Operative Management of Metatarsophalangeal Joint Instability and Lesser Toe Deformities
Key Takeaway
Metatarsophalangeal (MTP) joint instability is a progressive disorder commonly affecting the second ray, driven by attritional degeneration of the plantar plate and collateral ligaments. This comprehensive guide details the biomechanical etiology, clinical evaluation including the Lachman test, and evidence-based surgical management. Key interventions include synovectomy, plantar plate repair, and the flexor-to-extensor (Girdlestone-Taylor) tendon transfer to restore dynamic stability and correct lesser toe deformities.
Introduction to Lesser Toe Abnormalities
Deformities of the lesser toes—encompassing hammer toe, claw toe, mallet toe, and crossover toe—are among the most common pathologies encountered in foot and ankle surgery. While these conditions present with varying degrees of sagittal and coronal plane deformity, they frequently share a common pathophysiological denominator: metatarsophalangeal (MTP) joint instability.
Historically viewed as isolated digital deformities, modern orthopedic consensus recognizes that lesser toe abnormalities represent a complex continuum of capsuloligamentous failure. This disorder ranges in severity from mild, reversible synovitis of the MTP joint to chronic, fixed dislocation and severe multi-planar deformity. Understanding the intricate biomechanics and progressive nature of this instability is paramount for orthopedic surgeons to execute effective, durable reconstructions.
Etiology and Pathophysiology
The etiology of MTP joint instability is multifactorial, heavily influenced by both intrinsic anatomical predispositions and extrinsic mechanical forces. The second MTP joint is overwhelmingly the most common site of synovitis, instability, and subsequent fixed deformity.
Anatomical Predispositions
A primary anatomical driver is the presence of a long second metatarsal (often referred to as a Morton's foot type). Studies indicate that a disproportionately long second metatarsal is present in up to 90% of patients with second MTP joint instability, averaging 4 mm in excessive length compared to the first metatarsal. This length discrepancy subjects the second MTP joint to exponentially higher peak plantar pressures during the terminal stance phase of gait.
Extrinsic Factors
Lesser toe deformities are highly prevalent in two distinct patient populations:
1. Women wearing constrictive, high-heeled footwear: High heels force the MTP joints into chronic hyperextension, bowstringing the flexor tendons and placing continuous tensile stress on the plantar plate.
2. Athletes experiencing chronic overuse: Repetitive hyperextension injuries (e.g., "turf toe" variants of the lesser toes) lead to microtrauma and attritional failure of the static restraints.
Clinical Pearl: While hallux valgus is frequently associated with second MTP joint instability, the instability is primarily driven by attritional changes in the lateral collateral ligament, capsule, and plantar plate due to chronic synovitis, rather than direct mechanical pressure from the deviated hallux.
Other systemic and traumatic causes include chronic synovitis secondary to inflammatory arthropathies (e.g., rheumatoid arthritis), neuromuscular diseases causing intrinsic-extrinsic muscular imbalance, and acute traumatic disruptions of the plantar plate and collateral ligaments.
Anatomy and Biomechanics
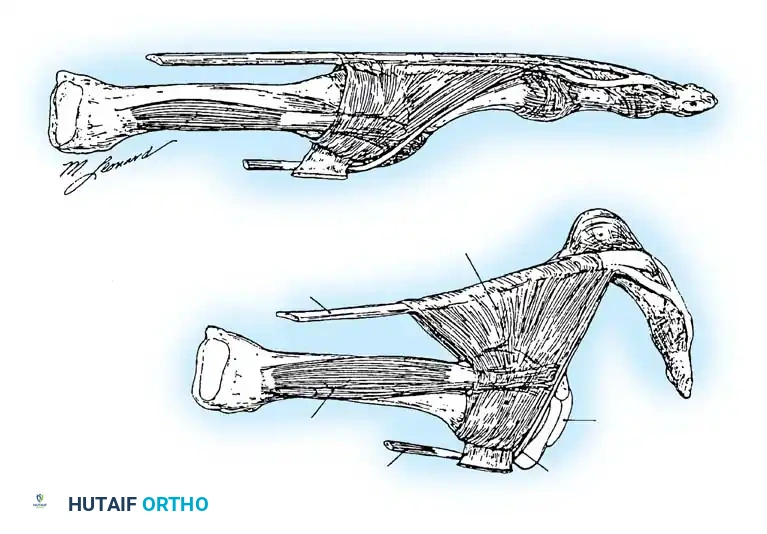
Normal lesser toe kinematics depend on a delicate equilibrium between dynamic musculotendinous forces and static capsuloligamentous restraints.
Dynamic Restraints
The most powerful extension force on the MTP joint is delivered by the extensor digitorum longus (EDL) tendon. The EDL extends the MTP joint through a fibroaponeurotic sling that attaches plantarly to the plantar plate and capsule, effectively suspending the proximal phalanx.
Crucially, the EDL can only extend the interphalangeal (IP) joints when the MTP joint is in a neutral or flexed position. If the toe is held in chronic extension (e.g., by high-heeled shoes), the EDL loses its mechanical advantage at the IP joints and becomes a pure deforming force, exacerbating MTP hyperextension.
Flexion of the MTP joint is primarily governed by the intrinsic muscles (lumbricals and interossei). The second toe possesses a unique anatomical vulnerability: it has two dorsal interossei and zero plantar interossei.
Normally, the axis of pull for these intrinsic muscles is plantar to the center of rotation of the MTP joint. However, as the MTP joint becomes chronically extended, the line of action shifts dorsal to the center of rotation. Consequently, these tendons paradoxically become deforming forces that drive further dorsal subluxation.
Furthermore, the lumbrical muscle, located on the medial side of the joint, acts as an unopposed adductor. While it normally passes plantar to the deep transverse intermetatarsal ligament to act as a plantar flexor, chronic extension renders it ineffective in the sagittal plane, allowing it to drive medial deviation (crossover toe deformity).
Static Restraints
The primary static stabilizers of the MTP joint are the collateral ligaments and the plantar plate. The plantar plate is a robust, fibrocartilaginous structure that originates on the metatarsal neck and inserts firmly into the plantar base of the proximal phalanx. Chronic joint irritation, effusion, and synovitis cause attritional degeneration, lengthening, and eventual rupture of these structures—most notably the lateral collateral ligament and the distal insertion of the plantar plate.
Clinical Evaluation and Diagnosis
Patient History
Patients typically present with an insidious, slowly progressive course of metatarsalgia, exacerbated by weight-bearing and constrictive footwear. A pathognomonic complaint is the sensation of "walking on a marble" beneath the affected metatarsal head.
Neuritic symptoms may radiate into the second and third toes, mimicking a Morton's neuroma. It is critical to differentiate between second MTP joint synovitis and a second web space neuroma, though the two can occasionally coexist. Athletes may recall a specific acute hyperextension injury that initiated the pain cycle. As the condition advances, pain may occur even at rest.
Physical Examination
Visual inspection may reveal a flexible or fixed hammer toe, claw toe, or medial crossover deformity. Swelling of the MTP joint is often manifested by the loss of the visible contour of the long extensor tendon compared to adjacent toes. A palpable joint effusion is frequently present.
Palpation reveals localized tenderness over the dorsofibular aspect of the joint (indicating lateral collateral ligament attenuation) or directly beneath the metatarsal head, just proximal to the joint line (indicating plantar plate pathology). As the proximal phalanx subluxates dorsally, the metatarsal head is driven plantarly, often resulting in a painful intractable plantar keratosis (callus).

The Lachman Test of the MTP Joint
The most reliable clinical assessment for dorsal-plantar instability is the MTP joint Lachman test, as described by Thompson and Hamilton.
Technique:
1. The examiner stabilizes the metatarsal neck with one hand.
2. The other hand grasps the base of the proximal phalanx.
3. A dorsal-to-plantar translation force is applied.
4. The degree of dorsal translation is compared to the contralateral, asymptomatic toe.
A positive test yields visible and palpable dorsal subluxation, often reproducing the patient's pain. Joint motion is typically limited, especially in plantar flexion.



Imaging
Weight-bearing anteroposterior (AP) and lateral radiographs are essential. Findings may include a long second metatarsal, widening of the MTP joint space (indicating effusion), or frank dorsal and medial subluxation.
While the diagnosis is primarily clinical, Magnetic Resonance Imaging (MRI) utilizing a small receiver coil (as described by Yao et al.) is highly sensitive and specific for evaluating the integrity of the plantar plate and collateral ligaments.
Non-Operative Management
In the early stages of synovitis (Grade 0 or 1 instability) with minimal deformity, conservative management is highly effective. Trepman and Yeo demonstrated that a majority of patients treated non-operatively do not require surgical intervention.
Conservative Modalities Include:
* Immobilization and Taping: Taping the toe in a neutral or slightly plantarflexed position (e.g., cross-over taping) relieves tension on the plantar plate.
* Orthotics: Custom orthoses with a metatarsal pad placed proximal to the metatarsal heads offload the affected joint. The addition of a rigid Morton's extension or a spring steel plate to the sole eliminates extension forces during toe-off.
* Pharmacotherapy: Oral NSAIDs and a single intra-articular corticosteroid injection can rapidly diminish acute synovitis.
Surgical Warning: Repeated corticosteroid injections are contraindicated, as they accelerate the attritional rupture of the plantar plate and collateral ligaments.
Surgical Management
When significant deformity or instability is present, or when conservative measures fail, surgical intervention is warranted. The choice of procedure is dictated by the degree of instability and the flexibility of the deformity.
Soft Tissue Procedures
For chronic synovitis without frank instability, an extensor longus lengthening, dorsal capsulotomy, and synovectomy may suffice. If preoperative evaluation strongly suggests concurrent neuritic pain, a second web space neuroma should be explored and resected.
If the joint subluxates more than 50% dorsally, a stabilizing procedure must be added. Direct anatomical repair of the plantar plate to the base of the proximal phalanx via a plantar or dorsal approach has gained significant popularity. However, in cases of severe attenuation or chronic flexible deformity, dynamic stabilization via tendon transfer is highly reliable.
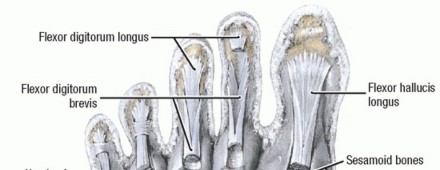
The Flexor-to-Extensor Transfer (Girdlestone-Taylor Procedure)
Originally described for flexible hammer toes, the transfer of the flexor digitorum longus (FDL) to the extensor mechanism is exceptionally effective at providing dynamic plantarflexion stability to an incompetent MTP joint. By rerouting the FDL dorsally, the procedure converts a flexor of the distal interphalangeal (DIP) joint into a dynamic plantar flexor of the MTP joint.
Clinical Pearl: If a severe intractable plantar keratosis is present, performing a concurrent plantar condylectomy of the metatarsal head removes the bony prominence, provides a bleeding cancellous bed for plantar plate healing, and adds static stability to the joint.
Operative Technique: Step-by-Step
1. Proximal Plantar Exposure
* On the affected toe, make a transverse plantar incision directly over the proximal flexion crease of the digit. Extreme care must be taken to preserve the neurovascular bundles located laterally and medially.
* Retract the skin and subcutaneous tissues using small hooked retractors to expose the underlying flexor tendon sheath.
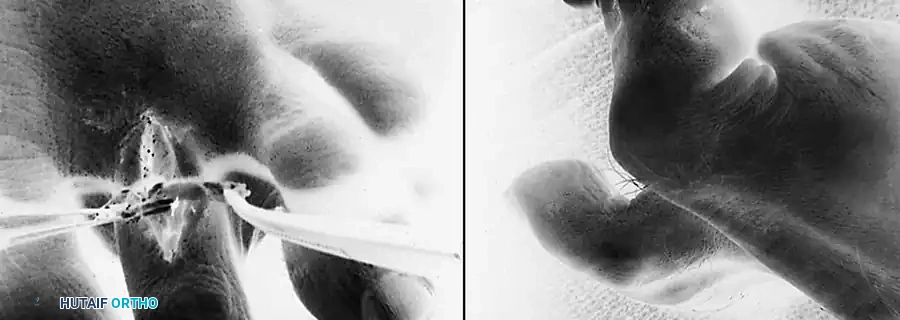
2. Tendon Identification and Release
* Open the proximal 3 to 4 mm of the fibrous pulley to expose the FDL tendon. This is best achieved by incising the pulley along its lateral border and reflecting it. Magnification loupes and a small round-end blade facilitate this delicate dissection.
* Topographically, this exposure is located at the middle third of the proximal phalanx.
* Identify the central tendon as the FDL. Confirm this by applying gentle, passive flexion and extension to the DIP joint while holding the proximal interphalangeal (PIP) joint in full extension.
* Elevate the FDL tendon. The vinculum longum will appear under tension; sever it using electrocautery to mobilize the tendon.
3. Distal Tenotomy
* Make a second transverse plantar incision at the level of the DIP joint.
* Perform a complete tenotomy of the FDL at its insertion, ensuring the plantar plate of the DIP joint is not violated.
4. Tendon Delivery and Splitting
* Return to the proximal incision. Hook the FDL tendon with a small hemostat (do not clamp the tendon substance) and deliver the distal segment into the proximal wound. Tenacious vincula may require gentle blunt force to release.
* Inspect the wound to ensure the two lateral slips of the flexor digitorum brevis (FDB) remain intact.
* Inspect the delivered FDL tendon to identify the shallow, linear furrow running longitudinally along its plantar surface.
* Using small forceps, hold one side of the free end while an assistant holds the other. Split the tendon longitudinally along this natural cleavage plane for 1.5 to 2.5 cm.
* Surgical Tip: Pull the tendon distally while plantarflexing the ankle. This provides optimal visualization of both sides of the tendon, preventing inadvertent complete sectioning of one half. Use the very tips of straight tenotomy scissors in the axilla of the split.
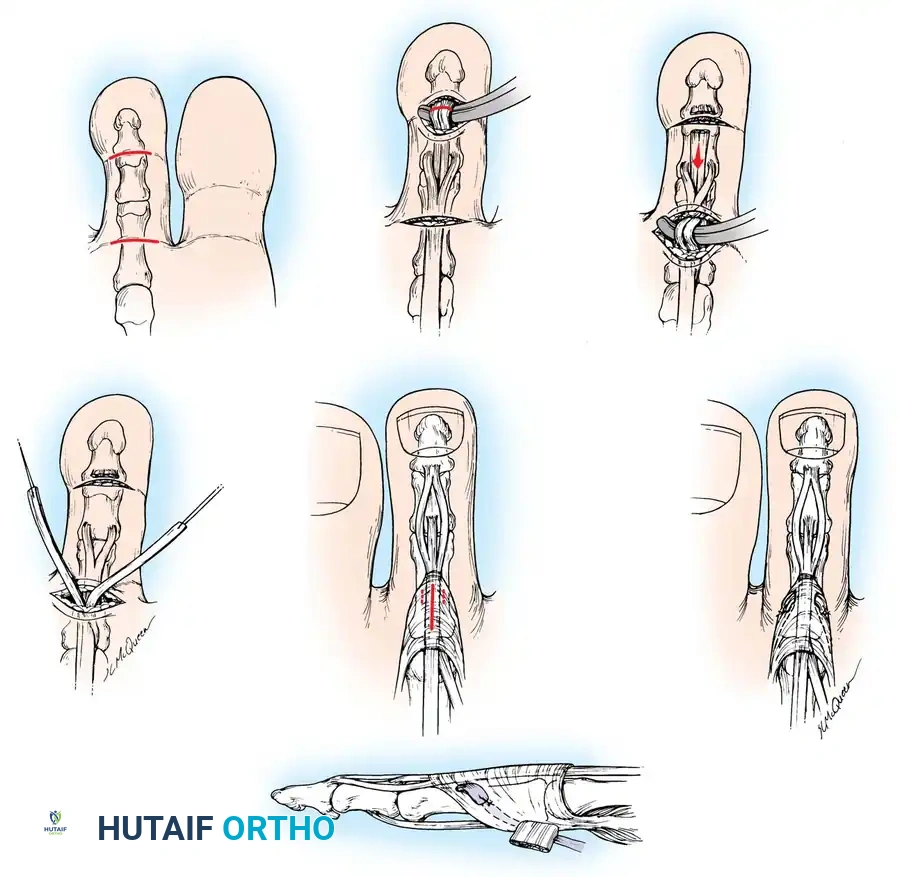
5. Dorsal Routing and Fixation
* Moisten the split tendon slips with sterile saline.
* Make a 1.5 to 2 cm longitudinal midline incision on the dorsum of the proximal phalanx. Carefully identify and retract or cauterize the dorsal digital veins.
* By sharp dissection, identify the trailing edge of each lateral band of the extensor mechanism while the skin is retracted, including the dorsal hood aponeurosis, to prepare for the routing of the split flexor tendon slips.
* Using a curved hemostat, create a tunnel passing from the dorsal incision, around the medial and lateral borders of the proximal phalanx, to the proximal plantar incision.
* Grasp the respective slips of the split FDL tendon and pull them dorsally. The slips should embrace the proximal phalanx like a sling.
6. Tensioning and Suturing
* With the ankle held in a neutral (90-degree) position, hold the MTP joint in approximately 10 to 15 degrees of plantar flexion.
* Overlap the two slips of the FDL tendon over the dorsal aspect of the proximal phalanx and the extensor mechanism.
* Suture the slips to each other and to the extensor aponeurosis using non-absorbable or slowly absorbable sutures (e.g., 3-0 or 4-0 braided polyester).
* Ensure the tension is sufficient to hold the MTP joint in slight plantarflexion without manual support.
* If concurrent bony procedures (such as a Weil osteotomy or PIP arthrodesis) are performed, a smooth 0.045-inch Kirschner wire may be driven retrogradely across the PIP and MTP joints to maintain alignment during the initial healing phase.
Postoperative Protocol and Rehabilitation
Meticulous postoperative care is critical to prevent stiffness and ensure the longevity of the dynamic transfer.
- Weeks 0-3: The patient is placed in a rigid, flat-bottom postoperative shoe and allowed heel-weight-bearing only. The toe is maintained in a bulky compressive dressing, splinted in slight plantarflexion. If a K-wire was utilized, it remains in place.
- Weeks 3-4: The K-wire (if present) is removed in the clinic. The patient transitions to full weight-bearing in a stiff-soled shoe.
- Weeks 4-6: Aggressive physical therapy is initiated. Active and passive range of motion exercises focus on MTP joint plantarflexion. Dorsal extension is strictly limited to prevent stretching of the tendon transfer. The toe is continuously taped in plantarflexion using a buddy-tape or crossover taping technique.
- Weeks 6+: The patient may gradually transition to standard, wide-toe-box footwear. Taping may be discontinued once dynamic plantarflexion strength is clinically evident and the toe rests in a neutral sagittal alignment.
Complications and Pitfalls
While the flexor-to-extensor transfer is highly successful, surgeons must be vigilant regarding potential complications:
- "Floating Toe" Deformity: The most common complication, resulting from inadequate tensioning of the tendon transfer or failure to address a severely elongated metatarsal (failure to perform a concurrent Weil osteotomy). The toe fails to purchase the ground during the stance phase.
- MTP Joint Stiffness: Over-tensioning the transfer or prolonged K-wire fixation can lead to a rigid, plantarflexed MTP joint, causing a new focal pressure point at the tip of the toe.
- Neurovascular Injury: The digital neurovascular bundles are highly vulnerable during the plantar dissection and the creation of the medial/lateral routing tunnels. Blind passage of instruments must be avoided.
- Recurrence: Failure to address the primary etiology (e.g., continuing to wear high-heeled shoes or ignoring a massive hallux valgus deformity) will inevitably lead to stretching of the transfer and recurrence of the instability.
By adhering to strict biomechanical principles, executing meticulous surgical technique, and
You Might Also Like