Preoperative Management and Surgical Decision-Making in Hallux Valgus Reconstruction
Key Takeaway
Preoperative management of hallux valgus requires a comprehensive clinical and radiographic evaluation. Surgeons must assess the entire foot, including lesser toe deformities and hindfoot alignment, to formulate an effective surgical plan. Treatment algorithms depend on deformity severity, joint congruency, and first ray mobility. This guide details evidence-based protocols, angular measurements, and step-by-step surgical decision-making for optimal outcomes in forefoot reconstruction.
PREOPERATIVE MANAGEMENT OF HALLUX VALGUS AND HALLUX RIGIDUS
The preoperative management of hallux valgus and hallux rigidus demands a meticulous, systematic approach. Forefoot reconstruction is highly nuanced; no single procedure universally corrects all variants of first ray pathology. The orthopaedic surgeon must synthesize clinical findings, patient expectations, and precise radiographic measurements to select the optimal surgical intervention. No procedure should be recommended until the entire foot—not merely the first ray—is thoroughly examined.
Comprehensive Clinical Evaluation
The clinical examination must be conducted with the patient in multiple positions: standing (weight-bearing), sitting, and lying supine and prone (if practical). Weight-bearing examination is paramount, as the biomechanical loads of stance often unmask the true severity of the deformity, including dynamic hypermobility of the first tarsometatarsal (TMT) joint and collapse of the medial longitudinal arch.
Particular attention must be directed to the remainder of the forefoot. The surgeon must systematically identify associated pathologies, including:
* Corns and intractable plantar keratoses (IPKs)
* Calluses and warts
* Interdigital (Morton's) neuromas
* Bunionettes (Tailor's bunions)
* Hammer toes, claw toes, and mallet toes
Clinical Pearl: Although pain and deformity at the first metatarsophalangeal (MTP) joint may be successfully relieved after correction of the hallux valgus, the overall clinical result can be severely marred if symptoms in the lesser toes or the central metatarsals remain unaddressed.
Patients frequently present with a primary complaint that is not the severe hallux valgus deformity itself, but rather transfer metatarsalgia or pain beneath the second metatarsal head due to a crossover toe deformity.

This phenomenon must be explained carefully to the patient before surgery to avoid false expectations and postoperative disappointment. Finally, the midfoot and hindfoot must be examined carefully. Conditions such as adult-acquired flatfoot deformity (posterior tibial tendon dysfunction) or Achilles contracture can exert profound deforming forces on the forefoot, predisposing the patient to recurrence if not concurrently managed.
Nonoperative Management
Initially, the vast majority of patients can and should be treated nonoperatively. The cornerstone of conservative management includes:
* Shoe Modifications: Wide toe-box footwear, soft upper materials, and avoidance of high heels.
* Orthoses: Custom or over-the-counter inserts with metatarsal pads to offload transfer lesions.
* Activity Adjustments: Modification of high-impact activities.
* Physical Therapy: Achilles stretching and intrinsic muscle strengthening.
Surgical Warning: Operative treatment of hallux valgus for purely cosmetic reasons is seldom indicated. The exception may be an adolescent with a significant, rapidly progressive deformity. However, even the mildest symptoms in an adolescent often worsen, especially in the presence of a strong family history. Correction of juvenile or adolescent hallux valgus is notoriously difficult, carries a high recurrence rate, and is often disappointing.
Biomechanics and Anatomical Considerations
Any surgical procedure chosen must account for the primary structural components of the deformity:
1. Valgus deviation and pronation of the great toe (hallux valgus).
2. Varus deviation of the first metatarsal (metatarsus primus varus).
Furthermore, the surgeon must identify anatomical variants that could compromise a technically well-done procedure:
* Os Intermetatarseum: The presence of an accessory bone between the bases of the first and second metatarsals might preclude the effectiveness of a soft-tissue procedure alone, as it physically blocks the lateral translation of the first metatarsal base required to reduce the intermetatarsal angle.
* Accessory Sesamoids and Prominent Ungual Tuberosities: These structures at the interphalangeal (IP) joint contribute to painful callosities at the tibial side of the joint.
* Os Tibialis Externum: Frequently associated with excessive hallux valgus interphalangeus and loss of medial column support.
* Metatarsus Adductus: Varus of the first metatarsal might be a significant part of the overall foot deformity even with an intermetatarsal angle (IMA) of less than 10 degrees. Metatarsus adductus combined with a relatively small hallux valgus angle (HVA) of 15 to 20 degrees may produce significant clinical deformity, necessitating a modified surgical approach.
Radiographic Evaluation and Angular Measurements
Standardized weight-bearing radiographs (anteroposterior, lateral, and sesamoid axial views) are mandatory. The usefulness of computer-assisted versus manual measurement of the IMA, HVA, and distal metatarsal articular angle (DMAA) has been a subject of extensive academic debate.
Both manual and digital methods demonstrate closer interobserver and intraobserver correlation in the measurement of the IMA and HVA than in the measurement of the DMAA. However, the reliability of either method has a wide range (up to 5 degrees). Therefore, while these measurements are vital guides, they do not provide a completely infallible indication of the magnitude of deformity.
Schneider et al. highlighted the critical importance of reference points, reporting two distinct methods for determining angular measurements:
1. Mid-diaphyseal Technique: Utilizing the longitudinal axis of the first metatarsal based on mid-diaphyseal reference points.
2. Center-head Technique: Utilizing the center of the articular surface (center head) and the center of the proximal diaphysis (center base).
They found that the measured correction of the HVA and IMA varied by approximately 9 degrees depending on which reference points were used.
To standardize this, the American Orthopaedic Foot and Ankle Society (AOFAS) Ad Hoc Committee on Angular Measurements (Coughlin, Saltzman, and Nunley) recommended:
* Standardized weight-bearing radiographic technique.
* Specific, consistent placement of reference points.
* Use of a protractor rather than a standard goniometer for manual measurements.
* Following distal osteotomies, dual measurements using a center-head technique and a Mose sphere.
More recently, Farber et al. determined that computer-assisted angle measurement on digital radiographs provides significantly more reliable results than goniometers on plain films, improving inter- and intra-observer agreement from 66% to 80%.
SURGICAL DECISION-MAKING ALGORITHM
The selection of the appropriate operative intervention is dictated by the severity of the deformity (HVA and IMA), the congruency of the first MTP joint, and the presence of first ray hypermobility. The following evidence-based algorithm (modified from Mann RA) guides procedure selection.
Mild Hallux Valgus (HVA < 25 Degrees, IMA < 13 Degrees)
Congruent Joint:
* Chevron Osteotomy: The workhorse for mild, congruent deformities. Provides excellent stability and predictable correction.
* Mitchell Osteotomy: A historical alternative, though less commonly used today due to the risk of dorsal malunion and transfer metatarsalgia.
Incongruent Joint:
* Distal Soft-Tissue Realignment (Modified McBride): Can be utilized if the IMA is minimal, though rarely performed in isolation today.
* Chevron Osteotomy: Often combined with a lateral release to restore joint congruency.
Moderate Hallux Valgus (HVA 25–40 Degrees, IMA 13–20 Degrees)
Congruent Joint:
* Chevron Osteotomy with Akin Procedure: The Akin (proximal phalanx medial closing wedge osteotomy) corrects residual hallux valgus interphalangeus without violating the congruent MTP joint.
Incongruent Joint:
* Distal Soft-Tissue Realignment with Proximal Osteotomy: A proximal crescentic or proximal chevron osteotomy allows for greater correction of the IMA. The distal soft-tissue procedure realigns the MTP joint.
Severe Hallux Valgus (HVA > 40 Degrees, IMA > 20 Degrees)
Congruent Joint:
* Double Osteotomy: Required to correct severe angular deformity without creating joint subluxation. Options include Akin combined with a Chevron osteotomy, Akin with a first metatarsal shaft osteotomy, or Akin with a first cuneiform opening wedge osteotomy.
Incongruent Joint:
* Distal Soft-Tissue Realignment with Proximal Osteotomy: Essential for severe incongruent deformities.
* First Metatarsal Crescentic Osteotomy: Provides powerful correction of the IMA.
* First Cuneiform Opening Wedge Osteotomy: Useful in cases with concurrent metatarsus adductus or a short first ray.
Hypermobile First Metatarsocuneiform Joint
- First Tarsometatarsal Arthrodesis (Lapidus Procedure): Combined with a distal soft-tissue realignment. This is the gold standard for patients with clinical hypermobility, severe deformity, or recurrent hallux valgus, as it stabilizes the medial column at its apex.
SURGICAL APPROACHES AND TECHNIQUES
Patient Positioning and Preparation
The patient is placed supine on the operating table. A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, ensuring the patella and foot face directly anteriorly. A well-padded thigh or calf tourniquet is applied. Prophylactic intravenous antibiotics are administered prior to inflation. Regional anesthesia (popliteal block or ankle block) is highly recommended for postoperative pain control.
Distal Soft-Tissue Realignment (Modified McBride)
Indications: Incongruent MTP joint, usually performed in conjunction with a metatarsal osteotomy.
Technique:
1. Medial Approach: A longitudinal incision is made centered over the medial eminence. The dorsal and plantar cutaneous nerves are protected.
2. Capsulotomy: An inverted L-shaped or vertical capsulotomy is performed to expose the medial eminence.
3. Exostectomy: The medial eminence is resected parallel to the medial border of the foot, preserving the sagittal sulcus to avoid destabilizing the tibial sesamoid.
4. Lateral Release: Accessed either transarticularly or via a separate dorsal first web-space incision. The adductor hallucis tendon is released from the base of the proximal phalanx and the fibular sesamoid. The deep transverse metatarsal ligament is transected.
5. Capsulorrhaphy: Following the osteotomy, the medial capsule is imbricated to hold the toe in neutral alignment.
Distal Metatarsal Osteotomy (Chevron)
Indications: Mild to moderate deformity (IMA < 15 degrees).
Biomechanics: A V-shaped osteotomy that allows lateral translation of the metatarsal head, reducing the IMA while maintaining intrinsic stability.
Technique:
1. Following exostectomy, a K-wire is placed in the center of the metatarsal head to mark the apex of the osteotomy.
2. A microsaw is used to create a V-shaped cut with an apex distal angle of approximately 60 degrees. The plantar arm must exit proximal to the sesamoid articulation.
3. The capital fragment is translated laterally by 3 to 5 mm (up to 50% of the bone width).
4. The osteotomy is provisionally pinned and then definitively fixed with a single headless compression screw or threaded K-wire.
5. The overhanging medial edge of the proximal fragment is resected flush with the translated head.
Proximal Metatarsal Osteotomy (Crescentic)
Indications: Moderate to severe deformity (IMA > 15 degrees).
Technique:
1. A dorsal longitudinal incision is made over the proximal first metatarsal.
2. A crescentic saw blade is used to make a dome-shaped osteotomy 1 to 1.5 cm distal to the first TMT joint, with the concavity facing proximally.
3. The distal fragment is rotated laterally to reduce the IMA.
4. Fixation is achieved with a low-profile plate or crossed compression screws.
5. Pitfall: Care must be taken to avoid dorsal elevation of the distal fragment, which will result in postoperative transfer metatarsalgia.
First Tarsometatarsal Arthrodesis (Lapidus Procedure)
Indications: Severe deformity, hypermobile first ray, recurrent hallux valgus.
Technique:
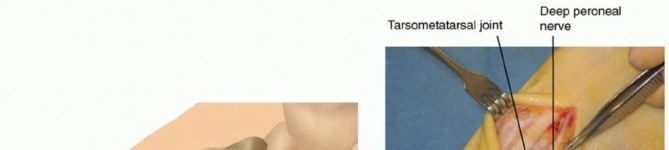
1. A dorsal incision is made over the first TMT joint.
2. The joint capsule is incised, and the articular cartilage of the medial cuneiform and the base of the first metatarsal is meticulously denuded using a saw, osteotomes, or curettes.
3. The subchondral bone is fenestrated to promote arthrodesis.
4. The deformity is reduced by plantarflexing and laterally translating the first metatarsal.
5. Rigid internal fixation is applied, typically utilizing a plantar or medial locking plate combined with a transarticular interfragmentary compression screw.
POSTOPERATIVE PROTOCOLS
Postoperative rehabilitation is dictated by the specific procedures performed and the stability of the fixation.
- Distal Osteotomies (Chevron): Patients are typically allowed immediate heel-weight-bearing or flat-foot weight-bearing in a rigid postoperative shoe. Dressings are changed at 2 weeks for suture removal, and the toe is taped in neutral alignment for 6 weeks to protect the medial capsulorrhaphy. Transition to a wide, soft athletic shoe occurs at 6 weeks.
- Proximal Osteotomies and Lapidus Arthrodesis: Due to the higher mechanical demands on proximal fixation, patients are generally kept strictly non-weight-bearing for 2 to 4 weeks, followed by protected weight-bearing in a controlled ankle motion (CAM) boot for an additional 4 weeks. Radiographic evidence of bridging trabecular bone is required before transitioning to normal footwear and unrestricted activity, typically around 8 to 10 weeks postoperatively.
Thorough preoperative planning, meticulous surgical execution, and strict adherence to postoperative protocols are essential to achieve durable, pain-free outcomes in hallux valgus reconstruction.
You Might Also Like