Arthrodesis of the First Metatarsocuneiform Articulation (Lapidus Procedure) and Management of Adolescent Hallux Valgus
Key Takeaway
The Lapidus procedure, an arthrodesis of the first metatarsocuneiform joint, is a powerful surgical technique for correcting severe hallux valgus, particularly in patients with hypermobility or recurrent deformity. This comprehensive guide details the biomechanical rationale, step-by-step operative execution—including sequential lateral release, joint preparation, and rigid plate fixation—alongside evidence-based postoperative protocols. Additionally, it outlines the distinct clinical considerations and surgical timing for managing juvenile and adolescent hallux valgus.
INTRODUCTION TO THE LAPIDUS PROCEDURE
The arthrodesis of the first metatarsocuneiform (TMT) articulation, universally recognized as the Lapidus procedure, remains a cornerstone in the armamentarium of the reconstructive foot and ankle surgeon. Originally described by Paul Lapidus in 1934, the procedure was designed to address the root cause of severe hallux valgus: metatarsus primus varus combined with hypermobility of the first ray.
Over the decades, the procedure has evolved significantly. Modern iterations, championed by surgeons such as Sorensen, Hyer, and Berlet, utilize advanced rigid internal fixation—specifically, interfragmentary screw fixation augmented by a dorsomedial locking plate. This biomechanically superior construct has drastically reduced historical nonunion rates from upwards of 20% to less than 5%, allowing for more aggressive rehabilitation protocols and improved long-term functional outcomes.
INDICATIONS AND PATIENT SELECTION
The Lapidus procedure is not a first-line treatment for mild to moderate hallux valgus; rather, it is reserved for complex, severe, or recurrent deformities. Proper patient selection is paramount to achieving a successful outcome.
Primary indications include:
* Recurrent Hallux Valgus: Patients presenting with a recurrence of the metatarsus primus varus component following a failed previous bunionectomy (e.g., failed distal chevron or Austin osteotomy).
* First Ray Hypermobility: Patients with marked ligamentous laxity or clinical hypermobility of the first TMT joint, often assessed clinically by excessive dorsal excursion of the first ray relative to the lesser metatarsals.
* Severe Deformity: An intermetatarsal angle (IMA) exceeding 15 to 20 degrees, where distal or diaphyseal osteotomies cannot provide adequate correction.
* Neuromuscular Deformity: Patients with cerebral palsy or other neuromuscular disorders presenting with spastic equinovalgus, metatarsus primus varus, and hallux valgus. The arthrodesis provides a rigid medial column to resist spastic deforming forces.
💡 Clinical Pearl: Assessing Hypermobility
True hypermobility of the first ray is often debated in the literature. Rather than relying solely on manual sagittal plane translation, evaluate the patient dynamically. Look for radiographic evidence of a cortical "sag" at the first TMT joint on weight-bearing lateral radiographs, or the presence of a transfer lesion beneath the second metatarsal head, which strongly suggests medial column incompetence.
BIOMECHANICAL RATIONALE
The first TMT joint is a complex, kidney-shaped articulation that dictates the spatial orientation of the entire medial column. By fusing this joint, the surgeon achieves three critical biomechanical goals:
1. Transverse Plane Correction: Direct reduction of the intermetatarsal angle (IMA) to normal physiological limits (less than 9 degrees).
2. Sagittal Plane Stabilization: Plantarflexion of the first metatarsal to restore the weight-bearing capacity of the first ray, thereby alleviating or preventing transfer metatarsalgia.
3. Frontal Plane Derotation: Correction of the pronatory twist of the first metatarsal, which is increasingly recognized as a primary driver of hallux valgus pathogenesis.
SURGICAL TECHNIQUE: LAPIDUS PROCEDURE WITH PLATE FIXATION
Anesthesia and Positioning
- Anesthesia: Administer a regional popliteal sciatic nerve block combined with a saphenous nerve block for optimal postoperative analgesia. Induce general anesthesia or deep intravenous sedation based on patient comorbidities and surgeon preference.
- Positioning: Place the patient supine on the operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg to a neutral position, ensuring the foot points directly toward the ceiling.
- Preparation: Prepare and drape the limb using standard sterile orthopedic technique. Exsanguinate the operative limb using an Esmarch bandage and inflate a proximal thigh tourniquet to 300 mm Hg to ensure a bloodless surgical field.
Incision 1: Sequential Lateral Release
The lateral release is critical for mobilizing the first metatarsophalangeal (MTP) joint and allowing the hallux to be reduced without tension.
* Make a 3 to 4 cm longitudinal dorsal incision over the first intermetatarsal space.
* Deepen the dissection carefully, protecting the terminal branches of the deep peroneal nerve and the first dorsal metatarsal artery.
* Perform a sequential lateral release:
1. Fibular Sesamoid Ligament Recession: Release the ligamentous attachments to the fibular sesamoid.
2. Conjoined Adductor Tenotomy: Release the adductor hallucis tendon from its insertion on the base of the proximal phalanx and the fibular sesamoid.
3. Deep Transverse Metatarsal Ligament Transection: Carefully divide this ligament to free the sesamoid apparatus from the lesser metatarsals.
4. Lateral Capsular "Pie-Crusting": Instead of a complete lateral capsulotomy, which risks avascular necrosis of the metatarsal head, perform multiple small fenestrations (pie-crusting) in the lateral capsule. Attenuate the capsule by applying a 45-degree varus stress to the hallux.
Incision 2: Medial Eminence Resection
- Make a second longitudinal incision over the medial aspect of the first MTP joint, centered over the medial eminence.
- Deepen the incision through the subcutaneous tissue, taking care to protect the dorsomedial cutaneous nerve.
- Perform an inverted-L medial capsulotomy. The vertical limb of the "L" should be at the base of the proximal phalanx, and the horizontal limb along the dorsal aspect of the metatarsal head.
- Reflect the capsule plantarly to expose the hypertrophic medial eminence.
- Using a sagittal saw, resect the hypertrophic medial eminence (bunion). The cut should be made parallel to the medial border of the foot, preserving the sagittal groove to ensure the tibial sesamoid does not subluxate medially.
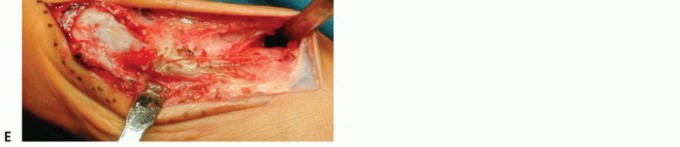
Incision 3: First Metatarsocuneiform Joint Exposure
- Make a third longitudinal incision over the dorsomedial aspect of the first TMT joint, extending from the base of the first metatarsal to the medial cuneiform.
- Identify and protect the extensor hallucis longus (EHL) tendon dorsally and the tibialis anterior tendon insertion plantarly.
- Perform a transverse capsulotomy to expose the joint.
- Joint Distraction: Insert smooth Steinmann pins into the medial cuneiform and the base of the first metatarsal. Apply a Hintermann retractor over the pins and distract the joint to maximize visualization.
Joint Preparation: The Critical Step
The success of the Lapidus procedure hinges entirely on meticulous joint preparation.
* Use a sharp osteotome and a mallet to denude the corresponding articular surfaces of the first metatarsal base and the medial cuneiform.
* Preserve the Subchondral Plate: It is imperative to remove the cartilage while maintaining the structural integrity of the subchondral bone plate. This prevents shortening of the first ray and provides a dense osseous foundation for screw purchase.
* Ensure the joint is fully exposed to a depth of up to 3 cm plantarward to guarantee the complete removal of the entire cartilaginous surface.
* Scalloping and Fenestration: Use a 2.0 mm drill bit or a sharp curette to scallop and fenestrate the subchondral plate. This breaches the avascular subchondral bone, releasing marrow elements and promoting robust angiogenic and osseous growth across the fusion site.
* Peripheral Rim Preservation: Retain the peripheral cortical rim of the joint. This maintains the length of the medial column and provides added mechanical stability for internal fixation.
* If autologous bone graft, allograft, or bone marrow aspirate (BMA) is utilized, pack it tightly within the prepared fusion site at this stage.
⚠️ Surgical Warning: Plantar Gapping
Failure to adequately prepare the plantar aspect of the TMT joint is the most common cause of nonunion and dorsal malunion (elevation of the first ray). Ensure visualization extends completely to the plantar-lateral corner of the articulation.
Reduction and Provisional Fixation
- Remove the Hintermann retractor.
- Manually reduce the first metatarsal in the transverse plane, closing the intermetatarsal angle.
- Engage the Windlass Mechanism: Attain the correct sagittal position by dorsiflexing the hallux. This engages the plantar fascia, naturally plantarflexing the first metatarsal and restoring the medial longitudinal arch.
- If the deformity is rigid, utilize a large bone reduction clamp (e.g., a Weber clamp) placed between the medial cuneiform and the second metatarsal to hold the first metatarsal in the corrected transverse position.
Definitive Internal Fixation
- With the metatarsal held in the corrected position, place a guide pin across the TMT joint. The trajectory should typically run from the dorsal-distal aspect of the first metatarsal base, aiming plantar-proximal into the medial cuneiform.
- Utilize intraoperative fluoroscopy to confirm adequate correction of the IMA, proper sagittal alignment, and optimal guide pin placement in all planes.
- Measure the guide pin depth. Overdrill the near cortex to create a gliding hole, and insert a partially threaded cannulated titanium screw (typically 3.5 mm or 4.0 mm) using standard AO interfragmentary compression technique. This is the "home run" screw that provides primary compression across the arthrodesis.
- Plate Application: Apply a four-hole, low-profile titanium locking plate over the dorsomedial aspect of the TMT joint.
- Secure the plate using four corresponding locked screws of varying lengths, adhering strictly to AO principles. The plate acts as a neutralization construct, protecting the interfragmentary screw from dorsal bending moments during weight-bearing.
Closure
- Irrigate all wounds copiously with sterile saline.
- Repair the medial capsule of the MTP joint using a strong absorbable suture (e.g., 2-0 Vicryl) to hold the hallux in neutral alignment.
- Close the subcutaneous layers and skin in a standard, layered fashion.
- Apply a sterile dressing and a modified Jones compression posterior splint to control edema and immobilize the foot and ankle in a neutral position.
POSTOPERATIVE CARE AND REHABILITATION
Historically, the Lapidus procedure required 6 to 8 weeks of strict non-weight-bearing (NWB) cast immobilization due to high nonunion rates. However, the advent of rigid locking plate technology has revolutionized the postoperative protocol.
- Phase 1 (Days 0 to 14): The patient remains strictly non-weight-bearing in the modified Jones splint. Elevation and strict adherence to rest are critical to allow for soft tissue healing and to minimize edema.
- Phase 2 (Weeks 2 to 6): At the first postoperative visit, sutures are removed. The patient is transitioned into a controlled ankle motion (CAM) walker boot. Depending on surgeon preference and the radiographic quality of the bone, patients may begin protected, progressive weight-bearing as tolerated.
- Phase 3 (Week 6 and Beyond): Radiographs are obtained to confirm progressive consolidation of the arthrodesis. Once clinical and radiographic union is evident, the patient is transitioned into a supportive, rigid-soled athletic shoe. Physical therapy is initiated to restore MTP joint range of motion, strengthen the intrinsic foot musculature, and normalize gait mechanics.
💡 Clinical Pearl: The Weight-Bearing Debate
Because of improvements in surgical technique and fixation methods—which have reduced the nonunion rate to less than 5%—the absolute necessity for prolonged cast immobilization has been heavily questioned. Several modern series describe immediate protected weight-bearing in a postoperative shoe or boot following Lapidus arthrodesis, provided that a robust locking plate construct was achieved intraoperatively.
JUVENILE AND ADOLESCENT HALLUX VALGUS (10 TO 19 YEARS OLD)
The management of hallux valgus in the pediatric and adolescent population represents a distinct and highly challenging clinical entity. It is a fundamental error to treat adolescent hallux valgus simply as an early-onset adult bunion. The pathophysiology, clinical presentation, and surgical outcomes differ significantly, requiring a highly specialized, algorithmic approach.
Unique Characteristics of Adolescent Hallux Valgus
Surgeons must consider adolescents with hallux valgus separately from adults for the following critical reasons:
- Atypical Pain Presentation: Unlike adults, pain at the medial eminence or beneath the lesser metatarsal heads (transfer metatarsalgia) may not be the primary presenting complaint. Often, the primary concern is cosmetic or difficulty with shoe wear.
- Absence of Bunion Hypertrophy: The classic "bunion" secondary to medial eminence exostosis and bursal hypertrophy is frequently a minor component of the deformity in youth. The prominence is almost entirely due to the angular deviation of the bone.
- Severe Metatarsus Primus Varus: A widened intermetatarsal angle with significant varus of the first metatarsal is almost universally present and is the primary driver of the pathology.
- Association with Hypermobile Flatfoot: Adolescent hallux valgus is frequently associated with a hypermobile pes planovalgus foot type. Pronation of the foot during the stance phase of gait unlocks the midtarsal joint, leading to hypermobility of the first ray and exacerbation of the valgus deforming forces on the hallux.
- High Recurrence Rates: Recurrence of the deformity following surgical correction is notoriously high in this demographic, especially if an underlying flatfoot deformity is ignored or inadequately addressed.
- Hallux Valgus Interphalangeus (HVI): An angular deformity within the hallux itself (at the interphalangeal joint) may be prominent. If HVI is overlooked during preoperative planning, correcting the MTP joint alone will result in an unsatisfactory, under-corrected clinical appearance.
- Strong Genetic Predisposition: The family history is frequently positive for hallux valgus, suggesting a strong hereditary component related to ligamentous laxity and bone morphology (e.g., a rounded first metatarsal head).
- Inefficacy of Soft Tissue Procedures: Soft tissue procedures alone (e.g., modified McBride procedure) are virtually guaranteed to fail in adolescents. The deformity is fundamentally osseous and structural.
- Necessity of Osteotomy: To obtain and maintain long-term correction, a single or double osteotomy of the first metatarsal (and occasionally the proximal phalanx, via an Akin osteotomy) is almost always necessary.
Indications and Timing for Surgical Intervention
The indications for surgical correction of hallux valgus in an adolescent are neither rigid nor universally agreed upon. The timing of the procedure remains one of the most debated topics in pediatric orthopedics.
The Physeal Closure Debate:
* Conservative Approach (Wait for Closure): Many well-documented series recommend postponing operative correction until the physes of the proximal phalanx and the first metatarsal are completely closed (typically around age 14-15 in girls, and 16-17 in boys). This approach avoids the risk of iatrogenic physeal arrest, which could lead to a shortened first ray and devastating secondary deformities. Proponents of this approach argue that surgery should only be offered for painful, radiographically progressive deformities after skeletal maturity.
* Aggressive Approach (Early Intervention): Conversely, other retrospective studies indicate that surgical intervention before 15 years of age—regardless of whether the physes are open or closed—yields the best long-term functional results. This is particularly true if the preservation of normal, pain-free metatarsophalangeal joint motion is considered the primary metric of success. Early correction of the osseous alignment may prevent the adaptive, irreversible soft-tissue contractures and joint congruency changes that occur over time.
Surgical Strategy in Adolescents
When surgery is indicated, the procedure must be tailored to the specific anatomical abnormalities present:
* Distal Metatarsal Articular Angle (DMAA): Adolescents frequently present with an increased DMAA. A standard closing base wedge osteotomy or Lapidus procedure will correct the IMA but may result in a hallux that points laterally if the DMAA is not addressed. A double osteotomy (e.g., proximal Lapidus combined with a distal Reverdin-Green osteotomy) may be required.
* Addressing the Flatfoot: If a severe hypermobile flatfoot is driving the deformity, isolated first ray surgery will likely fail. The surgeon must consider concomitant procedures to stabilize the medial column and hindfoot, such as a gastrocnemius recession, medial displacement calcaneal osteotomy, or subtalar arthroereisis, to alter the biomechanical environment and protect the hallux valgus correction.
⚠️ Pitfall: Ignoring Hallux Valgus Interphalangeus
Always evaluate the interphalangeal angle on the AP radiograph. If the hallux remains in valgus after the first metatarsal is perfectly realigned, an Akin osteotomy (medial closing wedge of the proximal phalanx) must be performed to achieve a rectus toe and ensure patient satisfaction.
You Might Also Like