Advanced Management of Complications Following Hallux Valgus Surgery
Key Takeaway
Complications following hallux valgus surgery, including recurrent deformity and hallux varus, present significant challenges. Successful revision requires meticulous clinical and radiographic evaluation to identify the biomechanical failure points. This guide details the etiology of recurrent bunions, essential weight-bearing radiographic parameters, and step-by-step surgical techniques for revision soft tissue reconstruction and capsular imbrication to restore the capsulosesamoid apparatus.
INTRODUCTION TO HALLUX VALGUS COMPLICATIONS
Complications following hallux valgus procedures can be profoundly discouraging for both patients and operating physicians. Despite extensive clinical experience, detailed physical and radiographic evaluations, meticulous surgical technique, and highly controlled postoperative care, the absolute prevention of complications cannot be guaranteed. The pathoanatomy of the first ray is complex, relying on a delicate balance of dynamic muscular forces and static ligamentous restraints.
The most frequently encountered complications include recurrence of the original hallux valgus deformity, iatrogenic overcorrection leading to hallux varus, malunion or nonunion of osteotomies, avascular necrosis (AVN) of the first metatarsal head, clawed hallux, and the development of transfer keratotic lesions resulting in intractable plantar keratosis (IPK). Successful management of these complications demands a postgraduate-level understanding of forefoot biomechanics, precise identification of the index procedure's failure mechanism, and mastery of advanced revision techniques.
PREVENTING COMPLICATIONS: THE CLINICAL EVALUATION
In the surgical treatment of hallux valgus, the prevention of complications begins at the very moment of the initial patient evaluation. A superficial assessment inevitably leads to poor procedure selection, which is the primary driver of surgical failure. A comprehensive physical examination can identify subtle biomechanical anomalies that ultimately predispose certain patients to recurrence or hardware failure.
Before any definitive decision is made regarding the surgical management of hallucal disorders, the foot and ankle must be examined dynamically and statically. The patient should be evaluated while sitting, standing (weight-bearing), lying supine, and prone. The time dedicated to the clinical evaluation of the deformity should equal or exceed the time spent reviewing the radiographs.
Clinical Pearl: A prominent medial eminence (bunion) is typically present with a hallux valgus deformity, but this is not an absolute rule. Furthermore, first metatarsal varus (metatarsus primus varus) is not universally present. Do not rely solely on the presence of a bunion to dictate the surgical algorithm.
Key Clinical Indicators of Potential Failure
Rotation of the hallux (pronation) is a critical element of the deformity. Pronation of the great toe indicates a severe, multiplanar deformity and provides significant insight into the condition of the entire capsulosesamoid apparatus.
Recurrence of a hallux valgus deformity is statistically more likely when the following clinical risk factors are present:
* First Metatarsophalangeal (MTP) Joint Subluxation: Frank subluxation or dislocation of the joint indicates severe attenuation of the medial capsuloligamentous structures.
* Hallux Pronation: Frequently an indication of advanced coronal plane deformity and lateral sesamoid dislocation.
* Fixed Deformity: A rigid first MTP joint that does not passively correct to neutral suggests significant soft tissue contracture or degenerative joint disease.
* Pes Planus and Joint Hypermobility: First ray hypermobility or a collapsed medial longitudinal arch (pes planus) places excessive valgus thrust on the first MTP joint during the terminal stance phase of gait.
* Gastrocnemius-Soleus Equinus: A tight heel cord forces early heel rise, exponentially increasing forefoot loading and exacerbating the deforming forces on the first ray.
RADIOGRAPHIC EVALUATION: THE WEIGHT-BEARING IMPERATIVE
Just as the physical examination must include a standing assessment, the radiographic evaluation of the foot is fundamentally incomplete without weight-bearing views. The discrepancy in the magnitude of the deformity between non-weight-bearing and weight-bearing radiographs is often striking and clinically significant. A concise, detailed evaluation of weight-bearing radiographs is imperative before planning any primary or revision procedure.
Correction of each anatomical component contributing to the hallux valgus deformity is necessary to avoid complications.
Observations on Weight-Bearing Anteroposterior (AP) Views

The weight-bearing AP radiograph is the cornerstone of preoperative planning. The surgeon must systematically evaluate the following parameters:
* Intermetatarsal Angle (IMA): Varus of the first metatarsal (normal IMA is ≤ 9 degrees).
* Hallux Valgus Angle (HVA): Severity of the valgus deviation of the hallux (normal HVA is ≤ 15 degrees).
* Joint Congruity: Congruity or incongruity of the first MTP joint. Note that a hallux valgus deformity can exist even within a congruous joint (often driven by an abnormal DMAA).
* Metatarsal Parabola: Length of the first metatarsal relative to the second. If the second metatarsal is > 6 to 7 mm longer than the first, the patient is at high risk for transfer metatarsalgia.
* Sesamoid Station: Subluxation of the sesamoid bones (graded via the Hardy and Clapham classification).
* First Metatarsocuneiform (MTC) Joint: Look for a well-developed facet between the first and second metatarsals, which suggests difficulty in displacing the first metatarsal laterally during a proximal osteotomy or Lapidus procedure. Note any severe lateral-to-medial sloping of the first MTC articulation.
* Degenerative Changes: Assess for arthritic narrowing, subchondral sclerosis, or osteophytes at the interphalangeal (IP), MTP, or MTC articulations.
* Hallux Valgus Interphalangeus (HVI): Normal is ≤ 10 degrees in neutral flexion/extension.
* Distal Metatarsal Articular Angle (DMAA): Excessive lateral sloping of the distal articular surface (normal DMAA is ≤ 15 degrees).
* Proximal Phalanx Morphology: Look for convex medial bowing of the proximal phalanx, which may necessitate an Akin osteotomy.
Observations on Weight-Bearing Lateral Views
The lateral view determines the degree of valgus thrust on the hallux MTP joint during the stance phase of gait, heavily influencing treatment decisions:
* Midfoot Collapse: Look for collapse deformity at the MTC, cuneonavicular, or talonavicular articulations (e.g., a broken Meary's line).
* Hindfoot Alignment: An increased talocalcaneal angle suggests a valgus posture of the hindfoot.
* Calcaneal Pitch: The calcaneal inclination angle (≥ 10 degrees is normal; a reduced angle indicates a valgus hindfoot and structural pes planus).
* First Metatarsal Elevation: Dorsiflexion (elevation) of the first metatarsal indicates incongruous reduction into the concavity of the base of the proximal phalanx.
* Diaphyseal Angle: The angle between the diaphysis of the proximal phalanx and the diaphysis of the first metatarsal (≥ 20 degrees is normal).
* Lesser Metatarsal Overlap: Delineation of the cortical outlines of the fifth, fourth, and third metatarsals. If the cortical borders are not clearly outlined and appear heavily overlapped on a weight-bearing lateral radiograph, severe pronation of the foot should be suspected.
Observations on Non-Weight-Bearing Medial Oblique Views
While weight-bearing views are paramount, the medial oblique view provides specific diagnostic utility:
* MTC Arthritis: Excellent visualization of arthritic changes in the first metatarsal–medial cuneiform articulation.
* Tarsal Coalitions: Identification of calcaneonavicular tarsal coalitions that may not be visible on standard AP or lateral views.
Observations on the Weight-Bearing Sesamoid View

The weight-bearing sesamoid axial view is especially useful in the evaluation of recurrent hallux valgus deformity. Repositioning the intrinsic and extrinsic muscles and the capsulosesamoid apparatus into their anatomical positions is the absolute key to correction.
* Sesamoid-Facet Relationship: This view clearly demonstrates the location of the sesamoid bones in relation to their respective facets on the plantar aspect of the first metatarsal head (often obscured on an AP view). Failure to reduce the sesamoid sling apparatus after a soft tissue procedure is a primary cause of recurrence and persistent pain beneath the tibial sesamoid.
RECURRENT DEFORMITY AFTER SIMPLE BUNIONECTOMY
Recurrence of the deformity is a frequent and frustrating complication following a simple bunionectomy (defined as isolated medial eminence excision combined with medial capsular imbrication, such as a Silver procedure).
Although it is tempting for the surgeon to perform a minor procedure for a seemingly minor deformity, soft tissue repair alone should not be performed except in highly specific scenarios—namely, in elderly, low-demand patients with impending skin breakdown over the medial eminence, and only if the hallux is congruously reduced on the first metatarsal head with normal HVA and IMA parameters.
Pathoanatomy of Recurrence
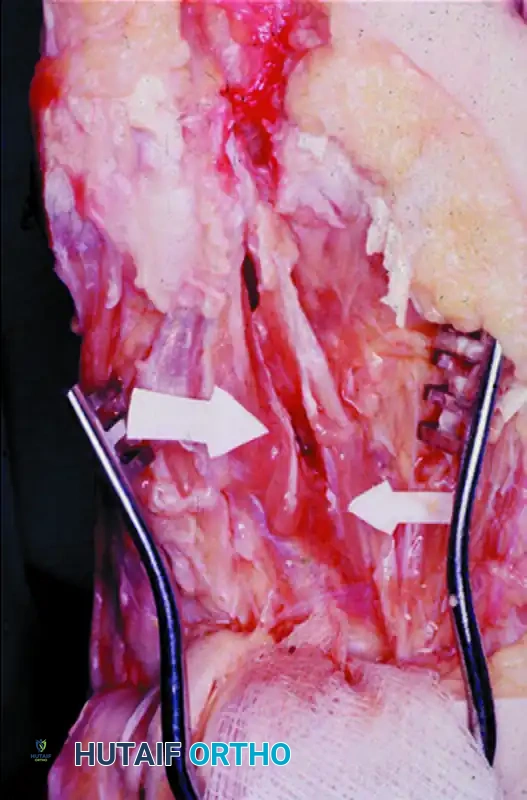
If a soft tissue procedure is chosen, a first web space dissection and lateral release must always be performed in conjunction with medial eminence removal and medial capsular imbrication. If the hallux does not remain in the desired corrected position at the conclusion of surgery without being held, adduction of the hallux will inevitably recur.
The Adductor Hallucis: The adductor must be released not only from its insertion on the base of the proximal phalanx but also from its conjoined insertion with the lateral head of the flexor hallucis brevis (FHB) on the fibular sesamoid. Tenotomy alone is generally effective, but the entire adductor insertion must be incised, and a section must be excised proximal to the MTP joint to prevent scarring and reattachment.
The Lateral Capsule: The lateral capsular release is an equally important factor. The lateral capsule must be incised beginning at the lateral margin of the extensor hallucis longus (EHL) tendon and progressing plantarward to the lateral edge of the fibular sesamoid. Alternatively, multiple perforations can be made in the lateral capsule, completing the capsulotomy by manually forcing the hallux into 20 to 25 degrees of varus before returning it to a neutral position.
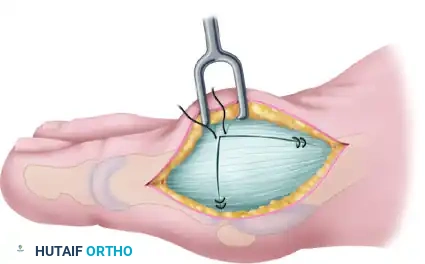
The Medial Capsule: If the redundant, attenuated medial capsule is not aggressively trimmed and imbricated to hold the hallux in correct alignment, recurrence is highly likely.
Bony and Extrinsic Muscular Factors
Failure to reposition the articular surface of the metatarsal head to a normal 5- to 15-degree alignment with the metatarsal shaft (correcting the DMAA) will severely compromise the correction. If the MTP joint is congruent but in a position of unacceptable valgus, correction must be obtained via a proximal phalangeal osteotomy (Akin), a distal metatarsal osteotomy (Chevron), or both.
Surgical Warning: Failure to reduce the sesamoid sling allows the lateral head of the flexor hallucis brevis muscle to pull the hallux into valgus, acting synergistically with the extensor hallucis longus and flexor hallucis longus muscles. These extrinsic muscles bowstring laterally across the MTP joint, exponentially increasing the valgus moment arm and guaranteeing recurrence. Releasing the capsulosesamoid ligament in an axial plane is integral to repositioning the sesamoid apparatus.
INDICATIONS FOR REVISION SOFT TISSUE REPAIR
The magnitude and rigidity of the recurrent deformity must guide the revision treatment algorithm. As a strict rule, a deformity that recurred after a primary soft tissue procedure should not be treated with another isolated soft tissue procedure unless the deformity is completely flexible. Flexibility is defined clinically: the hallux can be easily reduced into varus, and the first metatarsal freely translates laterally by manual pressure.
For severe, rigid recurrences, a proximal first metatarsal osteotomy or Lapidus arthrodesis combined with distal soft tissue reconstruction is required.
Indications for Soft Tissue Repair for Recurrent Hallux Valgus:
* First-second intermetatarsal angle (IMA) of ≤ 13 degrees.
* Hallux valgus angle (HVA) of ≤ 30 degrees.
* Normal distal metatarsal articular angle (DMAA < 10–15 degrees).
* Minimal degenerative arthritic changes at the first MTP joint.
* 50 to 60 degrees of passive motion of the first MTP joint.
* Subluxation, but not complete dislocation, of the sesamoid bones.
* Ability to passively displace the first metatarsal laterally at the MTC joint from its abnormal varus inclination.
* Presence of a functional longitudinal arch during weight-bearing. (If the arch improves with passive dorsiflexion of the hallux while standing—the Jack's test or windlass mechanism—the deformity is not a fixed structural pes planus, and a soft tissue repair is more likely to endure).
SURGICAL TECHNIQUE: FIRST WEB SPACE DISSECTION, LATERAL RELEASE, AND REPEAT CAPSULAR IMBRICATION
This technique is indicated for recurrent hallux valgus with a normal DMAA following a failed simple bunionectomy, provided the deformity remains flexible and meets the criteria outlined above.
Step 1: Incision and Neural Protection
Make a straight midline medial incision, extending from the middle of the proximal phalanx to 3 to 4 cm proximal to the first MTP joint.
Surgical Pearl: This incision lies in the internervous plane between the most medial branch of the superficial peroneal nerve (dorsomedial aspect of the hallux) and the proper branch of the medial plantar nerve (medial side of the hallux). The medial plantar nerve branch rests plantar-medially and blends intimately with the overlying superficial fascia, making it highly vulnerable to iatrogenic transection. Meticulous blunt dissection is required.
Step 2: Elevation of the Dorsal Flap
Raise a full-thickness dorsal flap the entire length of the incision until the EHL tendon and the dorsal aspect of the first MTP joint are exposed proximally, and the extensor hood is exposed distally.
The plane of dissection for this dorsal flap is critical. Do not enter the extensor mechanism itself; rather, raise the flap adjacent to it so that the flap carries the dorsal veins and the dorsal sensory nerves safely out of the operative field. Use blunt dissection proximally, as the dorsal nerve frequently crosses the center of the incision exactly where the medial eminence joins the metatarsal shaft.
Step 3: The Inverted-L Capsulotomy
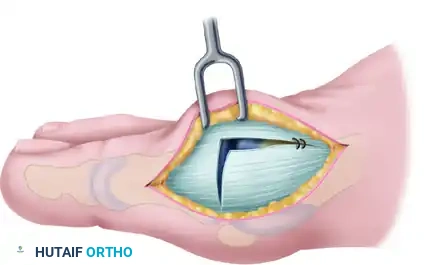
To maximize the effectiveness of the revision capsular imbrication, an extensive dorsal exposure is required. Commonly, a thin slip of accessory extensor tendon is visible; this serves as a helpful anatomical landmark. If absent, locate the dorsal and medial juncture of the rounded distal first metatarsal head.
Using either the medial aspect of the accessory tendon or the dorsomedial border of the first metatarsal as a starting point, perform an inverted-L capsulotomy. Complete a capsular-periosteal excision from the first MTP joint line extending proximally to the junction of the middle and distal thirds of the metatarsal.
Begin the transverse limb of this incision exactly at the joint line. Applying axial traction on the hallux helps to identify the distal edge of the metatarsal head, preventing inadvertent scoring of the articular cartilage with the scalpel. The transverse limb extends from dorsal to plantar through the capsule and the conjoined capsular-abductor hallucis tendon insertion, terminating 2 to 3 mm medial to the tibial sesamoid.
Step 4: Capsular Flap Elevation
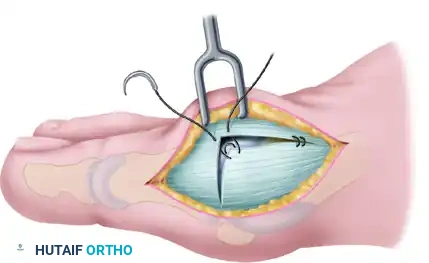
With a small, pointed blade (e.g., a #15 blade), carefully raise the medial capsule from the underlying bone. Begin at
Associated Surgical & Radiographic Imaging
You Might Also Like

