Medial Cuneiform and Proximal Phalangeal Osteotomies in Hallux Valgus Surgery
Key Takeaway
Medial cuneiform and proximal phalangeal (Akin) osteotomies are powerful adjunctive procedures for correcting complex hallux valgus deformities. The medial cuneiform opening wedge osteotomy is particularly indicated in adolescents with open physes and severe metatarsus primus varus. Conversely, the Akin closing wedge osteotomy effectively addresses hallux valgus interphalangeus and provides residual deformity correction. Both require meticulous preoperative radiographic planning, precise surgical execution, and rigid fixation to optimize biomechanical alignment and clinical outcomes.
Introduction and Epidemiology
Forefoot varus is a critical component of the multiplanar pes planovalgus deformity that occurs primarily as a result of posterior tibial tendon insufficiency. In addition to being a hallmark component of adult acquired flatfoot deformity, forefoot varus is also present in some cases of congenital pes planus and posttraumatic deformities of the first tarsometatarsal joint.
In 1936, Cotton described an adjunctive procedure for the operative treatment of flatfoot deformity using an opening wedge plantarflexion medial cuneiform osteotomy to restore what he termed the "triangle of support" of the static foot. Today, the Cotton osteotomy remains a cornerstone joint-sparing technique for correcting fixed forefoot supination or varus.

The epidemiology of forefoot varus is intimately tied to the incidence of adult acquired flatfoot deformity, which predominantly affects women in their fifth to seventh decades of life. The natural history of forefoot varus associated with an acquired adult flatfoot deformity has not been prospectively studied in isolation; however, it is presumed that the severity of the forefoot varus deformity progresses as the underlying pes planovalgus deformity worsens. Long-standing instability and subluxation at the first tarsometatarsal joint or naviculocuneiform joint may result in localized osteoarthritis of these joints. Some acquired adult flatfeet develop a fixed forefoot varus without osteoarthritis when the deformity has been longstanding and capsular stiffness holds the joint in the deformed position.
Surgical Anatomy and Biomechanics
Osseous Architecture of the Medial Column
Forefoot varus deformity may occur through a dorsiflexion angulation or rotation at the talonavicular, naviculocuneiform, or tarsometatarsal joints. The medial column of the foot consists of the talus, navicular, medial cuneiform, and the first metatarsal. The medial cuneiform is uniquely shaped, being wider plantarward than dorsalward, which contributes to the transverse arch of the midfoot.

Ligamentous and Dynamic Stabilizers
These joints are supported by the spring ligament complex (calcaneonavicular ligament) and the plantar intertarsal ligaments, including the long plantar ligament. In addition, the naviculocuneiform and tarsometatarsal joints are supported by their relatively constrained joint architecture, which in the normal state allows only a few degrees of motion in the sagittal plane.
The primary dynamic stabilizer of the medial column is the posterior tibial tendon, which inserts broadly across the navicular tuberosity, the cuneiforms, and the bases of the second through fourth metatarsals. The peroneus longus tendon acts as an antagonist, providing a plantarflexion force to the first ray. When the posterior tibial tendon fails, the peroneus brevis unopposedly everts the hindfoot, while the loss of dynamic medial support leads to medial column collapse.

Pathogenesis of Forefoot Varus
The pathogenesis of forefoot varus in association with an adult acquired flatfoot deformity secondary to posterior tibial tendon insufficiency is complex. Forefoot varus is presumed to develop when the posterior tibialis tendon can no longer provide dynamic support to the medial column of the midfoot. In the absence of the posterior tibialis tendon acting as a dynamic stabilizer, the static ligamentous stabilizers stretch out due to the repetitive dorsally directed weight-bearing forces on the medial column of the foot.
Several patterns of medial column "sag" have been described. The understanding of why some patients have dorsal instability at the first tarsometatarsal joint, the naviculocuneiform joint, or the talonavicular joint remains a subject of investigation. The differences in the magnitude and location of the dorsal sag may be related to bony anatomy, generalized ligamentous laxity, the presence or absence of gastrocnemius-soleus contracture, and the existence of an underlying congenital pes planovalgus deformity.
Medial displacement calcaneal osteotomy, lateral column lengthening, and subtalar fusion all provide correction of heel valgus; lateral column lengthening will correct forefoot abduction, but none of these procedures adequately addresses the fixed forefoot varus component of the pes planovalgus deformity. If hindfoot valgus is corrected and a fixed forefoot varus is left untreated, the patient will bear weight exclusively on the lateral border of the foot, leading to lateral column overload, pain, and eventual failure of the hindfoot correction.
Indications and Contraindications
The primary indication for a medial cuneiform opening wedge osteotomy is a fixed forefoot varus deformity in the setting of adult acquired flatfoot deformity, provided the medial column joints (naviculocuneiform and tarsometatarsal) are free of significant arthritic changes. The procedure is almost always performed as an adjunct to hindfoot reconstructive procedures.

| Clinical Scenario | Operative Indications | Non Operative Indications |
|---|---|---|
| Adult Acquired Flatfoot Deformity | Fixed forefoot varus persisting after hindfoot correction; flexible joints without severe arthritis. | Flexible forefoot varus that corrects with hindfoot realignment; asymptomatic flatfoot. |
| Medial Column Sag | Apex of deformity at the medial cuneiform or naviculocuneiform joint without degenerative changes. | Severe osteoarthritis at the first TMT or NC joint (requires arthrodesis instead). |
| Congenital Pes Planus | Symptomatic fixed supination of the forefoot failing conservative management. | Asymptomatic or fully flexible deformity managed with orthotics. |
| Iatrogenic Deformity | Residual forefoot varus following previous hindfoot fusion or osteotomy. | Active local infection, severe osteopenia preventing fixation, critical vascular compromise. |
Contraindications include severe degenerative joint disease at the first tarsometatarsal or naviculocuneiform joints. In the presence of arthritis, an arthrodesis (such as a modified Lapidus procedure or naviculocuneiform fusion) is indicated to simultaneously correct the deformity and eliminate the painful articulation. Severe osteopenia, active infection, and compromised soft tissue envelopes are absolute contraindications to the procedure.
Pre Operative Planning and Patient Positioning
Clinical Evaluation and Physical Examination
Forefoot varus is one of the components of a pes planovalgus deformity that is determined primarily by radiographic and physical examination findings. In the patient history, there may be complaints of localized pain to the dorsal medial column of the midfoot, either the tarsometatarsal joint or the naviculocuneiform joint. Patients may complain of pressure-related discomfort beneath the base of the first metatarsal or cuneiform due to excessive weight bearing at the apex of the plantar medial column sag.

The presence and the magnitude of forefoot varus are determined on physical examination by placing the hindfoot into the "subtalar neutral" position with the patient seated. With the hindfoot held in neutral, the relationship of the forefoot to the hindfoot is assessed. If the medial border of the forefoot is elevated relative to the lateral border, a forefoot varus deformity is present. The flexibility of this deformity must be assessed; if the first ray cannot be passively plantarflexed to the level of the lateral column, the deformity is considered fixed, indicating the need for a structural correction such as the Cotton osteotomy.
Additionally, the Silfverskiöld test must be performed to evaluate for gastrocnemius or Achilles tendon contracture, which is present in the vast majority of patients with adult acquired flatfoot deformity and must be addressed concurrently.
Radiographic Evaluation
Standard weight-bearing radiographs of the foot (anteroposterior, lateral, and axial hindfoot views) are mandatory.
On the lateral view, the medial column sag is quantified using Meary's angle (the angle between the longitudinal axis of the talus and the first metatarsal). A normal Meary's angle is 0 degrees; in flatfoot deformity, the angle is convex plantarly. The apex of the deformity should be identified to ensure the medial cuneiform osteotomy is the appropriate procedure.
The anteroposterior view is utilized to assess talonavicular coverage and the degree of forefoot abduction. The presence of degenerative changes at the naviculocuneiform and tarsometatarsal joints must be carefully scrutinized, as this alters the surgical plan from an osteotomy to an arthrodesis.

Operative Setup
The patient is positioned supine on the operating table. A bump is placed under the ipsilateral hip to internally rotate the lower extremity, ensuring the foot rests in a neutral position pointing directly toward the ceiling. This is particularly important for accessing the medial and lateral aspects of the foot, as multiple procedures are typically performed concurrently.
A thigh or calf tourniquet is applied based on surgeon preference. The entire lower extremity is prepped and draped in a standard sterile fashion. Fluoroscopy is positioned to enter from the contralateral side of the table, allowing for unobstructed anteroposterior and lateral imaging of the foot throughout the procedure.
Detailed Surgical Approach and Technique
The medial cuneiform osteotomy is typically performed after the hindfoot corrections (e.g., medial displacement calcaneal osteotomy, lateral column lengthening) have been provisionally or definitively fixed. Once the hindfoot is corrected, the residual forefoot varus becomes clinically apparent, and the degree of necessary plantarflexion can be accurately gauged.
Incision and Dissection
A 4 to 5 centimeter longitudinal incision is made over the dorsomedial aspect of the medial cuneiform. The incision is centered between the tibialis anterior tendon and the extensor hallucis longus tendon.
Careful subcutaneous dissection is performed to identify and protect the medial dorsal cutaneous nerve and terminal branches of the saphenous nerve. Retraction of these neural structures is critical to prevent postoperative neuromas. The extensor hallucis longus tendon is retracted laterally, and the tibialis anterior tendon is retracted medially.

Joint Identification and Exposure
The periosteum over the medial cuneiform is incised longitudinally and elevated via sharp subperiosteal dissection. It is imperative to accurately identify the naviculocuneiform joint proximally and the first tarsometatarsal joint distally. This can be achieved by placing small Keith needles or 25-gauge needles into the joints and confirming their position with lateral fluoroscopy.
Adequate exposure of the dorsal, medial, and lateral aspects of the medial cuneiform is necessary, but aggressive plantar stripping must be avoided to preserve the plantar ligaments and the blood supply, which will serve as the tension band and hinge for the osteotomy.
Osteotomy Execution
The osteotomy is planned in the central portion of the medial cuneiform, parallel to the articular surfaces of the naviculocuneiform and tarsometatarsal joints. Using a sagittal saw, the osteotomy is initiated on the dorsal cortex and directed plantarly.
The saw blade must be kept strictly perpendicular to the medial border of the foot in the coronal plane to avoid inducing an unintended transverse plane deformity. The osteotomy is carried down through the cancellous bone to the plantar cortex. It is critical to leave the plantar cortex and the robust plantar ligaments intact to act as a hinge.
Once the saw cut is nearly complete, an osteotome is gently advanced into the osteotomy site to complete the cut down to the plantar cortex. A lamina spreader or a specialized wedge-opening distractor is then inserted into the dorsal aspect of the osteotomy.

The osteotomy is slowly and carefully opened to plantarflex the first ray. The degree of opening is determined clinically by assessing the position of the first metatarsal head relative to the lesser metatarsal heads. The goal is to bring the first metatarsal head down to the same weight-bearing plane as the lateral column when the hindfoot is held in neutral.
Graft Sizing and Placement
Once the desired correction is achieved, the gap is measured. Typical wedge sizes range from 4 to 8 millimeters. The void can be filled with a variety of materials, including autologous tricortical iliac crest bone graft, allograft bone wedges, or porous metallic/PEEK wedges.
Allograft tricortical wedges (e.g., from the iliac crest or calcaneus) are frequently utilized to avoid the donor site morbidity associated with autograft harvest. The graft is fashioned to match the dimensions of the defect, ensuring it is wider dorsally and tapers plantarly. The graft is impacted into the osteotomy site while maintaining distraction.
Fixation Strategies
After the graft is seated, the distractor is removed, and the plantar hinge applies a compressive force across the graft. While the intact plantar hinge provides inherent stability, supplemental fixation is highly recommended to prevent dorsal extrusion of the graft and to maintain the correction.
Fixation can be achieved using a variety of implants. A dorsal spanning plate (such as a 2-hole or 4-hole low-profile titanium plate) secured with locking or non-locking screws is a biomechanically sound choice. Alternatively, memory-compression staples or crossed Kirschner wires may be utilized.

Following fixation, final fluoroscopic images are obtained to confirm the restoration of Meary's angle, the appropriate seating of the graft, and the correct extra-articular placement of all hardware. The periosteum and extensor retinaculum are closed over the hardware, followed by standard subcutaneous and skin closure.
Complications and Management
While the medial cuneiform opening wedge osteotomy is generally safe and effective, specific complications can arise due to the technical demands of the procedure and the complex biomechanics of the medial column.
| Complication | Incidence | Etiology and Management Strategies |
|---|---|---|
| Nonunion / Delayed Union | 2% - 5% | Associated with smoking, poor graft incorporation, or inadequate fixation. Management requires prolonged immobilization, bone stimulators, or revision surgery with autograft and robust plate fixation. |
| Hardware Prominence | 10% - 15% | The dorsal aspect of the midfoot has minimal soft tissue coverage. Prominent plates or staples may irritate footwear. Management consists of hardware removal after definitive radiographic union is achieved (typically >6 months). |
| Overcorrection (Plantarflexed First Ray) | 1% - 3% | Caused by inserting an excessively large wedge. Leads to a rigid plantarflexed first ray, resulting in sesamoiditis and first metatarsal head intractable plantar keratosis. Salvage may require dorsal closing wedge osteotomy of the first metatarsal. |
| Undercorrection | 3% - 8% | Failure to insert an adequate wedge or failure to recognize the full extent of the forefoot varus. Results in lateral column overload. Management involves orthotic offloading or revision osteotomy. |
| Plantar Hinge Fracture | 5% - 10% | Occurs during aggressive distraction or if the saw cut penetrates the plantar cortex. Results in destabilization of the osteotomy. Requires immediate rigid internal fixation, typically with a longer, more robust dorsal plate to bridge the instability. |
| Nerve Injury | < 5% | Neuropraxia or neuroma of the medial dorsal cutaneous nerve or saphenous branches due to aggressive retraction. Managed with gabapentinoids, targeted injections, or surgical neuroma excision if conservative measures fail. |
Meticulous surgical technique, particularly regarding the preservation of the plantar hinge and the careful handling of the dorsal neural structures, is the most effective method for minimizing these complications.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol for a Cotton osteotomy is largely dictated by the concomitant hindfoot procedures performed during the adult acquired flatfoot reconstruction. However, the integration of a midfoot osteotomy necessitates strict adherence to weight-bearing restrictions to ensure graft incorporation and prevent hardware failure.
Phase I: Immediate Postoperative Period (Weeks 0 - 2)
The patient is placed in a well-padded short leg splint in the operating room. The foot is maintained in a neutral position. The patient is strictly non-weight-bearing on the operative extremity. Elevation and strict edema control are emphasized. Sutures are removed at 10 to 14 days postoperatively.
Phase II: Immobilization and Non-Weight-Bearing (Weeks 2 - 6)
Following suture removal, the patient is transitioned to a short leg fiberglass cast or a rigid controlled ankle motion (CAM) boot. Strict non-weight-bearing is continued. Radiographs are obtained at the 6-week mark to assess for early graft incorporation and maintenance of alignment.
Phase III: Progressive Weight-Bearing (Weeks 6 - 10)
If 6-week radiographs demonstrate satisfactory healing of the osteotomy and concomitant hindfoot fusions/osteotomies, the patient may begin progressive weight-bearing in the CAM boot. Weight-bearing is advanced by 25% of body weight every few days as tolerated. Physical therapy is initiated to focus on active and active-assisted range of motion of the ankle, subtalar, and midtarsal joints.
Phase IV: Transition to Shoe Wear and Strengthening (Weeks 10+)
At 10 to 12 weeks, the patient is transitioned from the CAM boot to a supportive athletic shoe, often fitted with a custom orthotic or an over-the-counter arch support to protect the reconstruction. Physical therapy focuses on strengthening the dynamic stabilizers, particularly the posterior tibial tendon (if reconstructed) and the peroneal musculature, as well as proprioceptive training. Maximal medical improvement is typically reached between 9 and 12 months postoperatively.
Summary of Key Literature and Guidelines
The literature strongly supports the use of the medial cuneiform opening wedge osteotomy for the correction of fixed forefoot varus in adult acquired flatfoot deformity.
Cotton's original 1936 description laid the conceptual framework for restoring the "triangle of support." The modern resurgence of the procedure is largely attributed to Hirose and Johnson (2004), who demonstrated excellent clinical outcomes and reliable restoration of Meary's angle using structural allograft wedges. Their work underscored the importance of addressing the forefoot to prevent lateral column overload following hindfoot valgus correction.
Biomechanical studies have validated the efficacy of the Cotton osteotomy. Bixby et al. analyzed union rates and found that allograft utilization in the medial cuneiform yields union rates exceeding 95%, comparable to autograft, thereby validating the use of allograft to spare patients donor site morbidity. Furthermore, pedobarographic analyses have shown that adequate plantarflexion of the first ray normalizes forefoot contact pressures, shifting the load away from the lateral column and restoring normal first ray weight-bearing mechanics.
Current academic guidelines recommend intraoperative clinical assessment of forefoot varus after provisional hindfoot correction. If the first ray remains elevated above the lateral column, a joint-sparing medial cuneiform osteotomy is the procedure of choice, provided the adjacent joints are free of advanced arthritic degeneration. This algorithmic approach ensures comprehensive, multiplanar correction of the pes planovalgus deformity, optimizing long-term functional outcomes.
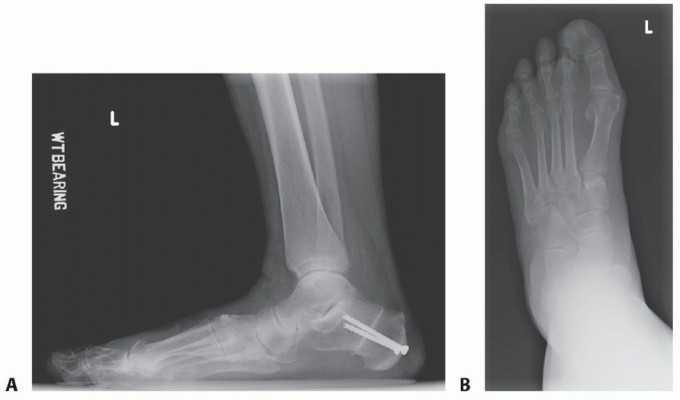
Clinical & Radiographic Imaging
You Might Also Like

