourth postoperative week; however, the ectopic bone does not mature fully for 1 to 2 years. The classification system developed by Brooker et al. remains the gold standard for describing the extent of bone formation:
- Grade I: Islands of bone within the soft tissues.
- Grade II: Bone spurs originating from the proximal femur or pelvis with at least 1 cm of space between opposing bone surfaces.
- Grade III: Bone spurs originating from the proximal femur or pelvis with less than 1 cm of space between opposing bone surfaces.
- Grade IV: Complete radiographic bony ankylosis.
The overall prevalence of this complication averages approximately 10% in modern series, though historical data by Riegler and Harris reported occurrences in up to 50% of patients. Fortunately, most patients who develop HO remain asymptomatic. However, restricted range of motion and pain are common in patients with severe Brooker Grade III or Grade IV ossification. Significant loss of function has been reported in up to 10% of affected patients.
Prophylactic Modalities: Radiation and NSAIDs
Routine prophylaxis is not recommended for all primary THA patients due to associated risks, but targeted prophylaxis is strongly warranted in high-risk populations. The two primary modalities are low-dose radiation and nonsteroidal anti-inflammatory drugs (NSAIDs).
Radiation Therapy:
Preoperative and postoperative radiation regimens utilizing a single dose of 500 cGy (or 700 cGy) have proven highly successful. In multicenter evaluations, failures occurred more commonly in patients treated more than 8 hours preoperatively or more than 72 hours postoperatively. Preoperative treatment is often preferred as it results in less patient discomfort regarding transport compared to the immediate postoperative period.
Surgical Warning: Radiation exposure must be strictly limited to the soft tissues immediately surrounding the hip joint. Potential biologic ingrowth surfaces of cementless femoral and acetabular components must be appropriately shielded to prevent catastrophic failure of osseointegration.
Hedley et al. and Kennedy et al. reported no clinical evidence of loosening, subsidence, or radiolucent lines around cementless prostheses after appropriately shielded irradiation. However, delayed union or nonunion of a trochanteric osteotomy remains a significant potential complication. Malignant transformation has not been reported with the low dosages currently recommended for prophylaxis.


Pharmacological Prophylaxis (NSAIDs):
NSAIDs, particularly indomethacin, significantly reduce the formation of heterotopic bone. Standard recommended dosages are 75 mg/day (often divided) for up to 6 weeks, although shorter courses of 10 to 14 days have also been reported as successful.
The overall utility of NSAID regimens is frequently limited by medical contraindications (e.g., peptic ulcer disease, renal insufficiency) and patient intolerance. Cella, Salvati, and Sculco noted that up to 37% of patients were unable to complete a full course of indomethacin. Similar to irradiation, NSAIDs have been shown in animal models to diminish bone ingrowth into porous implants; crucially, unlike radiation, there is no method to "shield" the implant from systemic pharmacological effects.

Surgical Excision of Heterotopic Bone
Operative intervention to remove heterotopic bone is rarely indicated because pain is usually not severe, and the excision of established HO is a technically demanding, high-risk procedure.
If surgery is undertaken, an extensile exposure is required. The ectopic bone severely distorts and obscures normal anatomic landmarks, placing the sciatic nerve and femoral vessels at high risk. The abnormal bone does not easily "shell out" of the surrounding soft tissues, and substantial intraoperative blood loss should be anticipated. Excision should be delayed until the bone is fully mature (typically 12 to 18 months postoperatively), confirmed by a normalizing alkaline phosphatase level and cold bone scan. Postoperative prophylaxis with radiation or NSAIDs is mandatory to prevent recurrence. While range of motion reliably improves following excision, patients must be counseled that pain may not be completely alleviated.


VENOUS THROMBOEMBOLISM (VTE)
Thromboembolic disease remains one of the most common and potentially devastating complications arising from total hip arthroplasty. Historically, the 30-day mortality rate from pulmonary embolism (PE) in a massive cohort of 30,714 patients undergoing elective THA at the Mayo Clinic was 0.04%, ranking just behind myocardial infarction and cardiorespiratory arrest.
In early historical reports of THA performed without routine prophylaxis, deep vein thrombosis (DVT) occurred in up to 50% of patients, with fatal pulmonary emboli occurring in 2%.
Risk Factors for Venous Thromboembolic Disease
The pathogenesis of VTE is governed by Virchow’s triad: endothelial injury, venous stasis, and hypercoagulability. Several clinical and hemostatic factors exponentially increase the risk of thromboembolism:
Clinical Risk Factors:
* Advanced age and obesity.
* Prior history of venous thromboembolic disease.
* Prolonged immobility or paralysis.
* Congestive heart failure or recent myocardial infarction.
* Concomitant pelvic, hip, or lower extremity fractures.
Hypercoagulable States:
* Antithrombin III, Protein C, or Protein S deficiency.
* Factor V Leiden mutation.
* Lupus anticoagulant and antiphospholipid antibodies.
* Myeloproliferative disorders.


Anesthesia and Timing of VTE
The choice of anesthesia significantly impacts VTE risk. Spinal and epidural (neuraxial) anesthesia carry a demonstrably lower risk of DVT and PE compared to general anesthesia. Davis et al. demonstrated a 13% incidence of DVT under spinal anesthesia versus a 27% incidence under general anesthesia, likely due to sympathetic blockade increasing lower extremity venous flow and decreased systemic hypercoagulability.
Thromboembolism can occur in the venous systems of the pelvis, thigh, and calf, with 80% to 90% of all thromboses occurring in the operated limb. While isolated calf thrombi were previously thought benign, Pellegrini et al. demonstrated that proximal propagation of untreated calf thromboses occurred in 17% of patients, leading to both nonfatal and fatal pulmonary emboli.
With modern rapid-recovery protocols and shorter hospital stays, the majority of thromboembolic events now occur after hospital discharge. The median time to diagnosis of symptomatic DVT is approximately 17 days postoperatively. Johnson et al. noted that fatal PE incidence peaks in the second and third postoperative weeks.


Diagnostic Modalities
The clinical diagnosis of DVT is notoriously unreliable. While classic signs include calf/thigh pain, unilateral swelling, erythema, low-grade fever, and a positive Homan sign, the diagnosis is not clinically apparent in at least 50% of affected patients. Similarly, while PE may present with pleuritic chest pain, tachycardia, and hypoxia, most pulmonary emboli are clinically silent until catastrophic failure occurs.
Adjunctive radiographic testing is therefore mandatory:
* Duplex Ultrasonography: B-mode or duplex Doppler ultrasound is the current standard of care. It is noninvasive, easily repeatable, and boasts a sensitivity of 79%, specificity of 98%, and accuracy of 97% for femoral thromboses. It is, however, less reliable for isolated calf and deep pelvic vein thrombi.
* Venography: Historically considered the gold standard, it is highly sensitive for calf and thigh thrombi but is invasive, costly, and carries risks of contrast allergy and contrast-
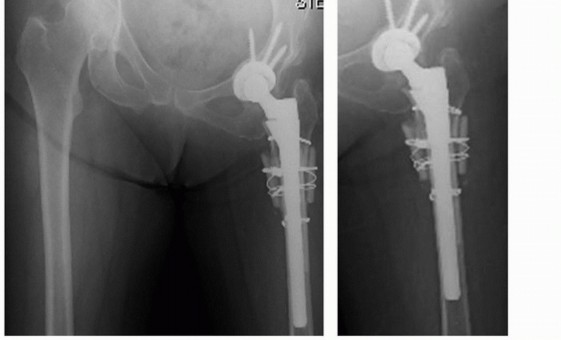
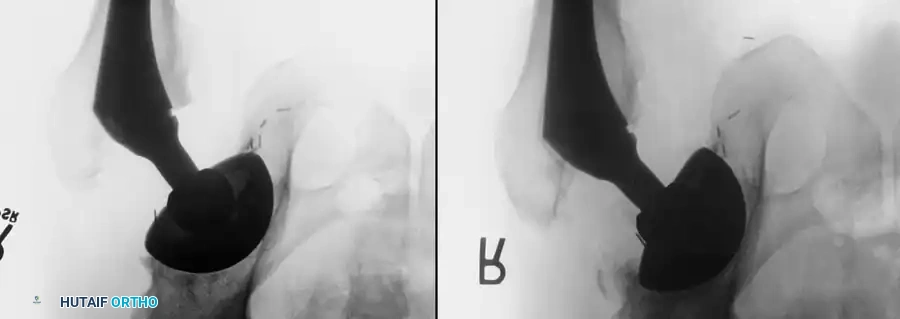
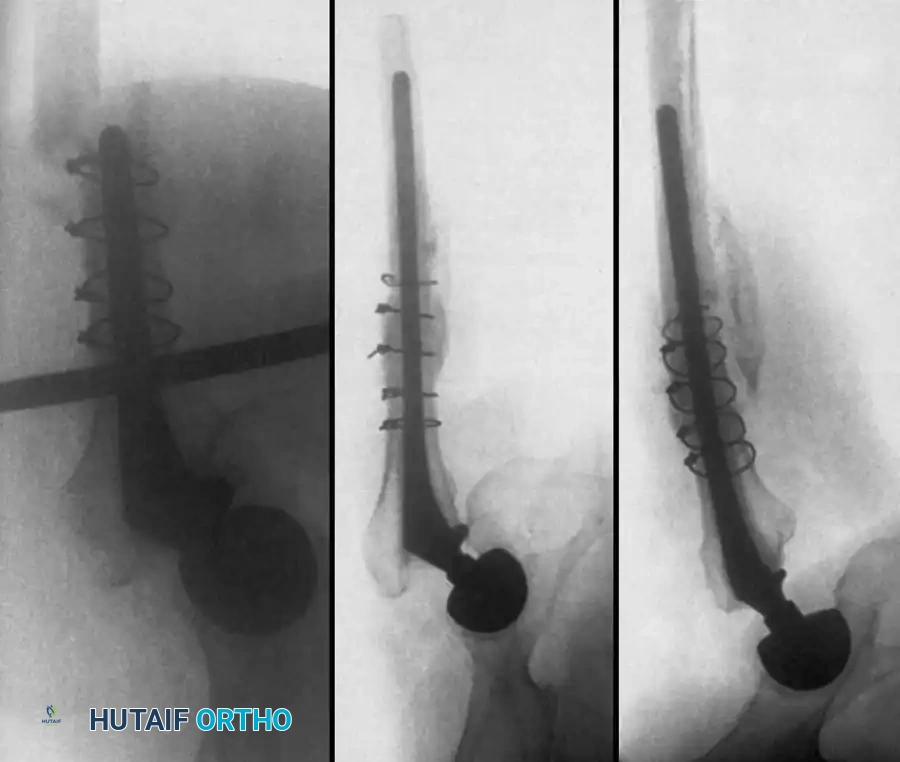
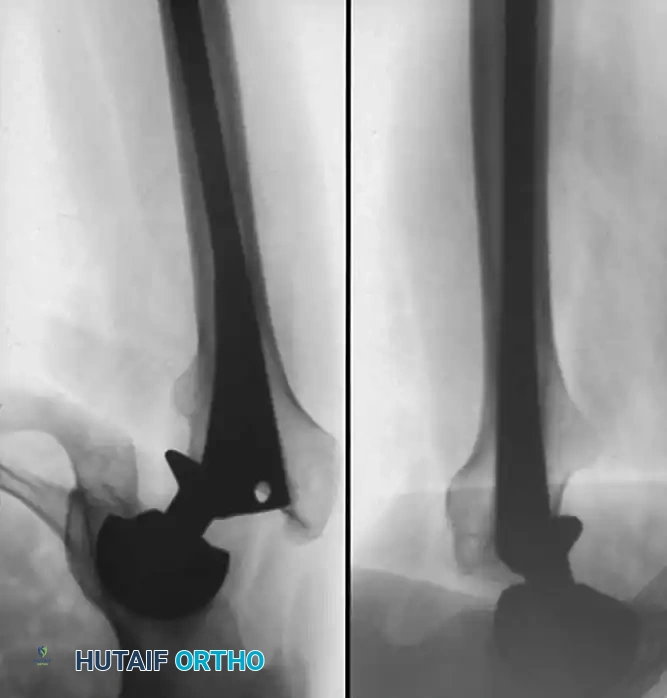
Associated Surgical & Radiographic Imaging

You Might Also Like