Orthopedic Foot And Ank Review | Dr Hutaif Foot & Ankle -...
14 Apr 2026
84 min read
61 Views

Key Takeaway
Looking for accurate information on ORTHOPEDIC MCQS ONLINE 015 FOOT AND ANKLE e? Lisfranc injuries are midfoot ligament disruptions, often missed initially. The Lisfranc ligament extends from the second metatarsal to the medial cuneiform; a "fleck sign" is an avulsion fracture at the second metatarsal base. Treatment for displaced injuries is typically open reduction and internal fixation (ORIF) with rigid screw/plate fixation. To review pubmed pmid view detailed evidence, consult relevant orthopedic literature.
Orthopedic Foot And Ank Review | Dr Hutaif Fo...
00:00
Start Quiz
Question 1High Yield
This injury is best treated with
Explanation
- ORIF with screw and/or plate fixation.
Question 2High Yield
The Lisfranc ligament extends from the
Explanation
- medial cuneiform to the second metatarsal bone.
Question 3High Yield
In Lisfranc injuries, the "fleck sign," when present, represents
Explanation
- a small avulsion fracture of the second metatarsal base.
Question 4High Yield
In the evaluation of Lisfranc injuries, which radiographic studies should routinely be obtained?

Explanation
It is estimated that as many as 20% of Lisfranc injuries are missed on initial radiographic examination. Weight-bearing bilateral radiographs should be performed routinely. CT scan, MRI, and stress radiographs performed under anesthesia may be needed in select cases. The Lisfranc ligament stabilizes the midfoot and consists of the dorsal and plantar oblique ligaments and the strong interosseous ligaments. All 3 extend from the base of the second metatarsal to the medial cuneiform. The “fleck sign" is a small avulsion fracture at the medial base of the second metatarsal, representing an avulsion of the Lisfranc ligament. The current treatment recommendation for displaced Lisfranc subluxations and dislocations is to perform ORIF with rigid fixation using either screws or plates and screws. Kirschner wire fixation may lead to recurrence after pin removal. Closed reduction and casting alone cannot permanently reduce the dislocation.
RECOMMENDED READINGS
Clanton TO, Waldrop III NE. Athletic injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. Vol 2. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014:1531-1687.
Karges DB. Foot trauma. In: Cannada LK, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:631-643.
CLINICAL SITUATION FOR QUESTIONS 5 THROUGH 8
A
B
Figures 5a and 5b are the clinical photograph and AP radiograph of a 55-year-old woman who has a painful right forefoot deformity. There is no history of antecedent trauma. The 1-2 intermetatarsal angle is 17 degrees, and the hallux valgus angle is 35 degrees.
RECOMMENDED READINGS
Clanton TO, Waldrop III NE. Athletic injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. Vol 2. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014:1531-1687.
Karges DB. Foot trauma. In: Cannada LK, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:631-643.
CLINICAL SITUATION FOR QUESTIONS 5 THROUGH 8
A
B
Figures 5a and 5b are the clinical photograph and AP radiograph of a 55-year-old woman who has a painful right forefoot deformity. There is no history of antecedent trauma. The 1-2 intermetatarsal angle is 17 degrees, and the hallux valgus angle is 35 degrees.
Question 5High Yield
The second-toe deformity is most accurately described as
Explanation
- crossover toe.
Question 6High Yield
The patient's painful great-toe deformity is best treated with
Explanation
- proximal metatarsal bunionectomy.
Question 7High Yield
Disruption of which anatomic structure is necessary for the second-toe pathology to occur?
Explanation
- Plantar plate
Question 8High Yield
On the morning of surgery the patient reports in the preop area that she has experienced skin breakdown over the second toe for 10 days. The extensor tendon is disrupted with an exposed proximal interphalangeal joint. She has been applying antibiotic ointment to the wound and denies fever or chills. What is the best plan of care?
Explanation
The clinical photograph shows a hallux valgus and a crossover toe deformity. The plantar plate must be damaged for a crossover toe deformity to develop. A moderately severe hallux valgus deformity without arthritic change is best treated with a bunionectomy with a proximal metatarsal osteotomy. The surgeon must assume that the open joint is at least colonized and at significant risk for postsurgical infection; consequently, it is best to cancel elective surgery, and surgical debridement of soft tissue and bone with deep cultures is recommended.
RECOMMENDED READINGS
[Kaz AJ, Coughlin MJ. Crossover second toe: demographics, etiology, and radiographic assessment. Foot Ankle Int. 2007 Dec;28(12):1223-37. doi: 10.3113/FAI.2007.1223. PubMed PMID: 18173985. ](http://www.ncbi.nlm.nih.gov/pubmed/18173985)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18173985)
[Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantar plate and surgical reconstruction techniques on static stability of lesser metatarsophalangeal joints: a biomechanical study. Foot Ankle Int. 2013 Oct;34(10):1436-42. doi: 10.1177/ 1071100713491728. Epub 2013 Jun 17. PubMed PMID: 23774466. ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23774466)
[Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. ](http://www.ncbi.nlm.nih.gov/pubmed/2613128)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2613128)
RECOMMENDED READINGS
[Kaz AJ, Coughlin MJ. Crossover second toe: demographics, etiology, and radiographic assessment. Foot Ankle Int. 2007 Dec;28(12):1223-37. doi: 10.3113/FAI.2007.1223. PubMed PMID: 18173985. ](http://www.ncbi.nlm.nih.gov/pubmed/18173985)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18173985)
[Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantar plate and surgical reconstruction techniques on static stability of lesser metatarsophalangeal joints: a biomechanical study. Foot Ankle Int. 2013 Oct;34(10):1436-42. doi: 10.1177/ 1071100713491728. Epub 2013 Jun 17. PubMed PMID: 23774466. ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23774466)
[Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. ](http://www.ncbi.nlm.nih.gov/pubmed/2613128)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2613128)
Question 9High Yield
Figure 9 is the radiograph of a 24-year-old amateur marathon runner who has ankle pain. She previously sustained a metatarsal stress fracture. In addition to asking about her training routine and the type of footwear she uses, the orthopaedic surgeon should inquire about this patient's history of nutrition and

Explanation
Several studies have reported an increased incidence of stress fractures in female athletes, including fractures of the foot and ankle in runners. The
female athlete triad describes a condition involving decreased bone density, anorexia, and amenorrhea. In addition to asking about this woman's exercise routine, the orthopaedic surgeon should obtain a comprehensive menstrual and dietary history in the context of multiple stress fractures. A review of genetics, rheumatology, and cardiovascular disorders is less likely to generate an etiology.
RECOMMENDED READINGS
Kasser JR, ed. Orthopaedic Knowledge Update 5: Home Study Syllabus. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1996:96-99.
Arendt EA. Osteoporosis in the athletic female: Amenorrhea and amenorrheic osteoporosis. In: Pearl AJ, ed. AOSSM: The Athletic Female. Champaign, IL: Human Kinetics; 1993:41-59. Brukner PD, Khan KM. Clinical Sports Medicine. Sydney: McGraw-Hill; 1991:17.
RESPONSES FOR QUESTIONS 10 THROUGH 13
1. Ankle replacement
2. Ankle fusion
3. Tibiotalocalcaneal fusion
4. Total contact cast
5. Intra-articular steroid injection
Match the appropriate treatment listed above with the patient scenario described below.
female athlete triad describes a condition involving decreased bone density, anorexia, and amenorrhea. In addition to asking about this woman's exercise routine, the orthopaedic surgeon should obtain a comprehensive menstrual and dietary history in the context of multiple stress fractures. A review of genetics, rheumatology, and cardiovascular disorders is less likely to generate an etiology.
RECOMMENDED READINGS
Kasser JR, ed. Orthopaedic Knowledge Update 5: Home Study Syllabus. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1996:96-99.
Arendt EA. Osteoporosis in the athletic female: Amenorrhea and amenorrheic osteoporosis. In: Pearl AJ, ed. AOSSM: The Athletic Female. Champaign, IL: Human Kinetics; 1993:41-59. Brukner PD, Khan KM. Clinical Sports Medicine. Sydney: McGraw-Hill; 1991:17.
RESPONSES FOR QUESTIONS 10 THROUGH 13
1. Ankle replacement
2. Ankle fusion
3. Tibiotalocalcaneal fusion
4. Total contact cast
5. Intra-articular steroid injection
Match the appropriate treatment listed above with the patient scenario described below.
Question 10High Yield
A 28-year-old woman with bone-on-bone ankle arthritis, little deformity, and recalcitrant pain
Explanation
- Ankle fusion
Question 11High Yield
A 56-year-old woman with diabetes, neuropathy, and an unbraceable ankle and hindfoot deformity
Explanation
- Tibiotalocalcaneal fusion
Question 12High Yield
A 72-year-old man with a previous contralateral ankle fusion, rheumatoid arthritis, and 5 degrees of valgus; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
Explanation
- Ankle replacement
Question 13High Yield
A 72-year-old man with diabetic neuropathy and 5 degrees of valgus talar tilt; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
Explanation
Arthritis of the ankle and hindfoot can pose challenges. Depending upon patient age, comorbidities, and alignment, a variety of surgical interventions may be offered. A total ankle replacement may be considered for patients older than 60 years of age who have minimal misalignment and low-demand lifestyles. In all other cases, ankle fusion must be considered. The nonsurgical care of ankle arthritis includes anti-inflammatory medication, intra-articular steroid injections, bracing with customized products such as the Arizona brace, or a molded foot and ankle orthosis.
Patients with diabetes and Charcot arthropathy may be treated nonsurgically with total-contact casting during acute and active or "hot" phases and accommodative shoes during consolidation and stable or "cool" phases. When the patient has recurrent ulcers or major anatomy changes, surgical intervention must be considered. Tibiotalocalcaneal fusion helps to realign the foot and ankle and make it more braceable in the setting of ankle and hindfoot Charcot disease.
RECOMMENDED READINGS
Patients with diabetes and Charcot arthropathy may be treated nonsurgically with total-contact casting during acute and active or "hot" phases and accommodative shoes during consolidation and stable or "cool" phases. When the patient has recurrent ulcers or major anatomy changes, surgical intervention must be considered. Tibiotalocalcaneal fusion helps to realign the foot and ankle and make it more braceable in the setting of ankle and hindfoot Charcot disease.
RECOMMENDED READINGS
Question 14High Yield
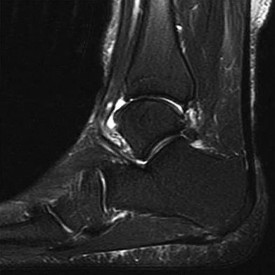
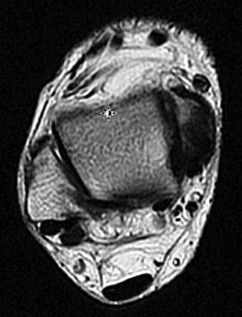
Figure 14 is a sagittal-cut MR image from the hindfoot of a 54-year-old woman who has had plantar heel pain for 3 months. There is no history of trauma. Her pain is worse when she rises and at the end of the day. Upon examination she has localizable tenderness over the plantar medial tubercle of the calcaneus. The Achilles is intact and nontender, and subtalar joint motion is full and painless. A Tinel test result is negative. What is the most likely diagnosis?



Explanation
Plantar fasciitis is inflammation of the plantar fascia at its insertion onto the medial calcaneus. The T2-weighted sagittal MR image reveals thickening of the plantar fascia with no evidence of a calcaneal stress fracture, coalition, or inflammation of the insertion of the Achilles tendon.
RECOMMENDED READINGS
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
[372/. PubMed PMID: 24860133. ](http://www.ncbi.nlm.nih.gov/pubmed/24860133)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860133)
Covey CJ, Mulder MD. Plantar fasciitis: How best to treat? J Fam Pract. 2013 Sep;62(9):466-
[71/. PubMed PMID: 24080555. ](http://www.ncbi.nlm.nih.gov/pubmed/%2024080555)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2024080555)
CLINICAL SITUATION FOR QUESTIONS 15 THROUGH 18
Figures 15a through 15c are the initial injury radiographs of a 32-year-old man who sustained a closed injury to his right lower extremity after a fall from a curb. Initial examination reveals a swollen painful ankle with pain both medially and laterally at the level of the malleoli.
15A
B
C
RECOMMENDED READINGS
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
[372/. PubMed PMID: 24860133. ](http://www.ncbi.nlm.nih.gov/pubmed/24860133)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860133)
Covey CJ, Mulder MD. Plantar fasciitis: How best to treat? J Fam Pract. 2013 Sep;62(9):466-
[71/. PubMed PMID: 24080555. ](http://www.ncbi.nlm.nih.gov/pubmed/%2024080555)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2024080555)
CLINICAL SITUATION FOR QUESTIONS 15 THROUGH 18
Figures 15a through 15c are the initial injury radiographs of a 32-year-old man who sustained a closed injury to his right lower extremity after a fall from a curb. Initial examination reveals a swollen painful ankle with pain both medially and laterally at the level of the malleoli.
15A
B
C
Question 15High Yield
Following surgical stabilization and fixation of the distal fibula, what is the most appropriate next step?
Explanation
- Perform a stress examination of the syndesmosis.
Question 16High Yield
16A
B
C
Figures 16a through 16c are the postsurgical radiographs taken 3 months after surgical stabilization of the fracture and syndesmosis. The patient has no pain and symmetrical range of motion to the contralateral lower extremity. What is the most appropriate next step?
B
C
Figures 16a through 16c are the postsurgical radiographs taken 3 months after surgical stabilization of the fracture and syndesmosis. The patient has no pain and symmetrical range of motion to the contralateral lower extremity. What is the most appropriate next step?



Explanation
- Retention of hardware with progression of activity
Question 17High Yield
One year after surgical fixation of the ankle (Figure 17) the patient has persistent pain within the ankle and wants the hardware removed. He should be counseled that after hardware removal he should expect

Explanation
- no significant change in his symptoms.
Question 18High Yield
Which complication is most common after syndesmotic fixation?
Explanation
The injury radiographs reveal a supination external rotation IV ankle fracture with evidence of medial clear space widening exceeding 4 mm and an increase relative to the superior tibiotalar clear space. This indicates injury to the deltoid ligament and necessitates surgical reduction and fixation to restore and maintain ankle stability. Following stabilization of the fibula, an intraoperative stress examination of the syndesmosis such as an external rotation stress test under fluoroscopy or lateral pull on the fibula (the Cotton test) should be performed to determine the integrity of the syndesmosis. Radiographic evidence of tibiofibular clear space widening, medial clear space widening with external rotation, and lateral displacement of the distal fibula when pulled is consistent with syndesmotic injury. In contrast to the presurgical stress test, once the fibula has been reduced and stabilized lateral talar translation can occur only if the syndesmosis is injured in addition to the deltoid ligament. Failure of the syndesmotic screw without evidence of malalignment of the mortise and a pain-free ankle are not indications for further surgery because these patients have satisfactory outcomes when compared to those who have intact or removed screws. Hardware removal following fibula ORIF is indicated when patients have pain directly related to hardware prominence. Resolution of joint pain or stiffness is not a reliable outcome following hardware removal. Although fibular fracture can occur, this is a rare complication. Malreduction of the syndesmosis is the most common complication following ORIF of the syndesmosis and is improved with direct visualization; however, malreduction still may occur with direct visualization.
RECOMMENDED READINGS
[Manjoo A, Sanders DW, Tieszer C, MacLeod MD. Functional and radiographic results of patients with syndesmotic screw fixation: implications for screw removal. J Orthop Trauma. 2010 Jan;24(1):2-6. doi: 10.1097/BOT.0b013e3181a9f7a5. PubMed PMID: 20035170. ](http://www.ncbi.nlm.nih.gov/pubmed/20035170)[View](http://www.ncbi.nlm.nih.gov/pubmed/20035170)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20035170)
[Jenkinson RJ, Sanders DW, Macleod MD, Domonkos A, Lydestadt J. Intraoperative diagnosis of syndesmosis injuries in external rotation ankle fractures. J Orthop Trauma. 2005 Oct;19(9):604-9. PubMed PMID: 16247304. ](http://www.ncbi.nlm.nih.gov/pubmed/16247304)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16247304)
[Stark E, Tornetta P 3rd, Creevy WR. Syndesmotic instability in Weber B ankle fractures: a clinical evaluation. J Orthop Trauma. 2007 Oct;21(9):643-6. PubMed PMID: 17921840. ](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[View](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17921840)
[Brown OL, Dirschl DR, Obremskey WT. Incidence of hardware-related pain and its effect on functional outcomes after open reduction and internal fixation of ankle fractures. J Orthop Trauma. 2001 May;15(4):271-4. PubMed PMID: 11371792. ](http://www.ncbi.nlm.nih.gov/pubmed/11371792)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11371792)
RECOMMENDED READINGS
[Manjoo A, Sanders DW, Tieszer C, MacLeod MD. Functional and radiographic results of patients with syndesmotic screw fixation: implications for screw removal. J Orthop Trauma. 2010 Jan;24(1):2-6. doi: 10.1097/BOT.0b013e3181a9f7a5. PubMed PMID: 20035170. ](http://www.ncbi.nlm.nih.gov/pubmed/20035170)[View](http://www.ncbi.nlm.nih.gov/pubmed/20035170)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20035170)
[Jenkinson RJ, Sanders DW, Macleod MD, Domonkos A, Lydestadt J. Intraoperative diagnosis of syndesmosis injuries in external rotation ankle fractures. J Orthop Trauma. 2005 Oct;19(9):604-9. PubMed PMID: 16247304. ](http://www.ncbi.nlm.nih.gov/pubmed/16247304)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16247304)
[Stark E, Tornetta P 3rd, Creevy WR. Syndesmotic instability in Weber B ankle fractures: a clinical evaluation. J Orthop Trauma. 2007 Oct;21(9):643-6. PubMed PMID: 17921840. ](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[View](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17921840)
[Brown OL, Dirschl DR, Obremskey WT. Incidence of hardware-related pain and its effect on functional outcomes after open reduction and internal fixation of ankle fractures. J Orthop Trauma. 2001 May;15(4):271-4. PubMed PMID: 11371792. ](http://www.ncbi.nlm.nih.gov/pubmed/11371792)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11371792)
Question 19High Yield
Figure 19 is the clinical photograph of a 54-year-old man who underwent a total ankle replacement (TAR). Three weeks after surgery he has increasing pain and a deep wound as seen in the photograph. What is the best next step?

Explanation
The patient is 3 weeks out from TAR. The wound is erythematous, and the tendon is visible. At 3 weeks this is an acute wound breakdown. The preferred treatment is a return to the operating room, an exchange of the polyethylene because the wound appears deep enough to go down to the joint, and a flap for coverage. Removal of the total ankle and placement of an antibiotic spacer should be considered in the settings of subacute (6 weeks postop) or chronic infection following TAR. A below-the-knee amputation may be considered with a failed salvage or a chronically infected TAR. Conversion to a fusion may be considered in situations in which the wound bed is not infected. In this case, there is concern for ongoing active infection, and an intercalary allograft is not appropriate.
RECOMMENDED READINGS
Cho EH, Garcia R, Pien I, Thomas S, Levin LS, Hollenbeck ST. An algorithmic approach for managing orthopaedic surgical wounds of the foot and ankle. Clin Orthop Relat Res. 2014 Jun;472(6):1921-9. doi: 10.1007/s11999-014-3536-7. Epub 2014 Feb 28. PubMed PMID:
[24577615.](http://www.ncbi.nlm.nih.gov/pubmed/24577615)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24577615)
Gadd RJ, Barwick TW, Paling E, Davies MB, Blundell CM. Assessment of a three-grade classification of complications in total ankle replacement. Foot Ankle Int. 2014 May;35(5):434-7. doi: 10.1177/1071100714524549. Epub 2014 Feb 14. PubMed PMID:
[24532698.](http://www.ncbi.nlm.nih.gov/pubmed/24532698)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24532698)
RECOMMENDED READINGS
Cho EH, Garcia R, Pien I, Thomas S, Levin LS, Hollenbeck ST. An algorithmic approach for managing orthopaedic surgical wounds of the foot and ankle. Clin Orthop Relat Res. 2014 Jun;472(6):1921-9. doi: 10.1007/s11999-014-3536-7. Epub 2014 Feb 28. PubMed PMID:
[24577615.](http://www.ncbi.nlm.nih.gov/pubmed/24577615)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24577615)
Gadd RJ, Barwick TW, Paling E, Davies MB, Blundell CM. Assessment of a three-grade classification of complications in total ankle replacement. Foot Ankle Int. 2014 May;35(5):434-7. doi: 10.1177/1071100714524549. Epub 2014 Feb 14. PubMed PMID:
[24532698.](http://www.ncbi.nlm.nih.gov/pubmed/24532698)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24532698)
Question 20High Yield
Figures 20a and 20b are the radiographs of a 56-year-old woman who runs a horse farm. She has a 2-year history of increasing ankle pain and swelling without previous treatment. Which treatment is most appropriate at this time?


Explanation
This patient has end-stage ankle arthritis. A short course of NSAIDs may provide pain and inflammation relief. Bracing with either an ankle-foot orthosis or Arizona brace can reduce pain by offloading the ankle joint. Ankle fusion is a reliable procedure for treatment of end-stage ankle arthritis and is especially recommended for active people after it is determined that nonsurgical measures no longer provide adequate relief. Arthroscopic debridement and cheilectomy may be indicated for bony impingement and mild arthritis with little articular cartilage loss. The long-term results of ankle distraction arthroplasty are not yet well defined but likewise would be reserved for scenarios in which nonsurgical measures no longer provide adequate relief. The patient must be able to wear a thin-wire external fixator for 3 months.
RECOMMENDED READINGS
Abidi NA, Neufeld SK, Brage ME, Reese KA, Sabharwal S, Paley, D. Ankle arthritis. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:159-193.
Saltzman CL: Ankle arthritis, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle. Philadelphia, PA, Mosby Elsevier, 2007, vol 1, pp 929-932.
RECOMMENDED READINGS
Abidi NA, Neufeld SK, Brage ME, Reese KA, Sabharwal S, Paley, D. Ankle arthritis. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:159-193.
Saltzman CL: Ankle arthritis, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle. Philadelphia, PA, Mosby Elsevier, 2007, vol 1, pp 929-932.
Question 21High Yield
Figure 21 is the intraoperative fluoroscopic image of a 40-year-old man who felt a pop during a twisting injury to his right ankle. He underwent open reduction and internal fixation (ORIF) of a bimalleolar ankle fracture. During the surgery the medial and lateral malleoli fractures were reduced and rigidly was internally fixed. Following fracture fixation, which additional test is recommended to ensure mortise stability?


Explanation
Following ORIF of a known osseous injury, stress testing of the syndesmosis is recommended, especially for pronation-external rotation injuries. The Cotton test applies a laterally directed force to the fibula to assess for widening of the distal tibiofibular joint space. A positive Cotton test result indicates that syndesmotic stabilization is indicated. The Thompson test is used to determine Achilles tendon integrity. The squeeze test is a clinical, not intraoperative, assessment of syndesmotic injury. The anterior drawer test assesses the integrity of the anterior talofibular ligament.
RECOMMENDED READINGS
[Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. ](http://www.ncbi.nlm.nih.gov/pubmed/17548882)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17548882)
Pakarinen H, Flinkkilä T, Ohtonen P, Hyvönen P, Lakovaara M, Leppilahti J, Ristiniemi J. Intraoperative assessment of the stability of the distal tibiofibular joint in supination-external rotation injuries of the ankle: sensitivity, specificity, and reliability of two clinical tests. J Bone Joint Surg Am. 2011 Nov 16;93(22):2057-61. doi: 10.2106/JBJS.J.01287. PubMed PMID:
[22262376.](http://www.ncbi.nlm.nih.gov/pubmed/22262376)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22262376)
CLINICAL SITUATION FOR QUESTIONS 22 THROUGH 25
Figure 22 is a lateral radiograph of a 56-year-old woman who arrives at the emergency department with a midfoot injury that occurred 4 weeks ago. Her
medical history is positive for diabetes mellitus, hypertension, and dialysis-dependent chronic renal failure. She is a household ambulator. Her midfoot is red, swollen, and deformed. The redness decreases with elevation. Her white blood cell count is 5600/µL (reference range [rr], 4500-11000/µL) and her erythrocyte sedimentation rate is 15 mm/h (rr, 0-20 mm/h).
RECOMMENDED READINGS
[Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. ](http://www.ncbi.nlm.nih.gov/pubmed/17548882)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17548882)
Pakarinen H, Flinkkilä T, Ohtonen P, Hyvönen P, Lakovaara M, Leppilahti J, Ristiniemi J. Intraoperative assessment of the stability of the distal tibiofibular joint in supination-external rotation injuries of the ankle: sensitivity, specificity, and reliability of two clinical tests. J Bone Joint Surg Am. 2011 Nov 16;93(22):2057-61. doi: 10.2106/JBJS.J.01287. PubMed PMID:
[22262376.](http://www.ncbi.nlm.nih.gov/pubmed/22262376)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22262376)
CLINICAL SITUATION FOR QUESTIONS 22 THROUGH 25
Figure 22 is a lateral radiograph of a 56-year-old woman who arrives at the emergency department with a midfoot injury that occurred 4 weeks ago. Her
medical history is positive for diabetes mellitus, hypertension, and dialysis-dependent chronic renal failure. She is a household ambulator. Her midfoot is red, swollen, and deformed. The redness decreases with elevation. Her white blood cell count is 5600/µL (reference range [rr], 4500-11000/µL) and her erythrocyte sedimentation rate is 15 mm/h (rr, 0-20 mm/h).
Question 22High Yield
What is the most appropriate diagnosis?
Explanation
- Charcot foot
Question 23High Yield
What is the most appropriate treatment?
Explanation
- Total-contact casting
Question 24High Yield
Glucose control assessment is best achieved by ordering which blood test?
Explanation
- Hemoglobin A1C
Question 25High Yield
The mechanism for the osseous destruction is attributable to
Explanation
This scenario is a classic example of the development of Charcot foot. A red, swollen, deformed foot without ulceration suggests neuroarthropathy. Normal inflammatory marker findings, no history of fever or chills, and radiographs demonstrating bone loss support the diagnosis. Limb elevation with dramatic reduction in erythema is also characteristic of this disease process and does not occur with infection. Total-contact casting is the cornerstone of treatment for acute Charcot disease. Hemoglobin A1C is an indicator of glucose averaged over a 3-month period, providing the most reliable indication of a patient's ongoing glucose control. The pathophysiology of bone destruction is believed to be hypervascularity of bone. Infection and Charcot disease may develop simultaneously, but the combination is rare.
RECOMMENDED READINGS
[Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.](http://www.ncbi.nlm.nih.gov/pubmed/23919113)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23919113)
[Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052. ](http://www.ncbi.nlm.nih.gov/pubmed/16701052)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16701052)
RECOMMENDED READINGS
[Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.](http://www.ncbi.nlm.nih.gov/pubmed/23919113)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23919113)
[Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052. ](http://www.ncbi.nlm.nih.gov/pubmed/16701052)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16701052)
Question 26High Yield
Contracture of which structure causes hammertoe deformity?
Explanation
A patient with a flexible hammertoe deformity has the deformity while standing, but practically no deformity when seated with the foot in equinus. The metatarsophalangeal joint is not involved. The deformity is created by contracture of the flexor digitorum longus tendon.
RECOMMENDED READINGS
[Coughlin MJ. Lesser toe abnormalities. Instr Course Lect. 2003;52:421-44. Review. PubMed PMID: 12690869.](http://www.ncbi.nlm.nih.gov/pubmed/12690869)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690869)
Couglin MJ. Lesser toe deformities. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 1. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:363-464.
RECOMMENDED READINGS
[Coughlin MJ. Lesser toe abnormalities. Instr Course Lect. 2003;52:421-44. Review. PubMed PMID: 12690869.](http://www.ncbi.nlm.nih.gov/pubmed/12690869)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690869)
Couglin MJ. Lesser toe deformities. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 1. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:363-464.
Question 27High Yield
A 10-year-old boy reports heel pain with sporting activities. An examination demonstrates gastrocnemius contracture and tenderness at the calcaneal apophysis. Radiographs are unremarkable. What is the best next step?
Explanation
Sever disease, or calcaneal apophysitis, is best treated with activity modification that includes rest, restriction from sports and running, and Achilles tendon stretching exercises. The diagnosis is clinical (rendering MRI study unnecessary) and the course is usually self-limited, obviating the need for surgery. Occasionally, children with severe symptoms may benefit from a short period of cast or fracture brace immobilization.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
Question 28High Yield
Figure 28 is the radiograph of a 25-year-old soccer player who twisted her left ankle 1 week ago. She has pain and swelling over the anterolateral ankle and there is ecchymosis over the lateral ankle. She has these muscle group findings: anterior tibial tendon-right 5/5, left 5/5; posterior tibial tendon-right
5/5, left 5/5; peroneals-right 5/5, left 4/5; Achilles-right 5/5, left 5/5. What is the best next diagnostic or treatment step?
5/5, left 5/5; peroneals-right 5/5, left 4/5; Achilles-right 5/5, left 5/5. What is the best next diagnostic or treatment step?



Explanation
Thousands of ankle sprains occur in the United States every day. Most affected patients do not have serious sequelae associated with their injury. In this case, a young athlete sprained her ankle. Her only area of tenderness is isolated to the anterior talofibular ligament. She also has associated weakness. The radiograph shows an os subfibulare; this is an entity that she likely was born with. There is no indication of bony pain, and it is too soon to test for instability; consequently, no further imaging is required. Considering the nature of the sprain and her weakness, physical therapy with proprioceptive training and peroneal strengthening would be most beneficial.
RECOMMENDED READINGS
[Lephart SM, Pincivero DM, Giraldo JL, Fu FH. The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med. 1997 Jan-Feb;25(1):130-7. PubMed PMID: 9006708. ](http://www.ncbi.nlm.nih.gov/pubmed/9006708)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9006708)
[McGuine TA, Keene JS. The effect of a balance training program on the risk of ankle sprains in high school athletes. Am J Sports Med. 2006 Jul;34(7):1103-11. Epub 2006 Feb 13. PubMed PMID: 16476915. ](http://www.ncbi.nlm.nih.gov/pubmed/16476915)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16476915)
[Chun TH, Park YS, Sung KS. The effect of ossicle resection in the lateral ligament repair for treatment of chronic lateral ankle instability. Foot Ankle Int. 2013 Aug;34(8):1128-33. doi: 10.1177/1071100713481457. Epub 2013 Mar 7. PubMed PMID: 23471672.](http://www.ncbi.nlm.nih.gov/pubmed/23471672)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/23471672)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23471672)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23471672)
CLINICAL SITUATION FOR QUESTIONS 29 THROUGH 33
Figures 29a and 29b are the weight-bearing radiographs of a 49-year-old woman who has had several months of increasing pain and deformity in her left foot. She points to her plantar medial arch as her area of greatest pain; however, she also has pain just distal to the tip of the distal fibula. Her pain worsens with walking or navigating stairs. Upon examination she has a flexible unilateral pes planus deformity with increased heel valgus and forefoot abduction. She is unable to perform a single heel raise.
29A
B
RECOMMENDED READINGS
[Lephart SM, Pincivero DM, Giraldo JL, Fu FH. The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med. 1997 Jan-Feb;25(1):130-7. PubMed PMID: 9006708. ](http://www.ncbi.nlm.nih.gov/pubmed/9006708)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9006708)
[McGuine TA, Keene JS. The effect of a balance training program on the risk of ankle sprains in high school athletes. Am J Sports Med. 2006 Jul;34(7):1103-11. Epub 2006 Feb 13. PubMed PMID: 16476915. ](http://www.ncbi.nlm.nih.gov/pubmed/16476915)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16476915)
[Chun TH, Park YS, Sung KS. The effect of ossicle resection in the lateral ligament repair for treatment of chronic lateral ankle instability. Foot Ankle Int. 2013 Aug;34(8):1128-33. doi: 10.1177/1071100713481457. Epub 2013 Mar 7. PubMed PMID: 23471672.](http://www.ncbi.nlm.nih.gov/pubmed/23471672)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/23471672)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23471672)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23471672)
CLINICAL SITUATION FOR QUESTIONS 29 THROUGH 33
Figures 29a and 29b are the weight-bearing radiographs of a 49-year-old woman who has had several months of increasing pain and deformity in her left foot. She points to her plantar medial arch as her area of greatest pain; however, she also has pain just distal to the tip of the distal fibula. Her pain worsens with walking or navigating stairs. Upon examination she has a flexible unilateral pes planus deformity with increased heel valgus and forefoot abduction. She is unable to perform a single heel raise.
29A
B
Question 29High Yield
Which primary underlying pathologic finding is causing her symptoms?
Explanation
- Posterior tibial tendon dysfunction
Question 30High Yield
Injury to which ligament is commonly seen in this condition?
Explanation
- Calcaneonavicular (spring)
Question 31High Yield
In addition to physical therapy, what is the best course of treatment at this time?
Explanation
- Ankle-foot orthosis
Question 32High Yield
Which surgical procedure should be considered after 6 months of unsuccessful nonsurgical treatment?
Explanation
- Calcaneal osteotomy with bone graft and flexor digitorum longus tendon transfer
Question 33High Yield
Figure 33 is the preoperative photograph of the patient's forefoot with the heel taken out of valgus. Which procedure will best address this forefoot deformity (which cannot be passively corrected by the examiner)?
33
33


Explanation
The most common cause of acquired adult flatfoot deformity (AAFD) is dysfunction of the posterior tibial tendon. Tearing of the calcaneonavicular (spring) ligament and gastrocnemius contracture results from longer-standing attenuation of the posterior tibial tendon. Tarsal coalitions typically cause rigid flatfoot deformity. The calcaneonavicular ligament comprises superomedial and inferomedial bands. More than 70% of patients with AAFD have tearing of the superomedial band. Tearing of the inferior band is seen less commonly. Deltoid ligament insufficiency can be seen in long-standing valgus foot deformity. Initial treatment should start with ankle-foot orthosis bracing and physical therapy.
The radiographs reveal loss of arch, significant uncoverage of the talar head by the navicular, and lack of significant arthritis. Fusion procedures are not indicated considering the patient's flexible deformity and the absence of hindfoot arthritis. Realignment osteotomy must be combined with flexor digitorum longus tendon transfer to successfully alleviate this patient's symptoms. Lateral column lengthening will correct the forefoot abduction and talonavicular subluxation. A medial sliding osteotomy can achieve additional correction and decompress subfibular impingement. A dorsal opening plantar flexion (Cotton) osteotomy of the medial cuneiform is an adjunct procedure that is needed to balance the foot in cases of residual forefoot varus, as seen in the clinical photograph.
RECOMMENDED READINGS
Pinney SJ, Lin SS. Current concept review: acquired adult flatfoot deformity. [Foot Ankle Int. 2006 Jan;27(1):66-75. Review. PubMed PMID: 16442033. ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16442033)
[Bluman EM, Title CI, Myerson MS. Posterior tibial tendon rupture: a refined classification system. Foot Ankle Clin. 2007 Jun;12(2):233-49, v. Review. PubMed PMID: 17561198. ](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[View](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17561198)
Haddad SL, Mann RA. Flatfoot deformity in adults. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:1007-1085.
The radiographs reveal loss of arch, significant uncoverage of the talar head by the navicular, and lack of significant arthritis. Fusion procedures are not indicated considering the patient's flexible deformity and the absence of hindfoot arthritis. Realignment osteotomy must be combined with flexor digitorum longus tendon transfer to successfully alleviate this patient's symptoms. Lateral column lengthening will correct the forefoot abduction and talonavicular subluxation. A medial sliding osteotomy can achieve additional correction and decompress subfibular impingement. A dorsal opening plantar flexion (Cotton) osteotomy of the medial cuneiform is an adjunct procedure that is needed to balance the foot in cases of residual forefoot varus, as seen in the clinical photograph.
RECOMMENDED READINGS
Pinney SJ, Lin SS. Current concept review: acquired adult flatfoot deformity. [Foot Ankle Int. 2006 Jan;27(1):66-75. Review. PubMed PMID: 16442033. ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16442033)
[Bluman EM, Title CI, Myerson MS. Posterior tibial tendon rupture: a refined classification system. Foot Ankle Clin. 2007 Jun;12(2):233-49, v. Review. PubMed PMID: 17561198. ](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[View](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17561198)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17561198)
Haddad SL, Mann RA. Flatfoot deformity in adults. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:1007-1085.
Question 34High Yield
Which stress fracture location is reported most frequently among ballet dancers?
Explanation
Stress fractures are a frequent overuse injury among professional ballet dancers. The most common location is at the proximal metaphyseal-diaphyseal junction of the second metatarsal. Repetitive stress injuries and fractures of the tibial sesamoid, tarsal navicular, and base of the fifth metatarsal occur among other athletes.
RECOMMENDED READINGS
[O'Malley MJ, Hamilton WG, Munyak J, DeFranco MJ. Stress fractures at the base of the second metatarsal in ballet dancers. Foot Ankle Int. 1996 Feb;17(2):89-94. PubMed PMID: 8919407. ](http://www.ncbi.nlm.nih.gov/pubmed/8919407)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8919407)
[Micheli LJ, Sohn RS, Solomon R. Stress fractures of the second metatarsal involving Lisfranc's joint in ballet dancers. A new overuse injury of the foot. J Bone Joint Surg Am. 1985 Dec;67(9):1372-5. PubMed PMID: 4077907. ](http://www.ncbi.nlm.nih.gov/pubmed/4077907)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4077907)
[Gehrmann RM, Renard RL. Current concepts review: Stress fractures of the foot. Foot Ankle Int. 2006 Sep;27(9):750-7. Review. PubMed PMID: 17038292. ](http://www.ncbi.nlm.nih.gov/pubmed/17038292)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17038292)
RECOMMENDED READINGS
[O'Malley MJ, Hamilton WG, Munyak J, DeFranco MJ. Stress fractures at the base of the second metatarsal in ballet dancers. Foot Ankle Int. 1996 Feb;17(2):89-94. PubMed PMID: 8919407. ](http://www.ncbi.nlm.nih.gov/pubmed/8919407)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8919407)
[Micheli LJ, Sohn RS, Solomon R. Stress fractures of the second metatarsal involving Lisfranc's joint in ballet dancers. A new overuse injury of the foot. J Bone Joint Surg Am. 1985 Dec;67(9):1372-5. PubMed PMID: 4077907. ](http://www.ncbi.nlm.nih.gov/pubmed/4077907)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4077907)
[Gehrmann RM, Renard RL. Current concepts review: Stress fractures of the foot. Foot Ankle Int. 2006 Sep;27(9):750-7. Review. PubMed PMID: 17038292. ](http://www.ncbi.nlm.nih.gov/pubmed/17038292)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17038292)
Question 35High Yield
Figure 35 is the radiograph of a 37-year-old woman who began having right forefoot pain about 4 weeks ago after increasing her daily running mileage. She denies any specific injury. Upon examination she has tenderness over the medial forefoot with mild swelling. In addition to her activity level, what is the primary etiology of the radiograph finding?

Explanation
Stress fractures are the result of physiological bone response to increased stress. Increased stress on bone triggers an increase in remodeling, which begins with resorption of bone at the site of stress. Ongoing stress can overwhelm bone strength, resulting in a fracture. In the foot this most commonly is seen in the second metatarsal at the junction of the middle and distal thirds. Contributing factors to increased loading of the second metatarsal include hallux valgus (decreased hallux loading transfers to the second metatarsal head), hallux rigidus (offloading of the hallux attributable to pain increases second metatarsal loading), and a long second metatarsal (increased duration of contact during push-off in the stance phase).
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
[76/. doi: 10.5435/JAAOS-20-03-167. Review. PubMed PMID: 22382289. ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22382289)
[Donahue SW, Sharkey NA. Strains in the metatarsals during the stance phase of gait: implications for stress fractures. J Bone Joint Surg Am. 1999 Sep;81(9):1236-44. PubMed PMID: 10505520. ](http://www.ncbi.nlm.nih.gov/pubmed/10505520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10505520)
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
[76/. doi: 10.5435/JAAOS-20-03-167. Review. PubMed PMID: 22382289. ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22382289)
[Donahue SW, Sharkey NA. Strains in the metatarsals during the stance phase of gait: implications for stress fractures. J Bone Joint Surg Am. 1999 Sep;81(9):1236-44. PubMed PMID: 10505520. ](http://www.ncbi.nlm.nih.gov/pubmed/10505520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10505520)
Question 36High Yield
Which radiographic abnormality most accurately serves as a predictor of ankle syndesmosis disruption?
Explanation
Normal syndesmotic relationships include a tibiofibular clear space smaller than 6 mm on both AP and mortise views. In a 1989 cadaveric study by Harper and Keller, a tibiofibular clear space exceeding 6 mm on both the AP and mortise views was the most reliable predictor of early syndesmotic widening. Tibiofibular overlap is measured 1 cm proximal to the plafond. Normal values exceed 6 mm or 42% of the width of the fibula on the AP view, or 1 mm on the mortise view. Proximal fibula fracture can occur in isolation without syndesmotic injury, frequently after direct trauma. The medial clear space is the distance between the lateral border of the medial malleolus and the medial border of the talus and is measured at the level of the talar dome. In the mortise view with the ankle in neutral dorsiflexion, the medial clear space should be equal to or smaller than the superior clear space between the talar dome and the tibial plafond. ?A normal medial clear space may be present with syndesmotic injury and consequently lacks sensitivity and specificity.
RECOMMENDED READINGS
[Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. ](http://www.ncbi.nlm.nih.gov/pubmed/17548882)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17548882)
[Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. ](http://www.ncbi.nlm.nih.gov/pubmed/10797219)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10797219)
[Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. ](http://www.ncbi.nlm.nih.gov/pubmed/2613128)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2613128)
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
RECOMMENDED READINGS
[Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. ](http://www.ncbi.nlm.nih.gov/pubmed/17548882)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17548882)
[Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. ](http://www.ncbi.nlm.nih.gov/pubmed/10797219)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10797219)
[Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. ](http://www.ncbi.nlm.nih.gov/pubmed/2613128)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2613128)
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
Question 37High Yield
What is the appropriate treatment at this time?
Explanation
- Begin a structured proprioceptive-based rehabilitation program and use a brace as needed.
Question 38High Yield
38A
B
Three months later this patient has continued swelling and giving-way episodes. Figures 38a and 38b are his stress radiographs. This study indicates laxity in which ligament?
B
Three months later this patient has continued swelling and giving-way episodes. Figures 38a and 38b are his stress radiographs. This study indicates laxity in which ligament?


Explanation
- Anterior talofibular
Question 39High Yield
39A
B
C
D
The continued pain and instability 4 months after injury are likely related to which finding on the presurgical MR images in Figures 39a through 39d?
B
C
D
The continued pain and instability 4 months after injury are likely related to which finding on the presurgical MR images in Figures 39a through 39d?
Explanation
- Osteochondral lesion of the talus
Question 40High Yield
40A
B
Figures 40a and 40b are this patient's intraoperative arthroscopic images. The abnormality seen here illustrates which of the patient's clinical findings?
B
Figures 40a and 40b are this patient's intraoperative arthroscopic images. The abnormality seen here illustrates which of the patient's clinical findings?


Explanation
Ankle sprains are the most common musculoskeletal injury; however, most of these sprains do not progress to chronic instability. Initial injuries are treated with RICE (rest, ice, compression, elevation), range of motion, weight bearing
as tolerated, and proprioceptive therapy. Lace-up ankle braces are most effective during the subacute period after a sprain. Structured physical therapy focused on proprioception is recommended for 6 weeks. Examination findings for ankle ligament instability are unreliable because of associated subtalar joint motion. Casting is not as effective as functional rehabilitation. Stress radiographs are recommended, but a clear pathologic range of measurements is not defined. Generalized ligament laxity can result in false-positive findings of instability; therefore, contralateral stress radiographs are often necessary for comparison. The difference in anterior drawer measurement between both ankles should not exceed 5mm. Likewise, the difference in talar tilt measurement between both ankles should be 5 or fewer degrees. Patients with mechanical symptoms, a joint effusion, or continued pain may have an intra-articular pathology such as a loose body or osteochondral lesion. Ankle instability can exist without ligamentous laxity. Symptoms of chronic instability can result from osteochondral lesions of talus, peroneal tendon pathology, loose bodies, anterior ankle impingement, and fracture nonunions. Although there is not sufficient evidence to recommend arthroscopy prior to all ligament reconstructions, arthroscopy is recommended when other pathology is suspected.
RECOMMENDED READINGS
[Colville MR. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg. 1998 Nov-Dec;6(6):368-77. Review. PubMed PMID: 9826420. ](http://www.ncbi.nlm.nih.gov/pubmed/9826420)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9826420)
[DiGiovanni CW, Brodsky A. Current concepts: lateral ankle instability. Foot Ankle Int. 2006 Oct;27(10):854-66. Review. PubMed PMID: 17054892. ](http://www.ncbi.nlm.nih.gov/pubmed/17054892)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17054892)
[Maffulli N, Ferran NA. Management of acute and chronic ankle instability. J Am Acad Orthop Surg. 2008 Oct;16(10):608-15. Review. PubMed PMID: 18832604. ](http://www.ncbi.nlm.nih.gov/pubmed/18832604)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18832604)
as tolerated, and proprioceptive therapy. Lace-up ankle braces are most effective during the subacute period after a sprain. Structured physical therapy focused on proprioception is recommended for 6 weeks. Examination findings for ankle ligament instability are unreliable because of associated subtalar joint motion. Casting is not as effective as functional rehabilitation. Stress radiographs are recommended, but a clear pathologic range of measurements is not defined. Generalized ligament laxity can result in false-positive findings of instability; therefore, contralateral stress radiographs are often necessary for comparison. The difference in anterior drawer measurement between both ankles should not exceed 5mm. Likewise, the difference in talar tilt measurement between both ankles should be 5 or fewer degrees. Patients with mechanical symptoms, a joint effusion, or continued pain may have an intra-articular pathology such as a loose body or osteochondral lesion. Ankle instability can exist without ligamentous laxity. Symptoms of chronic instability can result from osteochondral lesions of talus, peroneal tendon pathology, loose bodies, anterior ankle impingement, and fracture nonunions. Although there is not sufficient evidence to recommend arthroscopy prior to all ligament reconstructions, arthroscopy is recommended when other pathology is suspected.
RECOMMENDED READINGS
[Colville MR. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg. 1998 Nov-Dec;6(6):368-77. Review. PubMed PMID: 9826420. ](http://www.ncbi.nlm.nih.gov/pubmed/9826420)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9826420)
[DiGiovanni CW, Brodsky A. Current concepts: lateral ankle instability. Foot Ankle Int. 2006 Oct;27(10):854-66. Review. PubMed PMID: 17054892. ](http://www.ncbi.nlm.nih.gov/pubmed/17054892)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17054892)
[Maffulli N, Ferran NA. Management of acute and chronic ankle instability. J Am Acad Orthop Surg. 2008 Oct;16(10):608-15. Review. PubMed PMID: 18832604. ](http://www.ncbi.nlm.nih.gov/pubmed/18832604)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18832604)
Question 41High Yield
Which nerve is not included in a standard popliteal nerve block?


Explanation
A standard popliteal nerve block is performed with the patient prone. The injection aims for the area at, or close to, the peroneal and tibial nerves. The sural nerve branches distal to the injection site, so this nerve and the superficial peroneal, deep peroneal, and tibial nerves are covered with the injection. The saphenous nerve is in an anteromedial location at knee level and is not close enough to the area covered by the posterior injection to be included in the analgesic effect.
RECOMMENDED READINGS
[Varitimidis SE, Venouziou AI, Dailiana ZH, Christou D, Dimitroulias A, Malizos KN. Triple nerve block at the knee for foot and ankle surgery performed by the surgeon: difficulties and efficiency. Foot Ankle Int. 2009 Sep;30(9):854-9. PubMed PMID: 19755069. ](http://www.ncbi.nlm.nih.gov/pubmed/19755069)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/19755069)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19755069)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19755069)
[Hromádka R, Barták V, Popelka S, Jahoda D, Pokorný D, Sosna A. [Regional anaesthesia of the foot achieved from two cutaneous points of injection: an anatomical study]. Acta Chir Orthop Traumatol Cech. 2009 Apr;76(2):104-9. Czech. PubMed PMID: 19439129. ](http://www.ncbi.nlm.nih.gov/pubmed/19439129)[View](http://www.ncbi.nlm.nih.gov/pubmed/19439129)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19439129)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19439129)
[Tran D, Clemente A, Finlayson RJ. A review of approaches and techniques for lower extremity nerve blocks. Can J Anaesth. 2007 Nov;54(11):922-34. Review. PubMed PMID: 17975239. ](http://www.ncbi.nlm.nih.gov/pubmed/17975239)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17975239)
CLINICAL SITUATION FOR QUESTIONS 42 THROUGH 44
42A
B
Figures 42a and 42b are the radiographs of a 32-year-old man with an accessory navicular, pes planovalgus deformity, and an associated gastrocnemius contracture. He has been treated with custom orthotics and a physical therapy program for several years and has progressed to stage II posterior tibial tendon dysfunction (PTTD). This patient is now interested in surgery. Tendon reconstruction with bony procedure to correct alignment, medializing calcaneal osteotomy with lateral column lengthening, and a subtalar arthroereisis implant are discussed with the patient.
RECOMMENDED READINGS
[Varitimidis SE, Venouziou AI, Dailiana ZH, Christou D, Dimitroulias A, Malizos KN. Triple nerve block at the knee for foot and ankle surgery performed by the surgeon: difficulties and efficiency. Foot Ankle Int. 2009 Sep;30(9):854-9. PubMed PMID: 19755069. ](http://www.ncbi.nlm.nih.gov/pubmed/19755069)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/19755069)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19755069)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19755069)
[Hromádka R, Barták V, Popelka S, Jahoda D, Pokorný D, Sosna A. [Regional anaesthesia of the foot achieved from two cutaneous points of injection: an anatomical study]. Acta Chir Orthop Traumatol Cech. 2009 Apr;76(2):104-9. Czech. PubMed PMID: 19439129. ](http://www.ncbi.nlm.nih.gov/pubmed/19439129)[View](http://www.ncbi.nlm.nih.gov/pubmed/19439129)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19439129)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19439129)
[Tran D, Clemente A, Finlayson RJ. A review of approaches and techniques for lower extremity nerve blocks. Can J Anaesth. 2007 Nov;54(11):922-34. Review. PubMed PMID: 17975239. ](http://www.ncbi.nlm.nih.gov/pubmed/17975239)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17975239)
CLINICAL SITUATION FOR QUESTIONS 42 THROUGH 44
42A
B
Figures 42a and 42b are the radiographs of a 32-year-old man with an accessory navicular, pes planovalgus deformity, and an associated gastrocnemius contracture. He has been treated with custom orthotics and a physical therapy program for several years and has progressed to stage II posterior tibial tendon dysfunction (PTTD). This patient is now interested in surgery. Tendon reconstruction with bony procedure to correct alignment, medializing calcaneal osteotomy with lateral column lengthening, and a subtalar arthroereisis implant are discussed with the patient.
Question 42High Yield
Which complication associated with subtalar arthroereisis devices for treatment of flexible flatfoot deformity is most common?
Explanation
- Persistent pain in the sinus tarsi
Question 43High Yield
43A
B
Figures 43a and 43b are the postsurgical radiographs. Which tendon transfer is most appropriate for this patient's treatment?
B
Figures 43a and 43b are the postsurgical radiographs. Which tendon transfer is most appropriate for this patient's treatment?


Explanation
- FDL
Question 44High Yield
Os naviculare is present in which percentage of normal feet?
Explanation
Accessory navicular is found in 10% to 14% of normal feet, is generally asymptomatic, and involves 3 radiographic types. Type I represents a small ossicle embedded within the posterior tibial tendon, type II is larger with a synchondrosis, and type III is fused to the navicular tuberosity. Approximately 50% of patients with symptoms have flexible flatfoot; however, os naviculare is not directly associated with pes planovalgus deformity.
Subtalar arthroereisis describes the use of a sinus tarsi plug or implant to restrict eversion of the subtalar joint. This surgical procedure has been used in combination with tendon reconstruction for treatment of flexible flatfoot deformity. Known complications of subtalar arthroereisis include persistent sinus tarsi pain, foreign body reaction, implant failure, and osteonecrosis of the talus.
The FDL tendon travels within the same compartment adjacent to the posterior tibial tendon and is the most commonly used tendon transfer for treatment of stage II PTTD (strength characteristics are similar). The plantaris has inferior tendon strength to the FDL, and the peroneus longus travels in a different compartment than the FDL.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Alvarez RG, Price J, Marini A, Turner NS, Kitaoka HB. Adult acquired flatfoot deformity and posterior tibial tendon dysfunction. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:215-229.
[Pinney SJ, Lin SS. Current concept review: acquired adult flatfoot deformity. Foot Ankle Int. 2006 Jan;27(1):66-75. Review. PubMed PMID: 16442033. ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16442033)
[Viladot R, Pons M, Alvarez F, Omaña J. Subtalar arthroereisis for posterior tibial tendon dysfunction: a preliminary report. Foot Ankle Int. 2003 Aug;24(8):600-6. PubMed PMID: 12956565. ](http://www.ncbi.nlm.nih.gov/pubmed/12956565)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12956565)
Subtalar arthroereisis describes the use of a sinus tarsi plug or implant to restrict eversion of the subtalar joint. This surgical procedure has been used in combination with tendon reconstruction for treatment of flexible flatfoot deformity. Known complications of subtalar arthroereisis include persistent sinus tarsi pain, foreign body reaction, implant failure, and osteonecrosis of the talus.
The FDL tendon travels within the same compartment adjacent to the posterior tibial tendon and is the most commonly used tendon transfer for treatment of stage II PTTD (strength characteristics are similar). The plantaris has inferior tendon strength to the FDL, and the peroneus longus travels in a different compartment than the FDL.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Alvarez RG, Price J, Marini A, Turner NS, Kitaoka HB. Adult acquired flatfoot deformity and posterior tibial tendon dysfunction. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:215-229.
[Pinney SJ, Lin SS. Current concept review: acquired adult flatfoot deformity. Foot Ankle Int. 2006 Jan;27(1):66-75. Review. PubMed PMID: 16442033. ](http://www.ncbi.nlm.nih.gov/pubmed/16442033)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16442033)
[Viladot R, Pons M, Alvarez F, Omaña J. Subtalar arthroereisis for posterior tibial tendon dysfunction: a preliminary report. Foot Ankle Int. 2003 Aug;24(8):600-6. PubMed PMID: 12956565. ](http://www.ncbi.nlm.nih.gov/pubmed/12956565)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12956565)
Question 45High Yield
A
B C
D E
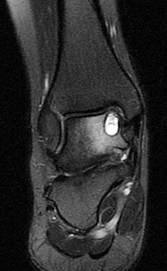
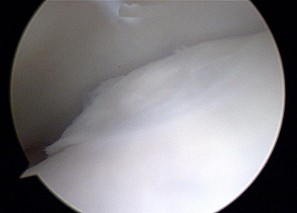
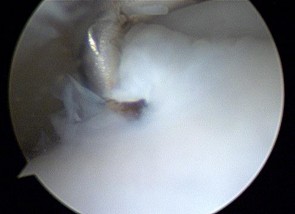
Figures 45a through 45c are the MR images of a 22-year-old woman who has had 6 months of ankle pain related to activities of daily living. She recently completed a course of cast immobilization and protected weight bearing without symptom resolution. Figures 45d and 45e are the intraoperative arthroscopy images after minimal probing. What is the most appropriate treatment?
B C
D E
Figures 45a through 45c are the MR images of a 22-year-old woman who has had 6 months of ankle pain related to activities of daily living. She recently completed a course of cast immobilization and protected weight bearing without symptom resolution. Figures 45d and 45e are the intraoperative arthroscopy images after minimal probing. What is the most appropriate treatment?


Explanation
The MR images reveal a large cystic medial talar dome osteochondral lesion (OCL) in a patient who has failed nonsurgical treatment. Ankle fusion is inappropriate because the patient has an otherwise normal ankle. Arthroscopic debridement and drilling are appropriate for smaller (< 1.5 cm sq) noncystic lesions. Retrograde drilling and bone grafting is an option in the treatment of cystic OCL if the cartilage surface is intact; however, intraoperative arthroscopy images show that this patient's cartilage surface is unstable. Osteochondral allografts and autografts are effective in the treatment of large cystic talar dome OCLs but are not appropriate for the initial surgical treatment of smaller lesions like this one.
RECOMMENDED READINGS
Hannon CP, Smyth NA, Murawski CD, Savage-Elliott I, Deyer TW, Calder JD, Kennedy JG. Osteochondral lesions of the talus: aspects of current management. Bone Joint J. 2014 Feb;96-B(2):164-71. doi: 10.1302/0301-620X.96B2.31637. Review. PubMed PMID:
[24493179/. ](http://www.ncbi.nlm.nih.gov/pubmed/24493179)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24493179)
[Easley ME, Latt LD, Santangelo JR, Merian-Genast M, Nunley JA 2nd. Osteochondral lesions of the talus. J Am Acad Orthop Surg. 2010 Oct;18(10):616-30. Review. PubMed PMID: 20889951. ](http://www.ncbi.nlm.nih.gov/pubmed/20889951)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20889951)
RECOMMENDED READINGS
Hannon CP, Smyth NA, Murawski CD, Savage-Elliott I, Deyer TW, Calder JD, Kennedy JG. Osteochondral lesions of the talus: aspects of current management. Bone Joint J. 2014 Feb;96-B(2):164-71. doi: 10.1302/0301-620X.96B2.31637. Review. PubMed PMID:
[24493179/. ](http://www.ncbi.nlm.nih.gov/pubmed/24493179)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24493179)
[Easley ME, Latt LD, Santangelo JR, Merian-Genast M, Nunley JA 2nd. Osteochondral lesions of the talus. J Am Acad Orthop Surg. 2010 Oct;18(10):616-30. Review. PubMed PMID: 20889951. ](http://www.ncbi.nlm.nih.gov/pubmed/20889951)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20889951)
Question 46High Yield
A 32-year-old woman has had progressive left foot pain over the first metatarsophalangeal (MTP) joint. Footwear is becoming problematic. There is full range of motion of the first MTP with medial eminence pain. Her weightbearing radiograph reveals a hallux valgus angle (HVA) of 35 degrees and a 1-2 intermetatarsal angle (IMA) of 10 degrees. What is the best next step?
Explanation
Patients with painful progressive hallux valgus are surgical candidates. Presurgical evaluation includes radiographic examination. The IMA between the first and second metatarsals as well as the HVA must be measured. If the IMA is smaller than 15 degrees and the HVA is smaller than 35 degrees, a distal osteotomy is preferred. Distal soft-tissue reconstruction is only useful for IMAs smaller than 11 degrees and HVAs smaller than 25 degrees. Proximal osteotomies and the Lapidus bunionectomy are reserved for larger hallux valgus deformities with IMAs exceeding 15 degrees and HVAs exceeding 35 degrees.
RECOMMENDED READINGS
Pentikainen I, Ojala R, Ohtonen P, Piippo J, Leppilahti J. Distal Chevron Osteotomy: Preoperative Radiological Factors Contributing to Long-Term Radiological Recurrence of Hallux
[Valgus. Foot Ankle Int. 2014 Sep 5. pii: 1071100714548703. [Epub ahead of print] PubMed PMID: 25192724. ](http://www.ncbi.nlm.nih.gov/pubmed/25192724)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25192724)
Fakoor M, Sarafan N, Mohammadhoseini P, Khorami M, Arti H, Mosavi S, Aghaeeaghdam A. Comparison of Clinical Outcomes of Scarf and Chevron Osteotomies and the McBride Procedure in the Treatment of Hallux Valgus Deformity. Arch Bone Jt Surg. 2014 Mar;2(1):31-
[6/. Epub 2014 Mar 15. PubMed PMID: 25207310. ](http://www.ncbi.nlm.nih.gov/pubmed/25207310)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25207310)
[Park YB, Lee KB, Kim SK, Seon JK, Lee JY. Comparison of distal soft-tissue procedures combined with a distal chevron osteotomy for moderate to severe hallux valgus: first web-space versus transarticular approach. J Bone Joint Surg Am. 2013 Nov 6;95(21):e158. doi: 10.2106/JBJS.L.01017. PubMed PMID: 24196470. ](http://www.ncbi.nlm.nih.gov/pubmed/24196470)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24196470)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24196470)
RESPONSES FOR QUESTION 47 THROUGH 50
1. Observation
2. Arizona brace
3. Medial arch support
4. Casting
5. Hindfoot fusion
Select the most appropriate initial treatment from the list above to address each of the conditions described below.
RECOMMENDED READINGS
Pentikainen I, Ojala R, Ohtonen P, Piippo J, Leppilahti J. Distal Chevron Osteotomy: Preoperative Radiological Factors Contributing to Long-Term Radiological Recurrence of Hallux
[Valgus. Foot Ankle Int. 2014 Sep 5. pii: 1071100714548703. [Epub ahead of print] PubMed PMID: 25192724. ](http://www.ncbi.nlm.nih.gov/pubmed/25192724)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25192724)
Fakoor M, Sarafan N, Mohammadhoseini P, Khorami M, Arti H, Mosavi S, Aghaeeaghdam A. Comparison of Clinical Outcomes of Scarf and Chevron Osteotomies and the McBride Procedure in the Treatment of Hallux Valgus Deformity. Arch Bone Jt Surg. 2014 Mar;2(1):31-
[6/. Epub 2014 Mar 15. PubMed PMID: 25207310. ](http://www.ncbi.nlm.nih.gov/pubmed/25207310)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25207310)
[Park YB, Lee KB, Kim SK, Seon JK, Lee JY. Comparison of distal soft-tissue procedures combined with a distal chevron osteotomy for moderate to severe hallux valgus: first web-space versus transarticular approach. J Bone Joint Surg Am. 2013 Nov 6;95(21):e158. doi: 10.2106/JBJS.L.01017. PubMed PMID: 24196470. ](http://www.ncbi.nlm.nih.gov/pubmed/24196470)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24196470)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24196470)
RESPONSES FOR QUESTION 47 THROUGH 50
1. Observation
2. Arizona brace
3. Medial arch support
4. Casting
5. Hindfoot fusion
Select the most appropriate initial treatment from the list above to address each of the conditions described below.
Question 47High Yield
An 8-year-old boy with pes planus that reconstitutes with heel-rise; his mother brought him in for evaluation because he seems to be "tripping a lot".
Explanation
- Observation
Question 48High Yield
A 37-year-old woman has had persistent right lateral ankle pain after sustaining a minor sprain 5 months ago. She has a sense of instability on
uneven ground. Physical therapy has not helped. She is tender along the peroneal tendons and in the sinus tarsi. She has a negative anterior drawer test result for the ankle and no tenderness over the anterior lateral malleolus. She also has bilateral pes planus that persists with heel rise.
uneven ground. Physical therapy has not helped. She is tender along the peroneal tendons and in the sinus tarsi. She has a negative anterior drawer test result for the ankle and no tenderness over the anterior lateral malleolus. She also has bilateral pes planus that persists with heel rise.
Explanation
- Casting
Question 49High Yield
A 15-year-old high school basketball player has pain over a medial midfoot prominence on his right foot. There has been no trauma and no specific treatment. He has bilateral flexible pes planus and pain with inversion against resistance on the right. His pain is disrupting or preventing his daily and sports activities.
Explanation
- Casting
Question 50High Yield
A 69-year-old woman has rigid painful left pes planus that has become less symptomatic with casting. She has multiple comorbidities and is not a good surgical candidate. She has failed a trial of activity without any supports.




Explanation
Treatment for pes planus revolves around 2 clinical parameters: pain and rigidity. In the absence of pain, no intervention is warranted because there are no other symptoms that can reasonably be linked to the foot shape. Flexible pes planus (that corrects with heel rise) is usually normal and does not cause symptoms, but it can be associated with a symptomatic accessory navicular, in which case the patient may have pain over the medial navicular from either traction by the tibialis posterior or the act of rubbing against the medial shoe counter. Rigid pes planus is most frequently associated with a tarsal coalition, which classically presents in late adolescence but can become symptomatic for the first time in adults. The initial treatment for painful pes planus, whether flexible or rigid, is immobilization, usually in a walking cast. This often is sufficient to relieve symptoms on a permanent basis. Surgery should be contemplated only when this treatment fails. Adult-acquired flatfoot is most commonly attributable to tibialis posterior tendon dysfunction. In stage 3, the pes planus is rigid. If it is painful, surgical treatment, which consists of a triple arthrodesis, may be considered. However, if medical constraints or patient preference preclude surgery, an Arizona brace can provide sufficient support to reduce symptoms to an acceptable level to perform activities of daily living.
RECOMMENDED READINGS
[Varner KE, Michelson JD. Tarsal coalition in adults. Foot Ankle Int. 2000 Aug;21(8):669-72. PubMed PMID: 10966365. ](http://www.ncbi.nlm.nih.gov/pubmed/10966365)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10966365)
[Lin JL, Balbas J, Richardson EG. Results of non-surgical treatment of stage II posterior tibial tendon dysfunction: a 7- to 10-year followup. Foot Ankle Int. 2008 Aug;29(8):781-6. doi: 10.3113/FAI.2008.0781. PubMed PMID: 18752775. ](http://www.ncbi.nlm.nih.gov/pubmed/18752775)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18752775)
[Chao W, Wapner KL, Lee TH, Adams J, Hecht PJ. Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int. 1996 Dec;17(12):736-41. PubMed PMID: 8973895. ](http://www.ncbi.nlm.nih.gov/pubmed/8973895)[View](http://www.ncbi.nlm.nih.gov/pubmed/8973895)[ ](http://www.ncbi.nlm.nih.gov/pubmed/8973895)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8973895)
Cha SM, Shin HD, Kim KC, Lee JK. Simple excision vs the Kidner procedure for type 2 accessory navicular associated with flatfoot in pediatric population. Foot Ankle Int. 2013 Feb;34(2):167-72. doi: 10.1177/1071100712467616. Epub 2013 Jan 15. PubMed PMID:
[23413054/. ](http://www.ncbi.nlm.nih.gov/pubmed/%2023413054)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2023413054)
[Sullivan JA. Pediatric flatfoot: evaluation and management. J Am Acad Orthop Surg. 1999 Jan;7(1):44-53. PubMed PMID: 9916191.](http://www.ncbi.nlm.nih.gov/pubmed/9916191)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9916191)
CLINICAL SITUATION FOR QUESTIONS 51 AND 52
Figure 51a demonstrates the sneaker wear pattern and Figures 51b and 51c are the weight-bearing radiographs of a 20-year-old National Collegiate Athletic Association Division I basketball player. Throughout his college career he has experienced pain in the lateral aspect of his right foot. He has been treated with a clamshell orthotic, but this preseason his pain is worse than ever. Upon examination he has tenderness to palpation over the fifth metatarsal and his peroneal strength is 5/5 bilaterally
A
B
C
RECOMMENDED READINGS
[Varner KE, Michelson JD. Tarsal coalition in adults. Foot Ankle Int. 2000 Aug;21(8):669-72. PubMed PMID: 10966365. ](http://www.ncbi.nlm.nih.gov/pubmed/10966365)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10966365)
[Lin JL, Balbas J, Richardson EG. Results of non-surgical treatment of stage II posterior tibial tendon dysfunction: a 7- to 10-year followup. Foot Ankle Int. 2008 Aug;29(8):781-6. doi: 10.3113/FAI.2008.0781. PubMed PMID: 18752775. ](http://www.ncbi.nlm.nih.gov/pubmed/18752775)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18752775)
[Chao W, Wapner KL, Lee TH, Adams J, Hecht PJ. Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int. 1996 Dec;17(12):736-41. PubMed PMID: 8973895. ](http://www.ncbi.nlm.nih.gov/pubmed/8973895)[View](http://www.ncbi.nlm.nih.gov/pubmed/8973895)[ ](http://www.ncbi.nlm.nih.gov/pubmed/8973895)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8973895)
Cha SM, Shin HD, Kim KC, Lee JK. Simple excision vs the Kidner procedure for type 2 accessory navicular associated with flatfoot in pediatric population. Foot Ankle Int. 2013 Feb;34(2):167-72. doi: 10.1177/1071100712467616. Epub 2013 Jan 15. PubMed PMID:
[23413054/. ](http://www.ncbi.nlm.nih.gov/pubmed/%2023413054)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2023413054)
[Sullivan JA. Pediatric flatfoot: evaluation and management. J Am Acad Orthop Surg. 1999 Jan;7(1):44-53. PubMed PMID: 9916191.](http://www.ncbi.nlm.nih.gov/pubmed/9916191)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9916191)
CLINICAL SITUATION FOR QUESTIONS 51 AND 52
Figure 51a demonstrates the sneaker wear pattern and Figures 51b and 51c are the weight-bearing radiographs of a 20-year-old National Collegiate Athletic Association Division I basketball player. Throughout his college career he has experienced pain in the lateral aspect of his right foot. He has been treated with a clamshell orthotic, but this preseason his pain is worse than ever. Upon examination he has tenderness to palpation over the fifth metatarsal and his peroneal strength is 5/5 bilaterally
A
B
C
Question 51High Yield
What is the primary concern regarding resolution of this fracture?
Explanation
- Blood supply to this area
Question 52High Yield
Which treatment option will most reliably achieve long-term success?
Explanation
There are 3 types of fifth metatarsal fractures. Zone 1 is an avulsion fracture. Zone 2 fractures, also known as Jones fractures, occur in the watershed area of the fifth metatarsal. A fracture must exit the intermetatarsal articulation between the fourth and fifth metatarsals to be considered a Jones fracture. Zone 3 fractures are distal to the articulation in the diaphysis of the fifth metatarsal. Jones fractures are associated with a 15% to 20% nonunion rate with nonsurgical care. Surgical intervention is preferred in athletic patients. Fixation with a solid screw is mechanically stronger than fixation with a cannulated screw. Nonunions or failure of hardware can be attributable to inadequate fixation or an unrecognized varus heel alignment leading to lateral column overload.
RECOMMENDED READINGS
[Zenios M, Kim WY, Sampath J, Muddu BN. Functional treatment of acute metatarsal fractures: a prospective randomised comparison of management in a cast versus elasticated support bandage. Injury. 2005 Jul;36(7):832-5. Epub 2005 Mar 21. PubMed PMID: 15949484. ](http://www.ncbi.nlm.nih.gov/pubmed/15949484)[View](http://www.ncbi.nlm.nih.gov/pubmed/15949484)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15949484)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15949484)
[Fetzer GB, Wright RW. Metatarsal shaft fractures and fractures of the proximal fifth metatarsal. Clin Sports Med. 2006 Jan;25(1):139-50, x. Review. PubMed PMID: 16324980. ](http://www.ncbi.nlm.nih.gov/pubmed/16324980)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16324980)
[Zwitser EW, Breederveld RS. Fractures of the fifth metatarsal; diagnosis and treatment. Injury. 2010 Jun;41(6):555-62. doi: 10.1016/j.injury.2009.05.035. Epub 2009 Jun 30. Review. PubMed PMID: 19570536. ](http://www.ncbi.nlm.nih.gov/pubmed/19570536)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19570536)
Hunt KJ, Goeb Y, Esparza R, Malone M, Shultz R, Matheson G. Site-Specific Loading at the Fifth Metatarsal Base in Rehabilitative Devices: Implications for Jones Fracture Treatment. PM
R. 2014 May 28. pii: S1934-1482(14)00243-3. doi: 10.1016/j.pmrj.2014.05.011. [Epub
[ahead of print] PubMed PMID: 24880059. ](http://www.ncbi.nlm.nih.gov/pubmed/24880059)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24880059)
[Nunley JA. Fractures of the base of the fifth metatarsal: the Jones fracture. Orthop Clin North Am. 2001 Jan;32(1):171-80. Review. PubMed PMID: 11465126. ](http://www.ncbi.nlm.nih.gov/pubmed/11465126)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11465126)
Orr JD, Glisson RR, Nunley JA. Jones fracture fixation: a biomechanical comparison of partially threaded screws versus tapered variable pitch screws. Am J Sports Med. 2012 Mar;40(3):691-
8/. doi: 10.1177/0363546511428870. Epub 2012 Jan 6. PubMed PMID: 22227846.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22227846)
RECOMMENDED READINGS
[Zenios M, Kim WY, Sampath J, Muddu BN. Functional treatment of acute metatarsal fractures: a prospective randomised comparison of management in a cast versus elasticated support bandage. Injury. 2005 Jul;36(7):832-5. Epub 2005 Mar 21. PubMed PMID: 15949484. ](http://www.ncbi.nlm.nih.gov/pubmed/15949484)[View](http://www.ncbi.nlm.nih.gov/pubmed/15949484)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15949484)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15949484)
[Fetzer GB, Wright RW. Metatarsal shaft fractures and fractures of the proximal fifth metatarsal. Clin Sports Med. 2006 Jan;25(1):139-50, x. Review. PubMed PMID: 16324980. ](http://www.ncbi.nlm.nih.gov/pubmed/16324980)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16324980)
[Zwitser EW, Breederveld RS. Fractures of the fifth metatarsal; diagnosis and treatment. Injury. 2010 Jun;41(6):555-62. doi: 10.1016/j.injury.2009.05.035. Epub 2009 Jun 30. Review. PubMed PMID: 19570536. ](http://www.ncbi.nlm.nih.gov/pubmed/19570536)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19570536)
Hunt KJ, Goeb Y, Esparza R, Malone M, Shultz R, Matheson G. Site-Specific Loading at the Fifth Metatarsal Base in Rehabilitative Devices: Implications for Jones Fracture Treatment. PM
R. 2014 May 28. pii: S1934-1482(14)00243-3. doi: 10.1016/j.pmrj.2014.05.011. [Epub
[ahead of print] PubMed PMID: 24880059. ](http://www.ncbi.nlm.nih.gov/pubmed/24880059)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24880059)
[Nunley JA. Fractures of the base of the fifth metatarsal: the Jones fracture. Orthop Clin North Am. 2001 Jan;32(1):171-80. Review. PubMed PMID: 11465126. ](http://www.ncbi.nlm.nih.gov/pubmed/11465126)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11465126)
Orr JD, Glisson RR, Nunley JA. Jones fracture fixation: a biomechanical comparison of partially threaded screws versus tapered variable pitch screws. Am J Sports Med. 2012 Mar;40(3):691-
8/. doi: 10.1177/0363546511428870. Epub 2012 Jan 6. PubMed PMID: 22227846.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22227846)
Question 53High Yield
Figure 53 is a coronal-cut CT scan of a 63-year-old woman who has a longstanding pes planus. She is seen for lateral ankle discomfort. Upon examination she is tender over the sinus tarsi and distal to the fibula. She has painless passive hindfoot eversion with 5/5 eversion strength. The most appropriate diagnosis is

Explanation
With the use of CT scans, adults with symptomatic flatfoot deformity have been noted to develop subluxation of the talocalcaneal joint with resulting lateral hindfoot pain. Impingement of the talus and calcaneus in the sinus tarsi and/or between the tip of the fibula and the calcaneus may occur. This impingement is known as lateral impaction syndrome. Hindfoot motion is painless; therefore, this patient does not have symptomatic subtalar arthritis. Middle facet and calcaneonavicular coalitions are not present (hindfoot motion is present).
RECOMMENDED READINGS
[Malicky ES, Crary JL, Houghton MJ, Agel J, Hansen ST Jr, Sangeorzan BJ. Talocalcaneal and subfibular impingement in symptomatic flatfoot in adults. J Bone Joint Surg Am. 2002 Nov;84-A(11):2005-9. PubMed PMID: 12429762. ? ](http://www.ncbi.nlm.nih.gov/pubmed/12429762)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12429762)
[Ananthakrisnan D, Ching R, Tencer A, Hansen ST Jr, Sangeorzan BJ. Subluxation of the talocalcaneal joint in adults who have symptomatic flatfoot. J Bone Joint Surg Am. 1999 Aug;81(8):1147-54. PubMed PMID: 10466647. ?](http://www.ncbi.nlm.nih.gov/pubmed/10466647)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10466647)
RECOMMENDED READINGS
[Malicky ES, Crary JL, Houghton MJ, Agel J, Hansen ST Jr, Sangeorzan BJ. Talocalcaneal and subfibular impingement in symptomatic flatfoot in adults. J Bone Joint Surg Am. 2002 Nov;84-A(11):2005-9. PubMed PMID: 12429762. ? ](http://www.ncbi.nlm.nih.gov/pubmed/12429762)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12429762)
[Ananthakrisnan D, Ching R, Tencer A, Hansen ST Jr, Sangeorzan BJ. Subluxation of the talocalcaneal joint in adults who have symptomatic flatfoot. J Bone Joint Surg Am. 1999 Aug;81(8):1147-54. PubMed PMID: 10466647. ?](http://www.ncbi.nlm.nih.gov/pubmed/10466647)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10466647)
Question 54High Yield
Figure 54 is the lateral radiograph of a 55-year-old man who is evaluated for a 2-year history of pain and stiffness of his right metatarsophalangeal (MTP) joint. Upon examination he has dorsal bossing, severe crepitation, and pain
with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?
with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?



Explanation
The radiograph reveals end-stage degenerative changes of the first MTP joint with a dorsal loose body. MTP arthritis and decreased joint dorsiflexion is referred to as hallux rigidus. A chevron bunionectomy is used to correct hallux valgus deformity without arthritis. The cheilectomy is used in lesser degrees of joint destruction. Resection of the proximal phalanx results in a floppy toe and is generally not recommended.
RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23386758)
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2022661564)
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.
A B
RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23386758)
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2022661564)
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.
A B
Question 55High Yield
What is the most likely diagnosis?
Explanation
- Fracture dislocation of the Chopart joint
Question 56High Yield
What is the most appropriate initial treatment?
Explanation
- Attempted closed reduction under anesthesia with possible open reduction
Question 57High Yield
If a closed reduction is attempted, which structure most likely will prevent a reduction?
Explanation
- Tibialis posterior tendon
Question 58High Yield
After full healing from this injury, which option most likely will help to optimize this patient's activities?
Explanation
Midfoot fracture dislocations typically occur after a fall from a height or a motor vehicle collision involving severe dorsiflexion loading of the foot from a brake pedal or the floorboards. The deformity that results may be subtle because the subluxation may be a valgus or varus rotation around the midfoot rather than pure dorsiflexion. Early recognition and reduction is indicated to minimize secondary complications such as nerve injury or vascular compromise. Closed reduction usually necessitates formal anesthesia in an operating room to permit adequate relaxation and reduction. In many cases, satisfactory reduction can be accomplished closed, but the surgeon must be prepared to perform an open reduction if needed. The most common reason for failed closed reduction is that the talar head is caught by the tibialis posterior tendon (under which the talar head has protruded). This acts as a Chinese finger trap, preventing relocation by the usual distraction followed by
a plantar flexion maneuver. In these cases, open reduction is performed through a dorsomedial incision through which the tibialis posterior is retracted medially, allowing reduction of the talonavicular joint. The joints usually require pinning to maintain stability during healing. The long-term prognosis for these injuries is guarded because many patients develop degenerative changes in the Chopart joint. If symptomatic arthritis develops, helpful external supports are designed to limit sagittal motion at the joint (for example, carbon fiber inserts or rocker-bottom soles).
RECOMMENDED READINGS
[Swords MP, Schramski M, Switzer K, Nemec S. Chopart fractures and dislocations. Foot Ankle Clin. 2008 Dec;13(4):679-93, viii. Doi: 10.1016/j.fcl.2008.08.004. Review. PubMed PMID: 19013402.](http://www.ncbi.nlm.nih.gov/pubmed/19013402)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19013402)
[Richter M, Thermann H, Huefner T, Schmidt U, Goesling T, Krettek C. Chopart joint fracture-dislocation: initial open reduction provides better outcome than closed reduction. Foot Ankle Int. 2004 May;25(5):340-8. PubMed PMID: 15134617. ](http://www.ncbi.nlm.nih.gov/pubmed/15134617)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15134617)
a plantar flexion maneuver. In these cases, open reduction is performed through a dorsomedial incision through which the tibialis posterior is retracted medially, allowing reduction of the talonavicular joint. The joints usually require pinning to maintain stability during healing. The long-term prognosis for these injuries is guarded because many patients develop degenerative changes in the Chopart joint. If symptomatic arthritis develops, helpful external supports are designed to limit sagittal motion at the joint (for example, carbon fiber inserts or rocker-bottom soles).
RECOMMENDED READINGS
[Swords MP, Schramski M, Switzer K, Nemec S. Chopart fractures and dislocations. Foot Ankle Clin. 2008 Dec;13(4):679-93, viii. Doi: 10.1016/j.fcl.2008.08.004. Review. PubMed PMID: 19013402.](http://www.ncbi.nlm.nih.gov/pubmed/19013402)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19013402)
[Richter M, Thermann H, Huefner T, Schmidt U, Goesling T, Krettek C. Chopart joint fracture-dislocation: initial open reduction provides better outcome than closed reduction. Foot Ankle Int. 2004 May;25(5):340-8. PubMed PMID: 15134617. ](http://www.ncbi.nlm.nih.gov/pubmed/15134617)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15134617)
Question 59High Yield
Which lower extremity muscle is first weakened in Charcot-Marie-Tooth (CMT) disease?

Explanation
Although many of the lower extremity muscles may be affected in CMT, those innervated by the longest axons have been shown to be affected first. In the lower extremity the muscles innervated by the longest axons are the intrinsic foot muscles. The tibialis anterior and the peroneus brevis may be severely affected but not before the foot intrinsics. The peroneus longus typically is spared, resulting in the cavus.
RECOMMENDED READINGS
[Pareyson D, Marchesi C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol. 2009 Jul;8(7):654-67. Review. PubMed PMID: 19539237. ](http://www.ncbi.nlm.nih.gov/pubmed/19539237)[View](http://www.ncbi.nlm.nih.gov/pubmed/19539237)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19539237)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19539237)
Wenz W, Dreher T. Charcot-Marie-Tooth disease and the cavovarus foot. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:291-306.
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
Figure 60 is the standing radiograph of a 27-year-old man who played football throughout his teen years. During those years, he noted that he had less mobility of his left foot and ankle. He twisted his left foot and ankle 8 months ago and has tried over-the-counter nonsteroidal anti-inflammatory drugs and a brace. He now has pain and edema in the left sinus tarsi area. Upon examination the following arcs of motion are identified: ankle dorsiflexion-right, 5 degrees/left, 5 degrees; ankle plantar flexion-right, 30 degrees/left 30 degrees; foot inversion-right, 10 degrees/left, 5 degrees; foot eversion-right, 10 degrees/left 5 degrees.
RECOMMENDED READINGS
[Pareyson D, Marchesi C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol. 2009 Jul;8(7):654-67. Review. PubMed PMID: 19539237. ](http://www.ncbi.nlm.nih.gov/pubmed/19539237)[View](http://www.ncbi.nlm.nih.gov/pubmed/19539237)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19539237)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19539237)
Wenz W, Dreher T. Charcot-Marie-Tooth disease and the cavovarus foot. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:291-306.
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
Figure 60 is the standing radiograph of a 27-year-old man who played football throughout his teen years. During those years, he noted that he had less mobility of his left foot and ankle. He twisted his left foot and ankle 8 months ago and has tried over-the-counter nonsteroidal anti-inflammatory drugs and a brace. He now has pain and edema in the left sinus tarsi area. Upon examination the following arcs of motion are identified: ankle dorsiflexion-right, 5 degrees/left, 5 degrees; ankle plantar flexion-right, 30 degrees/left 30 degrees; foot inversion-right, 10 degrees/left, 5 degrees; foot eversion-right, 10 degrees/left 5 degrees.
Question 60High Yield
What are the most common locations of the pathology?
Explanation
- Talocalcaneal and calcaneonavicular joints
Question 61High Yield
What is the origin of this patient's pathology?
Explanation
- Genetic
Question 62High Yield
After a review of the images, it appears the appropriate next diagnostic step should be
Explanation
- CT scan.
Question 63High Yield
The patient undergoes further testing and it is discovered that the lesion encompasses 70% of the joint. What is the best next treatment option?
Explanation
A tarsal coalition is an abnormal connection of 2 or more bones in the foot. Although tarsal coalitions are present at birth, children and adults typically do not show signs of the disorder until early adolescence or later. The exact incidence of the disorder is hard to determine; however, it is caused by a gene mutation that affects cells that produce the tarsal bones. The 2 most common locations for tarsal coalitions are between the calcaneus and the navicular or between the talus and the calcaneus. It is estimated that 1 out of every 100 people may have a tarsal coalition. In 50% of cases, both feet are affected. Tarsal coalitions are rarely discovered until symptoms arise. Symptoms may include stiff and painful feet, a rigid flatfoot, or increased pain or a limp with high-level activities. Upon examination, symptoms may include tenderness in the area of the coalition, loss of motion, rigid flat feet, and arthritic changes of the joint. Imaging studies begin with radiographs. A CT scan can provide bony detail for imaging tarsal coalitions and determining the extent of the coalition and any accompanying degenerative change. MRI can provide details of the soft tissues. Treatment includes nonsurgical care including rest, orthotics, a temporary boot or cast, and injections. Surgical options include resection with interposition of muscle or fatty tissue from another area of the body or fusions when large (exceeding 50% of the joint), more severe coalitions are encountered.
RECOMMENDED READINGS
[Lemley F, Berlet G, Hill K, Philbin T, Isaac B, Lee T. Current concepts review: Tarsal coalition. Foot Ankle Int. 2006 Dec;27(12):1163-9. Review. PubMed PMID: 17207452. ](http://www.ncbi.nlm.nih.gov/pubmed/17207452)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/17207452)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17207452)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17207452)
[Badgley CE. Coalition of the calcaneus and the navicular. Arch Surg. 1927;15:75-88. Conway JJ, Cowell HR. Tarsal coalition: clinical significance and roentgenographic demonstration. Radiology. 1969 Mar;92(4):799-811. PubMed PMID: 5767760. ](http://www.ncbi.nlm.nih.gov/pubmed/5767760)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/5767760)[ ](http://www.ncbi.nlm.nih.gov/pubmed/5767760)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/5767760)
Herzenberg JE, Goldner JL, Martinez S, Silverman PM. Computerized tomography of talocalcaneal tarsal coalition: a clinical and anatomic study. Foot Ankle. 1986 Jun;6(6):273-
[88/. PubMed PMID: 3721364. ](http://www.ncbi.nlm.nih.gov/pubmed/3721364)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3721364)
[Wechsler RJ, Schweitzer ME, Deely DM, Horn BD, Pizzutillo PD. Tarsal coalition: depiction and characterization with CT and MR imaging. Radiology. 1994 Nov;193(2):447-52. PubMed PMID: 7972761. ](http://www.ncbi.nlm.nih.gov/pubmed/7972761)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7972761)
[Leonard MA. The inheritance of tarsal coalition and its relationship to spastic flat foot. J Bone Joint Surg Br. 1974 Aug;56B(3):520-6. PubMed PMID: 4421359. ](http://www.ncbi.nlm.nih.gov/pubmed/4421359)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4421359)
RECOMMENDED READINGS
[Lemley F, Berlet G, Hill K, Philbin T, Isaac B, Lee T. Current concepts review: Tarsal coalition. Foot Ankle Int. 2006 Dec;27(12):1163-9. Review. PubMed PMID: 17207452. ](http://www.ncbi.nlm.nih.gov/pubmed/17207452)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/17207452)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17207452)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17207452)
[Badgley CE. Coalition of the calcaneus and the navicular. Arch Surg. 1927;15:75-88. Conway JJ, Cowell HR. Tarsal coalition: clinical significance and roentgenographic demonstration. Radiology. 1969 Mar;92(4):799-811. PubMed PMID: 5767760. ](http://www.ncbi.nlm.nih.gov/pubmed/5767760)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/5767760)[ ](http://www.ncbi.nlm.nih.gov/pubmed/5767760)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/5767760)
Herzenberg JE, Goldner JL, Martinez S, Silverman PM. Computerized tomography of talocalcaneal tarsal coalition: a clinical and anatomic study. Foot Ankle. 1986 Jun;6(6):273-
[88/. PubMed PMID: 3721364. ](http://www.ncbi.nlm.nih.gov/pubmed/3721364)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3721364)
[Wechsler RJ, Schweitzer ME, Deely DM, Horn BD, Pizzutillo PD. Tarsal coalition: depiction and characterization with CT and MR imaging. Radiology. 1994 Nov;193(2):447-52. PubMed PMID: 7972761. ](http://www.ncbi.nlm.nih.gov/pubmed/7972761)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7972761)
[Leonard MA. The inheritance of tarsal coalition and its relationship to spastic flat foot. J Bone Joint Surg Br. 1974 Aug;56B(3):520-6. PubMed PMID: 4421359. ](http://www.ncbi.nlm.nih.gov/pubmed/4421359)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4421359)
Question 64High Yield
A
B
C
Figures 64a through 64c are the MR images and radiograph of an active 30-year-old man who has been treated for pain in his subtalar joint for 6 months. He has had casting, physical therapy, and bracing but continues to have activity-limiting pain. An injection into the subtalar joint under fluoroscopic guidance temporarily relieved his pain. His best surgical option at this time is
B
C
Figures 64a through 64c are the MR images and radiograph of an active 30-year-old man who has been treated for pain in his subtalar joint for 6 months. He has had casting, physical therapy, and bracing but continues to have activity-limiting pain. An injection into the subtalar joint under fluoroscopic guidance temporarily relieved his pain. His best surgical option at this time is



Explanation
When contemplating the causes of subtalar joint degeneration in young patients, an unstable tarsal coalition should be considered in the absence of antecedent trauma. Initial treatment with casting is appropriate because this intervention can relieve symptoms for many patients. There are 2 surgical options for a symptomatic tarsal coalition: bar resection or completion fusion. Risk factors for a poor outcome after bar resection are adult age and a bar that encompasses more than 50% of the middle facet of the subtalar joint. Because this patient has both risk factors, the appropriate procedure is a subtalar fusion.
RECOMMENDED READINGS
[Comfort TK, Johnson LO. Resection for symptomatic talocalcaneal coalition. J PediatrOrthop. 1998 May-Jun;18(3):283-8. PubMed PMID: 9600549. ](http://www.ncbi.nlm.nih.gov/pubmed/9600549)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9600549)
[Thorpe SW, Wukich DK. Tarsal coalitions in the adult population: does treatment differ from the adolescent? Foot Ankle Clin. 2012 Jun;17(2):195-204. doi: 10.1016/j.fcl.2012.03.004. Epub 2012 Apr 6. Review. PubMed PMID: 22541520. ](http://www.ncbi.nlm.nih.gov/pubmed/22541520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22541520)
RECOMMENDED READINGS
[Comfort TK, Johnson LO. Resection for symptomatic talocalcaneal coalition. J PediatrOrthop. 1998 May-Jun;18(3):283-8. PubMed PMID: 9600549. ](http://www.ncbi.nlm.nih.gov/pubmed/9600549)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9600549)
[Thorpe SW, Wukich DK. Tarsal coalitions in the adult population: does treatment differ from the adolescent? Foot Ankle Clin. 2012 Jun;17(2):195-204. doi: 10.1016/j.fcl.2012.03.004. Epub 2012 Apr 6. Review. PubMed PMID: 22541520. ](http://www.ncbi.nlm.nih.gov/pubmed/22541520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22541520)
Question 65High Yield
What is a risk factor for interdigital neuroma?
Explanation
The only proven risk factor for development of an interdigital neuroma is female gender, which likely is related to the use of fashionable shoes that force plantar flexion of the metatarsal heads and secondary hyperdorsiflexion of the metatarsophalangeal joints. The other factors listed have not been proven to cause interdigital neuroma, as well as mediolateral compression of the forefoot.
RECOMMENDED READINGS
Hill KJ. Peripheral nerve disorder. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:307-327.
Schon LC, Mann RA. Diseases of the nerves. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:613-686.
RECOMMENDED READINGS
Hill KJ. Peripheral nerve disorder. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:307-327.
Schon LC, Mann RA. Diseases of the nerves. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:613-686.
Question 66High Yield
Which Morton neuroma histology is most common?
Explanation
Morton neuroma is a compressive neuropathy of the interdigital nerves of the forefoot that most commonly is noted in the third web space. Perineural fibrosis is commonly noted on microscopic examination of resected tissue. This accounts for the relatively higher failure rate of neuroma decompression by transection of the intermetatarsal ligament as opposed to resection. Wallerian degeneration is seen following axonal transection in the distal part of the nerve. Distal axonopathy is degeneration of the axon and myelin and is associated with "stocking-glove" distribution neuropathy. Segmental demyelination is characterized by breakdown of myelin with an intact axon
and is associated with lead poisoning and hereditary sensory motor neuropathy.
RECOMMENDED READINGS
[Akermark C, Crone H, Saartok T, Zuber Z. Plantar versus dorsal incision in the treatment of primary intermetatarsal Morton's neuroma. Foot Ankle Int. 2008 Feb;29(2):136-41. doi: 10.3113/FAI.2008.0136. PubMed PMID: 18315967.](http://www.ncbi.nlm.nih.gov/pubmed/18315967)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18315967)
[Ha'Eri GB, Fornasier VL, Schatzker J. Morton's neuroma--pathogenesis and ultrastructure. Clin Orthop Relat Res. 1979 Jun;(141):256-9. PubMed PMID: 477115. ](http://www.ncbi.nlm.nih.gov/pubmed/477115)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/477115)[ ](http://www.ncbi.nlm.nih.gov/pubmed/477115)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/477115)
[Graham CE, Graham DM. Morton's neuroma: a microscopic evaluation. Foot Ankle. 1984 Nov-Dec;5(3):150-3. PubMed PMID: 6519606. ](http://www.ncbi.nlm.nih.gov/pubmed/6519606)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6519606)
and is associated with lead poisoning and hereditary sensory motor neuropathy.
RECOMMENDED READINGS
[Akermark C, Crone H, Saartok T, Zuber Z. Plantar versus dorsal incision in the treatment of primary intermetatarsal Morton's neuroma. Foot Ankle Int. 2008 Feb;29(2):136-41. doi: 10.3113/FAI.2008.0136. PubMed PMID: 18315967.](http://www.ncbi.nlm.nih.gov/pubmed/18315967)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18315967)
[Ha'Eri GB, Fornasier VL, Schatzker J. Morton's neuroma--pathogenesis and ultrastructure. Clin Orthop Relat Res. 1979 Jun;(141):256-9. PubMed PMID: 477115. ](http://www.ncbi.nlm.nih.gov/pubmed/477115)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/477115)[ ](http://www.ncbi.nlm.nih.gov/pubmed/477115)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/477115)
[Graham CE, Graham DM. Morton's neuroma: a microscopic evaluation. Foot Ankle. 1984 Nov-Dec;5(3):150-3. PubMed PMID: 6519606. ](http://www.ncbi.nlm.nih.gov/pubmed/6519606)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6519606)
Question 67High Yield
A patient sustained a puncture wound to the plantar aspect of his foot. He was wearing shoes and socks at the time of the injury. Systemic antibiotic administration with specific coverage for which bacterial species (in addition to Staphylococcus aureus) should be instituted?
Explanation
Puncture wounds sustained through a shoe and sock increase risk for Pseudomonas infection. Clostridium are associated with soil-contaminated wounds. Mycobacterium marinum is associated with injuries sustained within water.
RECOMMENDED READINGS
[DeCoster TA, Miller RA. Management of Traumatic Foot Wounds. J Am Acad Orthop Surg. 1994 Jul;2(4):226-230. PubMed PMID: 10709013. ](http://www.ncbi.nlm.nih.gov/pubmed/10709013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10709013)
Raikin SM. Common infections of the foot. In: Richardson EG, ed. Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2004:199-205.
RECOMMENDED READINGS
[DeCoster TA, Miller RA. Management of Traumatic Foot Wounds. J Am Acad Orthop Surg. 1994 Jul;2(4):226-230. PubMed PMID: 10709013. ](http://www.ncbi.nlm.nih.gov/pubmed/10709013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10709013)
Raikin SM. Common infections of the foot. In: Richardson EG, ed. Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2004:199-205.
Question 68High Yield
Figure 68 is the radiograph of a 33-year-old runner who recently decided to begin running barefoot on trails. Since his transition to running without shoes 3 months ago, he has been having pain in the second metatarsophalangeal (MTP) joint. He feels like he is walking on a stone, notes edema in the ball of his foot, and has started to see a deviation of the second toe. What is the most likely etiology of these symptoms and findings?

Explanation
Lesser-toe plantar plate injuries are becoming increasingly recognized. Patients typically have an increase in pain, a positive Lachman test result upon examination, and deviation of the MTP joint. On radiograph, MTP subluxation can be appreciated. Nonsurgical treatment with a metatarsal pad may be attempted. Many patients who have surgery will have a partial or full tear of the plantar plate. The repair necessitates reinsertion of the plantar plate to the base of the proximal phalanx.
RECOMMENDED READINGS
[Doty JF, Coughlin MJ, Weil L Jr, Nery C. Etiology and management of lesser toe metatarsophalangeal joint instability. Foot Ankle Clin. 2014 Sep;19(3):385-405. doi: 10.1016/j.fcl.2014.06.013. Epub 2014 Jul 10. PubMed PMID: 25129351. ](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[ ](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25129351)
Nery C, Coughlin MJ, Baumfeld D, Raduan FC, Mann TS, Catena F. Prospective evaluation of protocol for surgical treatment of lesser MTP joint plantar plate tears. Foot Ankle Int. 2014 Sep;35(9):876-85. doi: 10.1177/1071100714539659. Epub 2014 Jun 23. PubMed PMID:
[24958766/. ](http://www.ncbi.nlm.nih.gov/pubmed/24958766)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24958766)
[Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantar plate and surgical reconstruction techniques on static stability of lesser metatarsophalangeal joints: a biomechanical study. Foot Ankle Int. 2013 Oct;34(10):1436-42. doi: 10.1177/1071100713491728. Epub 2013 Jun 17. PubMed PMID: 23774466. ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23774466)
RECOMMENDED READINGS
[Doty JF, Coughlin MJ, Weil L Jr, Nery C. Etiology and management of lesser toe metatarsophalangeal joint instability. Foot Ankle Clin. 2014 Sep;19(3):385-405. doi: 10.1016/j.fcl.2014.06.013. Epub 2014 Jul 10. PubMed PMID: 25129351. ](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[ ](http://www.ncbi.nlm.nih.gov/pubmed/25129351)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25129351)
Nery C, Coughlin MJ, Baumfeld D, Raduan FC, Mann TS, Catena F. Prospective evaluation of protocol for surgical treatment of lesser MTP joint plantar plate tears. Foot Ankle Int. 2014 Sep;35(9):876-85. doi: 10.1177/1071100714539659. Epub 2014 Jun 23. PubMed PMID:
[24958766/. ](http://www.ncbi.nlm.nih.gov/pubmed/24958766)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24958766)
[Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantar plate and surgical reconstruction techniques on static stability of lesser metatarsophalangeal joints: a biomechanical study. Foot Ankle Int. 2013 Oct;34(10):1436-42. doi: 10.1177/1071100713491728. Epub 2013 Jun 17. PubMed PMID: 23774466. ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23774466)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23774466)
Question 69High Yield
Figure 69 is the radiograph of a 9-year-old who has posterior hindfoot pain while running. What is the most likely diagnosis?

Explanation
Sever disease is a traction apophysitis at the Achilles tendon insertion on the calcaneus. Plain radiographs may be unremarkable for this condition. Other osteochondroses of the foot include Kohler disease (tarsal navicular), Freiberg infraction (lesser metatarsal head), and Thiemann disease (great toe phalanx).
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
[Schantz K, Rasmussen F. Thiemann's finger or toe disease. Follow-up of seven cases. Acta Orthop Scand. 1986 Feb;57(1):91-3. PubMed PMID: 3962642. ](http://www.ncbi.nlm.nih.gov/pubmed/3962642)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3962642)
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
[Schantz K, Rasmussen F. Thiemann's finger or toe disease. Follow-up of seven cases. Acta Orthop Scand. 1986 Feb;57(1):91-3. PubMed PMID: 3962642. ](http://www.ncbi.nlm.nih.gov/pubmed/3962642)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3962642)
Question 70High Yield
A 62-year-old runner injured his right ankle 8 weeks ago. He has ongoing lateral ankle pain and swelling that did not improve with 4 weeks of immobilization and 4 weeks of physical therapy. MR images demonstrate a longitudinal tear of the peroneus brevis tendon. Treatment should involve
Explanation
Additional nonsurgical treatment is not beneficial for peroneal tendon tears. Early repair of longitudinal tears reduces risk for progression to a full-thickness tear that would necessitate peroneus brevis to peroneus longus tenodesis. Platelet-rich plasma has no role in peroneal tendon tears.
RECOMMENDED READINGS
Arbab D, Tingart M, Frank D, Abbara-Czardybon M, Waizy H, Wingenfeld C. Treatment of isolated peroneus longus tears and a review of the literature. Foot Ankle Spec. 2014 Apr;7(2):113-8. doi: 10.1177/1938640013514273. Epub 2013 Dec 30. Review. PubMed
[PMID: 24381076.](http://www.ncbi.nlm.nih.gov/pubmed/24381076)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24381076)
Coughlin MJ, Schon LC. Disorders of tendons. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014: 1188-1291.
RESPONSES FOR QUESTIONS 71 THROUGH 75
1. Lapidus procedure
2. First metatarsophalangeal (MTP) joint arthrodesis and lesser metatarsal head resection
3. Proximal first metatarsal osteotomy
4. Distal first metatarsal chevron osteotomy
5. Biplanar distal first metatarsal osteotomy
Match the appropriate surgical procedure listed above with the clinical scenario described below.
RECOMMENDED READINGS
Arbab D, Tingart M, Frank D, Abbara-Czardybon M, Waizy H, Wingenfeld C. Treatment of isolated peroneus longus tears and a review of the literature. Foot Ankle Spec. 2014 Apr;7(2):113-8. doi: 10.1177/1938640013514273. Epub 2013 Dec 30. Review. PubMed
[PMID: 24381076.](http://www.ncbi.nlm.nih.gov/pubmed/24381076)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24381076)
Coughlin MJ, Schon LC. Disorders of tendons. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014: 1188-1291.
RESPONSES FOR QUESTIONS 71 THROUGH 75
1. Lapidus procedure
2. First metatarsophalangeal (MTP) joint arthrodesis and lesser metatarsal head resection
3. Proximal first metatarsal osteotomy
4. Distal first metatarsal chevron osteotomy
5. Biplanar distal first metatarsal osteotomy
Match the appropriate surgical procedure listed above with the clinical scenario described below.
Question 71High Yield
Figure 71 is the radiograph of a 67-year-old patient with rheumatoid arthritis who has experienced 6 months of increasing pain, swelling, and foot deformity. Anti-inflammatory medications, orthotics, and extra-depth shoes fail to provide sufficient relief.
71
71

Explanation
- First metatarsophalangeal (MTP) joint arthrodesis and lesser metatarsal head resection
Question 72High Yield
72
Figure 72 is the radiograph of a 58-year-old active woman with progressive medial first MTP joint pain, particularly with shoe wear and increased activity. The patient has no hypermobility.
Figure 72 is the radiograph of a 58-year-old active woman with progressive medial first MTP joint pain, particularly with shoe wear and increased activity. The patient has no hypermobility.

Explanation
- Proximal first metatarsal osteotomy
Question 73High Yield
A 44-year-old patient who has had a proximal first metatarsal osteotomy has recurrent pain and difficulty wearing many types of shoes. Radiographs show a large 1-2 intermetatarsal angle (IMA).

Explanation
- Lapidus procedure
Question 74High Yield
74
Figure 74 is the radiograph of a 31-year-old woman with a painful bunion deformity that has failed nonsurgical treatment.
Figure 74 is the radiograph of a 31-year-old woman with a painful bunion deformity that has failed nonsurgical treatment.
Explanation
- Distal first metatarsal chevron osteotomy
Question 75High Yield



Explanation
Most cases of HV should initially be treated nonsurgically. When indicated, the decision to pursue surgical treatment of HV is dependent on a variety of factors including presence of arthritis, joint stability/ligamentous laxity, congruence of the first MTP joint, and severity of deformity. Mild congruent HV may be treated with a distal chevron osteotomy. A distal soft-tissue procedure may be added if the deformity is incongruent. Moderate to severe HV deformities may be treated with proximal first metatarsal osteotomies such as the crescentic, Ludloff, or scarf osteotomy. Larger HV deformities are almost always associated with incongruent HV angles, and they necessitate a distal soft-tissue procedure to realign the first MTP joint. Fusion of the first MTP joint
is indicated in cases of severe HV deformity or associated osteoarthritis or rheumatoid arthritis. The Lapidus procedure, an arthrodesis of the first metatarsal-medial cuneiform joint, has been a success when used to treat patients with first-ray instability (hypermobility) or as a salvage procedure for those who have bunion recurrence after previous surgery. A biplanar distal chevron osteotomy is indicated for congruent HV deformities involving a large DMAA (the angle measured between the slope of the articular surface of the first metatarsal head and the longitudinal axis of the first metatarsal).
RECOMMENDED READINGS
[Coughlin MJ, Jones CP. Hallux valgus and first ray mobility. A prospective study. J Bone Joint Surg Am. 2007 Sep;89(9):1887-98. PubMed PMID: 17768183. ](http://www.ncbi.nlm.nih.gov/pubmed/17768183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17768183) [Robinson AH, Limbers JP. Modern concepts in the treatment of hallux valgus. J Bone Joint Surg Br. 2005 Aug;87(8):1038-45. Review. PubMed PMID: 16049235. ](http://www.ncbi.nlm.nih.gov/pubmed/16049235)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16049235)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16049235)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16049235)
[Coetzee JC, Wickum D. The Lapidus procedure: a prospective cohort outcome study. Foot Ankle Int. 2004 Aug;25(8):526-31. PubMed PMID: 15363372. ](http://www.ncbi.nlm.nih.gov/pubmed/15363372)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15363372) Coughlin MJ, Mann RA. Hallux valgus. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:230-236.
CLINICAL SITUATION FOR QUESTIONS 76 THROUGH 79
Figures 76a through 76c are the clinical photograph and radiographs of a 48-year-old man with a 10-year history of diabetes who has an open wound on his left foot. He had neither previous trauma nor earlier similar occurrences. His diabetes is well controlled, with a hemoglobin A1c level of 6.7% (reference range, 4%-7%). His examination is notable for well-perfused feet with intact pulses and intact sensation to light touch. There is mild tenderness over the left forefoot. The erythema in the forefoot does not resolve with elevation. The head of the fifth metatarsal can be probed through the wound.
A
2. C
is indicated in cases of severe HV deformity or associated osteoarthritis or rheumatoid arthritis. The Lapidus procedure, an arthrodesis of the first metatarsal-medial cuneiform joint, has been a success when used to treat patients with first-ray instability (hypermobility) or as a salvage procedure for those who have bunion recurrence after previous surgery. A biplanar distal chevron osteotomy is indicated for congruent HV deformities involving a large DMAA (the angle measured between the slope of the articular surface of the first metatarsal head and the longitudinal axis of the first metatarsal).
RECOMMENDED READINGS
[Coughlin MJ, Jones CP. Hallux valgus and first ray mobility. A prospective study. J Bone Joint Surg Am. 2007 Sep;89(9):1887-98. PubMed PMID: 17768183. ](http://www.ncbi.nlm.nih.gov/pubmed/17768183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17768183) [Robinson AH, Limbers JP. Modern concepts in the treatment of hallux valgus. J Bone Joint Surg Br. 2005 Aug;87(8):1038-45. Review. PubMed PMID: 16049235. ](http://www.ncbi.nlm.nih.gov/pubmed/16049235)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16049235)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16049235)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16049235)
[Coetzee JC, Wickum D. The Lapidus procedure: a prospective cohort outcome study. Foot Ankle Int. 2004 Aug;25(8):526-31. PubMed PMID: 15363372. ](http://www.ncbi.nlm.nih.gov/pubmed/15363372)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15363372) Coughlin MJ, Mann RA. Hallux valgus. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:230-236.
CLINICAL SITUATION FOR QUESTIONS 76 THROUGH 79
Figures 76a through 76c are the clinical photograph and radiographs of a 48-year-old man with a 10-year history of diabetes who has an open wound on his left foot. He had neither previous trauma nor earlier similar occurrences. His diabetes is well controlled, with a hemoglobin A1c level of 6.7% (reference range, 4%-7%). His examination is notable for well-perfused feet with intact pulses and intact sensation to light touch. There is mild tenderness over the left forefoot. The erythema in the forefoot does not resolve with elevation. The head of the fifth metatarsal can be probed through the wound.
A
2. C
Question 76High Yield
What is the most common underlying etiology for this condition in this clinical setting?
Explanation
- Sensory neuropathy
Question 77High Yield
If nonsurgical treatment of this wound fails, the most likely cause for failure is
Explanation
- underlying osteomyelitis.
Question 78High Yield
If surgery is necessary, what is the most appropriate procedure?
Explanation
- Debridement of all infected tissue and a negative-pressure dressing for the resulting wound
Question 79High Yield
After the patient's wound has healed, which intervention is critical to prevent future ulceration?
Explanation
The most common etiology for plantar ulcers in patients with diabetes is neuropathy; 80% of these patients have adequate vascularity. The pathobiology is increased pressure applied on skin that lacks protective sensation (detected by lack of sensation to Semmes-Weinstein monofilament 5.07). The presence of sensation to light touch is not predictive of ulcer risk, but absent Semmes-Weinstein sensation at 5.07 carries a 30% risk for developing an ulcer. Intact light touch sensation does not rule out loss of protective sensation, and, therefore, does not rule out sensory neuropathy. The grading of an ulcer primarily depends on the existence of deep infection, either an abscess or osteomyelitis. In the presence of deep infection, formal surgical debridement is required. The surgery should be limited to the tissues
that are compromised, without an attempt at primary closure (which increases risk for recurrent infection). Negative-pressure dressings are a significant advance in postsurgical treatment by permitting delayed healing without further surgical intervention. Once healed, the key to preventing recurrent ulceration is the use of orthopaedic shoes with custom-molded soft inserts that accommodate the contours of the feet. This is particularly true when surgery has removed a portion of the foot; the foot otherwise will shift in a shoe that does not include a custom molded insert incorporating a filler that occupies the space left by the surgical resection.
RECOMMENDED READINGS
[Pham H, Armstrong DG, Harvey C, Harkless LB, Giurini JM, Veves A. Screening techniques to identify people at high risk for diabetic foot ulceration: a prospective multicenter trial. Diabetes Care. 2000 May;23(5):606-11. PubMed PMID: 10834417. ](http://www.ncbi.nlm.nih.gov/pubmed/10834417)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10834417) [Pinzur MS, Slovenkai MP, Trepman E, Shields NN; Diabetes Committee of American Orthopaedic Foot and Ankle Society. Guidelines for diabetic foot care: recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int. 2005 Jan;26(1):113-9. PubMed PMID: 15680122. ](http://www.ncbi.nlm.nih.gov/pubmed/%2015680122)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2015680122) Chantelau E. Effectiveness of diabetic therapeutic footwear in preventing reulceration: response to Maciejewski et al. Diabetes Care. 2004 Dec;27(12):3024-5; author reply 3025-
[6/. PubMed PMID: 15562237. ](http://www.ncbi.nlm.nih.gov/pubmed/15562237)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15562237)
that are compromised, without an attempt at primary closure (which increases risk for recurrent infection). Negative-pressure dressings are a significant advance in postsurgical treatment by permitting delayed healing without further surgical intervention. Once healed, the key to preventing recurrent ulceration is the use of orthopaedic shoes with custom-molded soft inserts that accommodate the contours of the feet. This is particularly true when surgery has removed a portion of the foot; the foot otherwise will shift in a shoe that does not include a custom molded insert incorporating a filler that occupies the space left by the surgical resection.
RECOMMENDED READINGS
[Pham H, Armstrong DG, Harvey C, Harkless LB, Giurini JM, Veves A. Screening techniques to identify people at high risk for diabetic foot ulceration: a prospective multicenter trial. Diabetes Care. 2000 May;23(5):606-11. PubMed PMID: 10834417. ](http://www.ncbi.nlm.nih.gov/pubmed/10834417)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10834417) [Pinzur MS, Slovenkai MP, Trepman E, Shields NN; Diabetes Committee of American Orthopaedic Foot and Ankle Society. Guidelines for diabetic foot care: recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int. 2005 Jan;26(1):113-9. PubMed PMID: 15680122. ](http://www.ncbi.nlm.nih.gov/pubmed/%2015680122)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2015680122) Chantelau E. Effectiveness of diabetic therapeutic footwear in preventing reulceration: response to Maciejewski et al. Diabetes Care. 2004 Dec;27(12):3024-5; author reply 3025-
[6/. PubMed PMID: 15562237. ](http://www.ncbi.nlm.nih.gov/pubmed/15562237)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15562237)
Question 80High Yield
Which repair technique for an osteochondral lesion of the medial talus shoulder produces hyaline cartilage that is similar to native cartilage and will not degrade over time?
Explanation
Autologous osteochondral transplantation (typically involving tubular grafts harvested from the knee) has been shown to replace a talar defect with viable hyaline cartilage. The results over the medium term show good clinical outcomes, and MRI studies reveal cartilage repair similar to native cartilage. Chondroplasty and arthroscopic bone-marrow stimulation are both associated with good clinical results for smaller lesions, but these techniques develop fibrocartilaginous repair tissue composed of type I collagen instead of hyaline cartilage. Osteochondral transplantation of fresh allografts performed less than 14 days after harvest contains high chondrocyte viability. Few clinical studies report long-term results, but radiographic studies demonstrate high rates of collapse and resorption. Joint space narrowing has been noted in 60% of ankles treated with bulk grafts after an average of 44 months. Autologous chondrocyte implantation (both periosteum-covered and matrix-associated techniques) has been shown to create hyaline cartilage in some studies, but fibrocartilage creation has been reported in others.
RECOMMENDED READINGS
[Schachter AK, Chen AL, Reddy PD, Tejwani NC. Osteochondral lesions of the talus. J Am Acad Orthop Surg. 2005 May-Jun;13(3):152-8. Review. PubMed PMID: 15938604. ](http://www.ncbi.nlm.nih.gov/pubmed/15938604)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/15938604)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15938604)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15938604)
[Mitchell ME, Giza E, Sullivan MR. Cartilage transplantation techniques for talar cartilage lesions. J Am Acad Orthop Surg. 2009 Jul;17(7):407-14. Review. PubMed PMID: 19571296. ](http://www.ncbi.nlm.nih.gov/pubmed/19571296)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19571296)
[Murawski CD, Kennedy JG. Operative treatment of osteochondral lesions of the talus. J Bone Joint Surg Am. 2013 Jun 5;95(11):1045-54. doi: 10.2106/JBJS.L.00773. Review. PubMed PMID: 23780543. ](http://www.ncbi.nlm.nih.gov/pubmed/23780543)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23780543)
RECOMMENDED READINGS
[Schachter AK, Chen AL, Reddy PD, Tejwani NC. Osteochondral lesions of the talus. J Am Acad Orthop Surg. 2005 May-Jun;13(3):152-8. Review. PubMed PMID: 15938604. ](http://www.ncbi.nlm.nih.gov/pubmed/15938604)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/15938604)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15938604)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15938604)
[Mitchell ME, Giza E, Sullivan MR. Cartilage transplantation techniques for talar cartilage lesions. J Am Acad Orthop Surg. 2009 Jul;17(7):407-14. Review. PubMed PMID: 19571296. ](http://www.ncbi.nlm.nih.gov/pubmed/19571296)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19571296)
[Murawski CD, Kennedy JG. Operative treatment of osteochondral lesions of the talus. J Bone Joint Surg Am. 2013 Jun 5;95(11):1045-54. doi: 10.2106/JBJS.L.00773. Review. PubMed PMID: 23780543. ](http://www.ncbi.nlm.nih.gov/pubmed/23780543)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23780543)
Question 81High Yield
What is the most common turf toe mechanism of injury?
Explanation
Turf toe, or capsuloligamentous injury to the first MTP joint, most commonly is caused by an axial load being applied to a fixed, dorsiflexed great toe with the heel off the ground. The external force causes further dorsiflexion of the great toe, leading to injury to the capsuloligamentous complex. A less common mechanism of turf toe is hyperplantarflexion of the great toe with valgus stress, which is seen in beach volleyball players.
RECOMMENDED READINGS
[Kadakia AR, Molloy A. Current concepts review: traumatic disorders of the first metatarsophalangeal joint and sesamoid complex. Foot Ankle Int. 2011 Aug;32(8):834-9. Review. PubMed PMID: 22049873. ](http://www.ncbi.nlm.nih.gov/pubmed/22049873)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22049873)
Clanton TO, McGarvey W. Athletic Injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:1526-1535
RECOMMENDED READINGS
[Kadakia AR, Molloy A. Current concepts review: traumatic disorders of the first metatarsophalangeal joint and sesamoid complex. Foot Ankle Int. 2011 Aug;32(8):834-9. Review. PubMed PMID: 22049873. ](http://www.ncbi.nlm.nih.gov/pubmed/22049873)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22049873)
Clanton TO, McGarvey W. Athletic Injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:1526-1535
Question 82High Yield
A
B
Figures 82a and 82b are the clinical photograph and radiograph of a 60-year-old man with a 30-year history of diabetes complicated by borderline chronic
renal failure, heart failure controlled by medication, and bilateral lower extremity neuropathy. He is currently wheelchair bound because of his cardiopulmonary limitations, but uses his legs for transfers. He has had a progressive left ankle deformity that has progressed to the point at which he cannot use his leg for pivot transfers. He is adamant that something should be done to improve his living situation. Which surgical option can best achieve his goal of using the leg for transfers?
B
Figures 82a and 82b are the clinical photograph and radiograph of a 60-year-old man with a 30-year history of diabetes complicated by borderline chronic
renal failure, heart failure controlled by medication, and bilateral lower extremity neuropathy. He is currently wheelchair bound because of his cardiopulmonary limitations, but uses his legs for transfers. He has had a progressive left ankle deformity that has progressed to the point at which he cannot use his leg for pivot transfers. He is adamant that something should be done to improve his living situation. Which surgical option can best achieve his goal of using the leg for transfers?




Explanation
The indications for surgery in a Charcot joint are an unbraceable deformity or recurrent ulceration despite use of adequate bracing. Any significant varus/valgus deformity of the ankle or hindfoot (as in this patient) is unbraceable, whereas midfoot Charcot deformities usually can be treated nonsurgically. The goal of surgery is to provide a stable aligned foot and ankle to permit activities and reduce risk for recurrent ulceration. This does not mean that there has to be a radiographic fusion because many patients with diabetes achieve a stable nonunion without pain. The only surgical construct that will provide long-term inherent stability and alignment in this situation is use of a hindfoot fusion rod. It provides better stability and purchase than screw fixation and can be left in indefinitely (unlike an external fixator).
RECOMMENDED READINGS
[Dalla Paola L, Volpe A, Varotto D, Postorino A, Brocco E, Senesi A, Merico M, De Vido D, Da Ros R, Assaloni R. Use of a retrograde nail for ankle arthrodesis in Charcot neuroarthropathy: a limb salvage procedure. Foot Ankle Int. 2007 Sep;28(9):967-70. PubMed PMID: 17880869. ](http://www.ncbi.nlm.nih.gov/pubmed/17880869)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17880869)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17880869)
[Pinzur MS. Benchmark analysis of diabetic patients with neuropathic (Charcot) foot deformity. Foot Ankle Int. 1999 Sep;20(9):564-7. PubMed PMID: 10509683. ](http://www.ncbi.nlm.nih.gov/pubmed/10509683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10509683) [Pinzur M. Surgical versus accommodative treatment for Charcot arthropathy of the midfoot. Foot Ankle Int. 2004 Aug;25(8):545-9. PubMed PMID: 15363375. ](http://www.ncbi.nlm.nih.gov/pubmed/15363375)[View ](http://www.ncbi.nlm.nih.gov/pubmed/15363375)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15363375)
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 87
Figures 83a and 83b are the clinical photographs of a 42-year-old woman with a BMI of 31 who has had a 1-year history of right heel pain.
A
B
RECOMMENDED READINGS
[Dalla Paola L, Volpe A, Varotto D, Postorino A, Brocco E, Senesi A, Merico M, De Vido D, Da Ros R, Assaloni R. Use of a retrograde nail for ankle arthrodesis in Charcot neuroarthropathy: a limb salvage procedure. Foot Ankle Int. 2007 Sep;28(9):967-70. PubMed PMID: 17880869. ](http://www.ncbi.nlm.nih.gov/pubmed/17880869)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17880869)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17880869)
[Pinzur MS. Benchmark analysis of diabetic patients with neuropathic (Charcot) foot deformity. Foot Ankle Int. 1999 Sep;20(9):564-7. PubMed PMID: 10509683. ](http://www.ncbi.nlm.nih.gov/pubmed/10509683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10509683) [Pinzur M. Surgical versus accommodative treatment for Charcot arthropathy of the midfoot. Foot Ankle Int. 2004 Aug;25(8):545-9. PubMed PMID: 15363375. ](http://www.ncbi.nlm.nih.gov/pubmed/15363375)[View ](http://www.ncbi.nlm.nih.gov/pubmed/15363375)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15363375)
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 87
Figures 83a and 83b are the clinical photographs of a 42-year-old woman with a BMI of 31 who has had a 1-year history of right heel pain.
A
B
Question 83High Yield
Pain and tenderness at location 2 on Figures 83a and 83b is most consistent with which diagnosis?
Explanation
- Plantar fasciitis.
Question 84High Yield
What is the most appropriate initial diagnostic test for plantar heel pain?
Explanation
- Weight-bearing plain radiographs
Question 85High Yield
What is the strongest risk factor for plantar fasciitis?
Explanation
- BMI higher than 30
Question 86High Yield
What is the most reliable nonsurgical treatment for plantar fasciitis?
Explanation
- Plantar fascia stretching
Question 87High Yield
Which surgical procedure should be considered for treatment of chronic plantar fasciitis?
Explanation
Imaging studies in the evaluation of plantar fasciitis should always include weight-bearing foot radiographs to reveal alignment and exclude calcaneal stress fracture, tumor, subtalar arthritis, and insertional posterior spurs. MRI is occasionally indicated in problematic cases. Ultrasound can be helpful to evaluate thickening and disease in the proximal plantar fascia. Ultrasound is quick and much more cost effective than MRI. Laboratory screenings to evaluate inflammatory arthritis are indicated only for patients with bilateral heel pain who may be more likely to have systemic disease.
In the nonsurgical treatment of plantar fasciitis, high-impact loading exercises may make the condition worse. Corticosteroid injections may provide short-term relief only and can occasionally cause plantar fascia rupture. They should be used with caution. PRP injections are expensive and currently not covered by insurance. Studies have not demonstrated long-term pain relief with PRP. Plantar fascia-specific stretching has been shown more effective than Achilles tendon stretching alone.
Surgical treatment is indicated for fewer than 5% of patients. It is not necessary to resect the heel spur because the spur is not attached to the plantar fascia and rarely contributes to a patient's pain. The open extensile approach is associated with a much longer recovery than the open or endoscopic approaches and is no longer justified. Multiple studies have demonstrated the efficacy of endoscopic and open plantar fasciotomy techniques.
RECOMMENDED READINGS
Bader L, Park K, Gu Y, O'Malley MJ. Functional outcome of endoscopic plantar fasciotomy. Foot Ankle Int. 2012 Jan;33(1):37-43. doi: 10.3113/FAI.2012.0037. PubMed PMID:
[22381234.](http://www.ncbi.nlm.nih.gov/pubmed/22381234)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22381234)
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
[372/. PubMed PMID: 24860133.](http://www.ncbi.nlm.nih.gov/pubmed/24860133)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860133)
In the nonsurgical treatment of plantar fasciitis, high-impact loading exercises may make the condition worse. Corticosteroid injections may provide short-term relief only and can occasionally cause plantar fascia rupture. They should be used with caution. PRP injections are expensive and currently not covered by insurance. Studies have not demonstrated long-term pain relief with PRP. Plantar fascia-specific stretching has been shown more effective than Achilles tendon stretching alone.
Surgical treatment is indicated for fewer than 5% of patients. It is not necessary to resect the heel spur because the spur is not attached to the plantar fascia and rarely contributes to a patient's pain. The open extensile approach is associated with a much longer recovery than the open or endoscopic approaches and is no longer justified. Multiple studies have demonstrated the efficacy of endoscopic and open plantar fasciotomy techniques.
RECOMMENDED READINGS
Bader L, Park K, Gu Y, O'Malley MJ. Functional outcome of endoscopic plantar fasciotomy. Foot Ankle Int. 2012 Jan;33(1):37-43. doi: 10.3113/FAI.2012.0037. PubMed PMID:
[22381234.](http://www.ncbi.nlm.nih.gov/pubmed/22381234)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22381234)
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
[372/. PubMed PMID: 24860133.](http://www.ncbi.nlm.nih.gov/pubmed/24860133)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860133)
Question 88High Yield
A 45-year-old woman with grade II adult-acquired flatfoot deformity has pain on the lateral side of her foot just distal to the tip of the fibula. Which component of a comprehensive flatfoot reconstruction most likely will address the deformity responsible for this pain?
Explanation
Patients develop lateral ankle pain with progression of adult-acquired flatfoot deformity. This is associated with increased hindfoot valgus deformity. Calcaneal fibular impingement has been considered the primary cause of this pain. Studies demonstrate that arthrosis of the posterior facet of the subtalar joint strongly correlates with lateral pain in adult-acquired flatfoot deformity. Both conditions are related to hindfoot valgus deformity. Although lateral column lengthening is a powerful tool for correction of flatfoot deformity, its effect on hindfoot deformity is less defined. Lateral column lengthening provides better correction of the longitudinal arch of the midfoot and realignment of the medial column than other osteotomies. A medializing calcaneal osteotomy has a significant linear effect on hindfoot valgus alignment. Spring ligament reconstruction and medial cuneiform opening-wedge osteotomies have less effect on hindfoot alignment than the medial calcaneal slide.
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
[20460061/. ](http://www.ncbi.nlm.nih.gov/pubmed/20460061)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20460061)
[Chan JY, Williams BR, Nair P, Young E, Sofka C, Deland JT, Ellis SJ. The contribution of medializing calcaneal osteotomy on hindfoot alignment in the reconstruction of the stage II adult acquired flatfoot deformity. Foot Ankle Int.2013 Feb;34(2):159-66.doi: 10.1177/ 1071100712460225. Epub 2013 Jan 10. PubMed PMID: 23413053. ](http://www.ncbi.nlm.nih.gov/pubmed/23413053)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23413053)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23413053)
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
[20460061/. ](http://www.ncbi.nlm.nih.gov/pubmed/20460061)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20460061)
[Chan JY, Williams BR, Nair P, Young E, Sofka C, Deland JT, Ellis SJ. The contribution of medializing calcaneal osteotomy on hindfoot alignment in the reconstruction of the stage II adult acquired flatfoot deformity. Foot Ankle Int.2013 Feb;34(2):159-66.doi: 10.1177/ 1071100712460225. Epub 2013 Jan 10. PubMed PMID: 23413053. ](http://www.ncbi.nlm.nih.gov/pubmed/23413053)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23413053)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23413053)
Question 89High Yield
A
B
C
Figures 89a through 89c are the radiographs of a 35-year-old woman who has had 7 years of progressive ankle pain. She experiences stiffness and pain despite the use of an ankle-foot orthosis. Examination reveals pain along the anterior tibiotalar joint without tenderness to the subtalar or talonavicular joints. What is the most appropriate surgical intervention?
B
C
Figures 89a through 89c are the radiographs of a 35-year-old woman who has had 7 years of progressive ankle pain. She experiences stiffness and pain despite the use of an ankle-foot orthosis. Examination reveals pain along the anterior tibiotalar joint without tenderness to the subtalar or talonavicular joints. What is the most appropriate surgical intervention?



Explanation
This patient has isolated posttraumatic ankle arthritis with significantly decreased ankle range of motion that is best treated with an isolated ankle arthrodesis to eliminate pain. Because this patient is younger than 50 years of age and has limited presurgical range of motion, she is not a candidate for ankle arthroplasty. Additionally, TAA outcomes among patients who have a posttraumatic etiology are worse than for those with osteoarthritis. Tibiotalocalcaneal arthrodesis is suited for patients with associated subtalar
arthritis or rigid hindfoot deformity that necessitates correction. Anterior tibial exostectomy will not resolve the underlying arthritic pain and is not indicated.
RECOMMENDED READINGS
[Easley ME, Adams SB Jr, Hembree WC, DeOrio JK. Results of total ankle arthroplasty. J Bone Joint Surg Am. 2011 Aug 3;93(15):1455-68. doi: 10.2106/JBJS.J.00126. Review. PubMed PMID: 21915552. ](http://www.ncbi.nlm.nih.gov/pubmed/21915552)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21915552)
[Spirt AA, Assal M, Hansen ST Jr. Complications and failure after total ankle arthroplasty. J Bone Joint Surg Am. 2004 Jun;86-A(6):1172-8. PubMed PMID: 15173289. ](http://www.ncbi.nlm.nih.gov/pubmed/15173289)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/15173289)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15173289)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15173289)
[Ajis A, Henriquez H, Myerson M. Postoperative range of motion trends following total ankle arthroplasty. Foot Ankle Int. 2013 May;34(5):645-56. doi: 10.1177/1071100713481433. Epub 2013 Mar 11. PubMed PMID: 23478890. ](http://www.ncbi.nlm.nih.gov/pubmed/23478890)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23478890)
[Thomas R, Daniels TR, Parker K. Gait analysis and functional outcomes following ankle arthrodesis for isolated ankle arthritis. J Bone Joint Surg Am. 2006 Mar;88(3):526-35. PubMed PMID: 16510818. ](http://www.ncbi.nlm.nih.gov/pubmed/16510818)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16510818)
[Coester LM, Saltzman CL, Leupold J, Pontarelli W. Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am. 2001 Feb;83-A(2):219-28. PubMed PMID: 11216683. ](http://www.ncbi.nlm.nih.gov/pubmed/11216683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11216683)
arthritis or rigid hindfoot deformity that necessitates correction. Anterior tibial exostectomy will not resolve the underlying arthritic pain and is not indicated.
RECOMMENDED READINGS
[Easley ME, Adams SB Jr, Hembree WC, DeOrio JK. Results of total ankle arthroplasty. J Bone Joint Surg Am. 2011 Aug 3;93(15):1455-68. doi: 10.2106/JBJS.J.00126. Review. PubMed PMID: 21915552. ](http://www.ncbi.nlm.nih.gov/pubmed/21915552)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21915552)
[Spirt AA, Assal M, Hansen ST Jr. Complications and failure after total ankle arthroplasty. J Bone Joint Surg Am. 2004 Jun;86-A(6):1172-8. PubMed PMID: 15173289. ](http://www.ncbi.nlm.nih.gov/pubmed/15173289)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/15173289)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15173289)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15173289)
[Ajis A, Henriquez H, Myerson M. Postoperative range of motion trends following total ankle arthroplasty. Foot Ankle Int. 2013 May;34(5):645-56. doi: 10.1177/1071100713481433. Epub 2013 Mar 11. PubMed PMID: 23478890. ](http://www.ncbi.nlm.nih.gov/pubmed/23478890)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23478890)
[Thomas R, Daniels TR, Parker K. Gait analysis and functional outcomes following ankle arthrodesis for isolated ankle arthritis. J Bone Joint Surg Am. 2006 Mar;88(3):526-35. PubMed PMID: 16510818. ](http://www.ncbi.nlm.nih.gov/pubmed/16510818)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16510818)
[Coester LM, Saltzman CL, Leupold J, Pontarelli W. Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am. 2001 Feb;83-A(2):219-28. PubMed PMID: 11216683. ](http://www.ncbi.nlm.nih.gov/pubmed/11216683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11216683)
Question 90High Yield
Which structure is the primary stabilizer of the lesser metatarsophalangeal (MTP) joint?
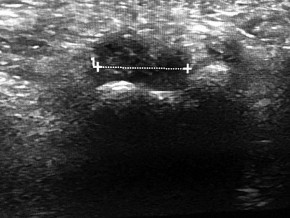


Explanation
Synovitis of the second MTP occurs in association with instability of the joint. This can be idiopathic or secondary to an external deforming force (such as a hallux valgus or shoe wear causing a claw toe). The primary stabilizer of the MTP joint for translation in the vertical plane is the plantar plate. The flexor digitorum brevis flexes the MTP joint, and the flexor digitorum longus flexes
all joints of the toe. The collateral ligaments are primary stabilizers in the transverse plane and secondary stabilizers in the sagittal plane.
RECOMMENDED READINGS
[Deland JT, Sung IH. The medial crosssover toe: a cadaveric dissection. Foot Ankle Int. 2000 May;21(5):375-8. PubMed PMID: 10830654.](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)
[Suero EM, Meyers KN, Bohne WH. Stability of the metatarsophalangeal joint of the lesser toes: a cadaveric study. J Orthop Res. 2012 Dec;30(12):1995-8. doi: 10.1002/jor.22173. Epub 2012 Jun 13. PubMed PMID: 22696467. ](http://www.ncbi.nlm.nih.gov/pubmed/22696467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22696467)
CLINICAL SITUATION FOR QUESTIONS 91 THROUGH 95
Figure 91a is the sagittal plane ultrasound of the second web space of a 48-year-old woman who has noted burning pain in the ball of her right foot for 2 years. The pain intermittently radiates into her second and the third toes. Figure 91b shows the surgical procedure and Figure 91c is the pathologic specimen.
A
B
C
all joints of the toe. The collateral ligaments are primary stabilizers in the transverse plane and secondary stabilizers in the sagittal plane.
RECOMMENDED READINGS
[Deland JT, Sung IH. The medial crosssover toe: a cadaveric dissection. Foot Ankle Int. 2000 May;21(5):375-8. PubMed PMID: 10830654.](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)
[Suero EM, Meyers KN, Bohne WH. Stability of the metatarsophalangeal joint of the lesser toes: a cadaveric study. J Orthop Res. 2012 Dec;30(12):1995-8. doi: 10.1002/jor.22173. Epub 2012 Jun 13. PubMed PMID: 22696467. ](http://www.ncbi.nlm.nih.gov/pubmed/22696467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22696467)
CLINICAL SITUATION FOR QUESTIONS 91 THROUGH 95
Figure 91a is the sagittal plane ultrasound of the second web space of a 48-year-old woman who has noted burning pain in the ball of her right foot for 2 years. The pain intermittently radiates into her second and the third toes. Figure 91b shows the surgical procedure and Figure 91c is the pathologic specimen.
A
B
C
Question 91High Yield
The cause of this patient's symptoms most likely is
Explanation
- interdigital neuroma.
Question 92High Yield
The most appropriate pedorthic management of symptomatic interdigital neuroma involves
Explanation
- a metatarsal pad.
Question 93High Yield
Open or endoscopic decompression of interdigital neuroma is predicated on the hypothesis that interdigital neuromas represent a compression neuropathy from which anatomic structure?
Explanation
- Intermetatarsal ligament
Question 94High Yield
The primary advantage of the plantar approach for resection of interdigital neuromas is
Explanation
- better access to the neuroma.
Question 95High Yield
The most common complication associated with corticosteroid injection for the treatment of interdigital neuroma is

Explanation
Interdigital neuromas represent perineural fibrosis of the intermetatarsal nerve most commonly seen in the second and third web spaces. The photographs depict a neuroma in the second web space, which is less common than in the third space. Its hypoechoic appearance is characteristic on ultrasound. PVNS occurs in joints. Lipomas are fatty tumors. A ganglion cyst can occasionally occur adjacent to a nerve, but it has a cystic appearance.
The most popular theory on the etiology of interdigital neuromas is compression neuropathy by the intermetatarsal ligament. The plantar approach for the resection of interdigital neuromas has become more popular, especially for recurrent neuromas. The major advantage is better visualization and access to the neuromas.
Infection and allergic reactions such as hives are rare after steroid injection. CRPS is not known to occur in this setting. Hammertoe formation can occur, especially after multiple steroid injections into an interdigital neuroma.
RECOMMENDED READINGS
Schon LC, Reed MA. Disorder of the nerves. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014:622-641.
[Gauthier G. Thomas Morton's disease: a nerve entrapment syndrome. A new surgical technique. Clin Orthop Relat Res. 1979 Jul-Aug;(142):90-2. PubMed PMID: 498653. ](http://www.ncbi.nlm.nih.gov/pubmed/498653)[View](http://www.ncbi.nlm.nih.gov/pubmed/498653)[ ](http://www.ncbi.nlm.nih.gov/pubmed/498653)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/498653)
CLINICAL SITUATION FOR QUESTIONS 96 THROUGH 98
Figure 96 is the anteroposterior projection foot radiograph of a 35-year-old woman who is injured in a high-speed motorcycle collision. Her assessment reveals an isolated injury. Her pulses are palpable and her neuromotor examination is intact. There is tenting of skin with ecchymosis over the second metatarsal. The foot is extremely swollen but not tense. Passive toe range of motion is painless.
The most popular theory on the etiology of interdigital neuromas is compression neuropathy by the intermetatarsal ligament. The plantar approach for the resection of interdigital neuromas has become more popular, especially for recurrent neuromas. The major advantage is better visualization and access to the neuromas.
Infection and allergic reactions such as hives are rare after steroid injection. CRPS is not known to occur in this setting. Hammertoe formation can occur, especially after multiple steroid injections into an interdigital neuroma.
RECOMMENDED READINGS
Schon LC, Reed MA. Disorder of the nerves. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014:622-641.
[Gauthier G. Thomas Morton's disease: a nerve entrapment syndrome. A new surgical technique. Clin Orthop Relat Res. 1979 Jul-Aug;(142):90-2. PubMed PMID: 498653. ](http://www.ncbi.nlm.nih.gov/pubmed/498653)[View](http://www.ncbi.nlm.nih.gov/pubmed/498653)[ ](http://www.ncbi.nlm.nih.gov/pubmed/498653)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/498653)
CLINICAL SITUATION FOR QUESTIONS 96 THROUGH 98
Figure 96 is the anteroposterior projection foot radiograph of a 35-year-old woman who is injured in a high-speed motorcycle collision. Her assessment reveals an isolated injury. Her pulses are palpable and her neuromotor examination is intact. There is tenting of skin with ecchymosis over the second metatarsal. The foot is extremely swollen but not tense. Passive toe range of motion is painless.
Question 96High Yield
The most appropriate urgent orthopaedic intervention involves
Explanation
- urgent closed reduction and splinting with serial compartment checks.
Question 97High Yield
Six months after surgical repair, the patient reports that when tapping over her central midfoot incision, paresthesias to the third and fourth toes occur. What is the most likely diagnosis?
Explanation
- Neuritis of the superficial peroneal nerve
Question 98High Yield
The patient returns 1 year later to report curling of her toes and numbness on the plantar surface of her foot. What is the most likely cause of this condition?
Explanation
Radiographs reveal a Lisfranc fracture dislocation with fractures of the first and second metatarsals. Tenting of skin that is over a bony prominence is an orthopaedic emergency. The fracture dislocation should be reduced without delay. There is no evidence of compartment syndrome of the foot, but this may develop and monitoring is necessary. Toe deformity may develop on a delayed basis because of the subclinical presentation. Nerve irritation is not uncommon with dorsal midfoot surgical incisions. A positive Tinel test result over the midfoot in the distribution of the superficial common peroneal nerve is consistent with a stretch injury to this nerve. CRPS is usually associated with multiple nerve distributions and autonomic nerve findings such as cold hypersensitivity and hyperhidrosis.
RECOMMENDED READINGS
[Benirschke SK, Meinberg EG, Anderson SA, Jones CB, Cole PA. Fractures and dislocations of the midfoot: Lisfranc and Chopart injuries. Instr Course Lect. 2013;62:79-91. PubMed PMID: 23395016. ](http://www.ncbi.nlm.nih.gov/pubmed/23395016)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23395016)
Schepers T, Oprel PP, Van Lieshout EM. Influence of approach and implant on reduction accuracy and stability in lisfranc fracture-dislocation at the tarsometatarsal joint. Foot Ankle Int. 2013 May;34(5):705-10. doi: 10.1177/1071100712468581. Epub 2013 Jan 14. PubMed
[PMID: 23637239. ](http://www.ncbi.nlm.nih.gov/pubmed/23637239)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23637239)
RECOMMENDED READINGS
[Benirschke SK, Meinberg EG, Anderson SA, Jones CB, Cole PA. Fractures and dislocations of the midfoot: Lisfranc and Chopart injuries. Instr Course Lect. 2013;62:79-91. PubMed PMID: 23395016. ](http://www.ncbi.nlm.nih.gov/pubmed/23395016)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23395016)
Schepers T, Oprel PP, Van Lieshout EM. Influence of approach and implant on reduction accuracy and stability in lisfranc fracture-dislocation at the tarsometatarsal joint. Foot Ankle Int. 2013 May;34(5):705-10. doi: 10.1177/1071100712468581. Epub 2013 Jan 14. PubMed
[PMID: 23637239. ](http://www.ncbi.nlm.nih.gov/pubmed/23637239)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23637239)
Question 99High Yield
Figure 99 is the radiograph of an 18-year-old National Collegiate Athletic Association Division I basketball player who jumped for a basket. After
landing, he was unable to put weight on his left great toe. He developed pain, swelling, and ecchymosis maximally around the sesamoids. When assessing stability of the first metatarsophalangeal joint, he appears to have more laxity on the left. What is the best next step?
landing, he was unable to put weight on his left great toe. He developed pain, swelling, and ecchymosis maximally around the sesamoids. When assessing stability of the first metatarsophalangeal joint, he appears to have more laxity on the left. What is the best next step?

Explanation
This patient jumped on his forefoot and landed with pain in his great toe. His radiograph shows possible increased space between the sesamoids and the base of the phalanx. A comparison radiograph on the other side will reveal if this position is normal for this patient. If findings are asymmetric, turf toe injury is a possibility based on this patient's symptoms and mechanism of injury.
RECOMMENDED READINGS
[Waldrop NE 3rd, Zirker CA, Wijdicks CA, Laprade RF, Clanton TO. Radiographic evaluation of plantar plate injury: an in vitro biomechanical study. Foot Ankle Int. 2013 Mar;34(3):403-8. doi: 10.1177/1071100712464953. Epub 2013 Jan 14. PubMed PMID: 23520299. ](http://www.ncbi.nlm.nih.gov/pubmed/23520299)[View](http://www.ncbi.nlm.nih.gov/pubmed/23520299)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23520299)
[McCormick JJ, Anderson RB. The great toe: failed turf toe, chronic turf toe, and complicated sesamoid injuries. Foot Ankle Clin. 2009 Jun;14(2):135-50. doi: 10.1016/j.fcl.2009.01.001. Review. PubMed PMID: 19501799. ](http://www.ncbi.nlm.nih.gov/pubmed/19501799)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19501799)
RECOMMENDED READINGS
[Waldrop NE 3rd, Zirker CA, Wijdicks CA, Laprade RF, Clanton TO. Radiographic evaluation of plantar plate injury: an in vitro biomechanical study. Foot Ankle Int. 2013 Mar;34(3):403-8. doi: 10.1177/1071100712464953. Epub 2013 Jan 14. PubMed PMID: 23520299. ](http://www.ncbi.nlm.nih.gov/pubmed/23520299)[View](http://www.ncbi.nlm.nih.gov/pubmed/23520299)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23520299)
[McCormick JJ, Anderson RB. The great toe: failed turf toe, chronic turf toe, and complicated sesamoid injuries. Foot Ankle Clin. 2009 Jun;14(2):135-50. doi: 10.1016/j.fcl.2009.01.001. Review. PubMed PMID: 19501799. ](http://www.ncbi.nlm.nih.gov/pubmed/19501799)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19501799)
Question 100High Yield
Video 100 is the presurgical lateral ankle examination of a 45-year-old woman who has had pain and discomfort for 2 years along the posterolateral ankle following a sudden dorsiflexion injury. She notes occasional clicking and popping, and she has not experienced resolution of her symptoms despite immobilization and physical therapy. Examination reveals a stable ankle-to-anterior drawer and inversion stress testing. No strength deficit is noted, but
she has apprehension with resisted eversion. MR images do not reveal evidence of tendonosis or tear. The most appropriate surgical intervention is
she has apprehension with resisted eversion. MR images do not reveal evidence of tendonosis or tear. The most appropriate surgical intervention is




Explanation
This patient has a clear history of dorsiflexion injury complicated by chronic peroneal tendon dislocation. The symptoms and findings are consistent with dislocation in this particular case. Groove deepening of the posterior fibula with associated imbrication of the peroneal retinaculum is the most effective surgical procedure. Associated synovitis or tendonosis should be addressed. However, failure to deepen the groove and imbricate the retinaculum will result in continued discomfort. Consequently, both responses that involve isolated tendon surgery are not appropriate. Associated subjective instability can be noted in these patients. The examination is critical to determine the stability of the lateral collateral complex, which is intact in this case (so
imbrication is not indicated). A sense of apprehension is a common examination finding because patients sense that the peroneals will subluxate with resisted eversion. Placement of the examiner's hands on the peroneals to stabilize the tendons should relieve this apprehension. A patient may not be able to voluntarily dislocate the tendon. Dynamic ultrasound is the most sensitive radiographic examination for detection of dislocation. Intrasheath peroneal subluxation may also occur and is treated similarly.
RECOMMENDED READINGS
Raikin SM. Intrasheath subluxation of the peroneal tendons. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:146-55. doi: 10.2106/JBJS.H.01356. PubMed PMID:
[19255207.](http://www.ncbi.nlm.nih.gov/pubmed/19255207)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19255207)
[Philbin TM, Landis GS, Smith B. Peroneal tendon injuries. J Am Acad Orthop Surg. 2009 May;17(5):306-17. Review. PubMed PMID: 19411642. ](http://www.ncbi.nlm.nih.gov/pubmed/19411642)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19411642)
[Ogawa BK, Thordarson DB. Current concepts review: peroneal tendon subluxation and dislocation. Foot Ankle Int. 2007 Sep;28(9):1034-40. Review. PubMed PMID: 17880883. ](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[View](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17880883)
This is the last question of the exam.
imbrication is not indicated). A sense of apprehension is a common examination finding because patients sense that the peroneals will subluxate with resisted eversion. Placement of the examiner's hands on the peroneals to stabilize the tendons should relieve this apprehension. A patient may not be able to voluntarily dislocate the tendon. Dynamic ultrasound is the most sensitive radiographic examination for detection of dislocation. Intrasheath peroneal subluxation may also occur and is treated similarly.
RECOMMENDED READINGS
Raikin SM. Intrasheath subluxation of the peroneal tendons. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:146-55. doi: 10.2106/JBJS.H.01356. PubMed PMID:
[19255207.](http://www.ncbi.nlm.nih.gov/pubmed/19255207)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19255207)
[Philbin TM, Landis GS, Smith B. Peroneal tendon injuries. J Am Acad Orthop Surg. 2009 May;17(5):306-17. Review. PubMed PMID: 19411642. ](http://www.ncbi.nlm.nih.gov/pubmed/19411642)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19411642)
[Ogawa BK, Thordarson DB. Current concepts review: peroneal tendon subluxation and dislocation. Foot Ankle Int. 2007 Sep;28(9):1034-40. Review. PubMed PMID: 17880883. ](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[View](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17880883)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17880883)
This is the last question of the exam.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon