Lateral Malleolus Lateral Approach: A Comprehensive Surgical & Anatomical Review

Key Takeaway
The lateral malleolus lateral approach is the standard surgical incision for distal fibula fractures, critical for anatomical reduction and stable internal fixation. It requires comprehensive knowledge of ankle epidemiology, detailed surgical anatomy (ligaments, tendons, neurovascular structures), and biomechanics. This understanding is crucial for surgeons to optimize patient outcomes and prevent long-term sequelae such as post-traumatic arthritis.
Detailed: Lateral Malleolus Lateral Approach for Surgeons
Introduction & Epidemiology
Ankle fractures represent a significant burden on healthcare systems globally, with the lateral malleolus being the most commonly fractured component. These injuries typically result from low-energy mechanisms in elderly individuals (often osteoporotic women) and higher-energy trauma in younger, active populations. The integrity of the ankle mortise is paramount for functional ambulation, making anatomical reduction and stable internal fixation of displaced or unstable lateral malleolar fractures a cornerstone of modern orthopedic trauma care. The lateral approach to the lateral malleolus is the workhorse incision for these injuries, providing direct access to the distal fibula and allowing for comprehensive assessment and management of associated syndesmotic or deltoid ligamentous pathology.
Epidemiologically, ankle fractures exhibit a bimodal distribution, with a peak incidence in adolescent and young adult males, often associated with sports injuries, and a second peak in elderly females, frequently linked to falls and diminished bone mineral density. The annual incidence is estimated to be approximately 100 to 150 per 100,000 person-years, with lateral malleolar fractures accounting for over 70% of all ankle fractures. The precise management of these injuries is critical to prevent long-term sequelae such as post-traumatic arthritis, chronic pain, and functional limitations.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate surgical anatomy and biomechanics of the ankle joint is crucial for successful outcomes.
Distal Fibula and Lateral Malleolus
The distal fibula forms the lateral aspect of the ankle mortise, articulating with the talus and contributing significantly to ankle stability. The lateral malleolus is the distal-most projection of the fibula, extending approximately 1 cm distal to the medial malleolus. Its subcutaneous location makes it easily palpable and accessible, but also susceptible to soft tissue compromise following trauma. The fibula acts as a lateral buttress, preventing excessive lateral talar shift and external rotation. Its anatomical position, length, and rotation are critical for maintaining ankle joint congruity.
Ligamentous Structures
The stability of the ankle joint is maintained by a complex interplay of osseous congruity and strong ligamentous restraints.
*
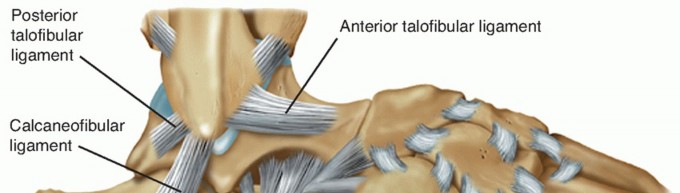
Lateral Collateral Ligament Complex:
Located on the lateral aspect of the ankle, these ligaments resist inversion and internal rotation.
*
Anterior Talofibular Ligament (ATFL):
Originates from the anterior aspect of the lateral malleolus and inserts onto the talar neck. It is the weakest and most commonly injured lateral ligament.
*
Calcaneofibular Ligament (CFL):
Courses obliquely from the tip of the lateral malleolus to the lateral surface of the calcaneus. It lies deep to the peroneal tendons.
*
Posterior Talofibular Ligament (PTFL):
The strongest of the three, originating from the posterior aspect of the lateral malleolus and inserting onto the posterior talus.
*
Syndesmotic Ligament Complex:
These ligaments connect the distal tibia and fibula, maintaining the integrity of the distal tibiofibular joint (syndesmosis).
*
Anterior Inferior Tibiofibular Ligament (AITFL):
Connects the anterior tubercle of the tibia to the anterior border of the fibula.
*
Posterior Inferior Tibiofibular Ligament (PITFL):
Connects the posterior tubercle of the tibia to the posterior fibula.
*
Interosseous Ligament:
A continuation of the interosseous membrane, providing significant stability.
*
Medial Deltoid Ligament Complex:
A strong, fan-shaped ligament on the medial side, resisting eversion and external rotation. It comprises superficial and deep layers. Injury to the deltoid ligament, often indicated by medial clear space widening on mortise radiographs, signifies medial instability and is frequently associated with lateral malleolar fractures, particularly supination-external rotation (SER) injuries.
Tendons and Neurovascular Structures
- Peroneal Tendons: The peroneus longus and brevis tendons run in a groove posterior to the lateral malleolus, contained within the peroneal retinaculum. The peroneus brevis inserts onto the base of the fifth metatarsal, while the peroneus longus courses under the cuboid to insert on the medial cuneiform and first metatarsal base. Care must be taken to protect these tendons during dissection.
-
Neurovascular Structures:
- Superficial Peroneal Nerve: Provides sensation to the dorsum of the foot (excluding the first web space). It typically emerges from the deep fascia approximately 10-15 cm proximal to the tip of the lateral malleolus, then divides into intermediate dorsal cutaneous and medial dorsal cutaneous branches. It is at risk during incisions extending anteriorly or with excessive traction.
- Sural Nerve: Provides sensation to the posterolateral aspect of the leg and lateral foot. It runs along the posterior border of the fibula and lateral malleolus, often in close proximity to the short saphenous vein. It is vulnerable during posterior dissection or placement of posterolateral plates.
- Short Saphenous Vein: Accompanies the sural nerve and drains into the popliteal vein. It is highly variable in its course but generally lies superficially along the posterior border of the lateral malleolus. It can be seen pre-exsanguination.
-
Biomechanics
The ankle mortise functions as a highly congruent hinge joint, allowing primary dorsiflexion and plantarflexion. The fibula plays a critical role in maintaining talar stability within the mortise. Shortening, external rotation, or lateral translation of the fibula, even by a few millimeters, can significantly alter joint contact pressures, lead to talar shift, and predispose to early post-traumatic arthritis. Restoration of fibular length, rotation, and alignment is therefore paramount in the surgical management of lateral malleolar fractures.
Indications & Contraindications
The decision for operative versus non-operative management of lateral malleolus fractures hinges on fracture stability, displacement, and the presence of associated injuries to the medial structures or syndesmosis.
Indications for Operative Fixation
- Displaced Lateral Malleolus Fractures: Any fracture with significant displacement (e.g., >2mm articular step-off, >2mm shortening of the fibula).
-
Unstable Ankle Fractures:
- Medial Instability: Widening of the medial clear space on AP or mortise views (typically >4mm compared to the superior clear space), indicating deltoid ligament rupture or medial malleolus fracture.
- Syndesmotic Instability: Widening of the syndesmosis (tibiofibular clear space >6mm on AP/mortise views, tibiofibular overlap <6mm on AP or <10mm on mortise), positive hook test intraoperatively, or stress radiography showing instability.
- Talar Shift: Any lateral or posterior shift of the talus within the mortise.
- Open Fractures: Require urgent surgical debridement and stabilization.
- Associated Injuries: Fractures of the posterior malleolus requiring fixation (often necessitates a posterolateral approach, but the lateral approach can provide some access), or complex pilon fractures where fibular reconstruction is part of the overall strategy.
- Specific Fracture Patterns: Lauge-Hansen classifications (e.g., Supination-External Rotation stages II-IV, Pronation-Abduction, Pronation-External Rotation), and Weber B or C fractures with instability.
Contraindications for Operative Fixation
-
Absolute Contraindications:
- Severe active infection (osteomyelitis).
- Extremely poor soft tissue envelope precluding safe incision and closure (e.g., severe degloving injury, full-thickness skin loss without viable soft tissue for coverage).
- Medically unstable patient unable to tolerate anesthesia or surgery (e.g., severe cardiac compromise, uncontrolled sepsis).
-
Relative Contraindications:
- Non-displaced, stable lateral malleolus fractures without medial or syndesmotic instability. These can often be managed non-operatively with bracing or casting.
- Severe peripheral vascular disease or diabetes with high risk of wound healing complications.
- Extremely frail or debilitated patients with limited functional goals.
- Morbid obesity, which increases surgical risk and may complicate implant selection and postoperative rehabilitation.
- Pre-existing severe neuropathy or Charcot arthropathy.
Operative vs. Non-Operative Indications
| Feature | Operative Indication | Non-Operative Indication |
|---|---|---|
| Fracture Displacement | >2mm articular step-off or fibular shortening, talar shift | <2mm displacement, stable |
| Medial Instability | Medial clear space widening (>4mm) or displaced medial malleolus fracture | No medial clear space widening, intact deltoid |
| Syndesmotic Instability | Widening on radiographs, positive hook test, diastasis | Stable syndesmosis (no widening, no pain with stress) |
| Associated Injuries | Displaced posterior malleolus fracture, open fracture | Isolated, non-displaced lateral malleolus fracture |
| Patient Status | Healthy, able to tolerate surgery | Medically frail, significant comorbidities (relative) |
| Soft Tissue | Intact, viable soft tissue | Severe soft tissue compromise (absolute contraindication for immediate ORIF) |
| Fracture Pattern | Lauge-Hansen SER II-IV, PA, PER; Weber B/C with instability | Lauge-Hansen SER I; Weber A, or stable Weber B |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning and meticulous patient positioning are critical for successful surgical outcomes and complication avoidance.
Pre-Operative Planning
- Clinical Assessment: Thorough history and physical examination, focusing on neurovascular status, soft tissue integrity (swelling, blistering, open wounds), and associated injuries. Note any pre-existing conditions (diabetes, PVD, neuropathy).
-
Radiographic Evaluation:
- Standard Ankle Series: Anteroposterior (AP), lateral, and mortise views are mandatory.
- Stress Radiographs: May be indicated to assess deltoid or syndesmotic instability if routine views are inconclusive.
- Contralateral Ankle Views: Useful for comparison of fibular length and syndesmotic measurements.
- CT Scan: Indicated for complex fracture patterns, significant comminution, articular involvement, or to delineate posterior malleolus fractures.
- MRI: Rarely indicated acutely, but may be useful for assessing purely ligamentous injuries (e.g., syndesmotic disruption without fibular fracture) or pre-existing pathology.
-
Implants and Equipment:
- Selection of plate and screw system: Options include 1/3 tubular plates, locking plates (e.g., precontoured fibular plates), anti-glide plates, or hook plates. Consideration for screw length (bicortical vs. unicortical).
- Syndesmotic fixation: Syndesmotic screws (cortical screws, typically 3.5mm or 4.5mm), suture button devices (e.g., TightRope™).
- Reduction clamps, small fragment set, drills, depth gauges.
- Fluoroscopy unit (C-arm).
- Anesthesia and Prophylaxis: General or regional anesthesia (spinal/epidural) is common. Pre-operative prophylactic antibiotics (e.g., Cefazolin) should be administered within 60 minutes of incision. Deep vein thrombosis (DVT) prophylaxis should be initiated as per institutional protocols.
Patient Positioning
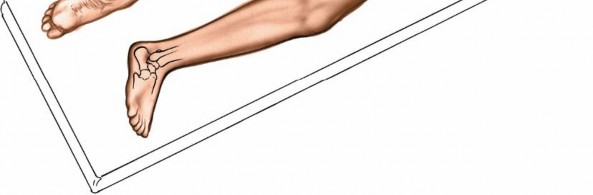
- Operating Table: Position the patient supine on the operating table. A radiolucent table is preferred to allow for intraoperative fluoroscopy without repositioning.
- Limb Exsanguination and Tourniquet: The affected limb is elevated for 3 to 5 minutes to achieve exsanguination, then a pneumatic tourniquet is inflated on the proximal thigh. Tourniquet pressure should be set at 100 mmHg above systolic blood pressure or 250-300 mmHg.
-
Medial Rotation:
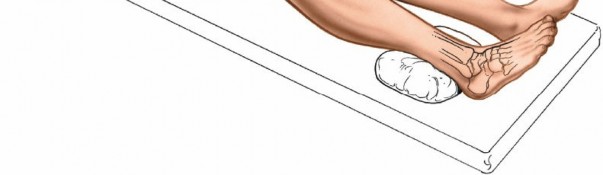
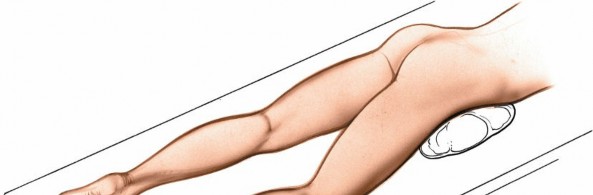
To optimize access to the lateral malleolus, a sandbag or bolster is placed under the ipsilateral buttock of the affected limb. This maneuver internally rotates the entire limb, bringing the lateral malleolus into a more anteriorly oriented position, making dissection and plate application easier.
-
 -
-
- Sterile Preparation and Draping: The limb is prepped from the mid-calf to the toes, including the foot, using an antiseptic solution. Sterile draping isolates the operative field.
Detailed Surgical Approach / Technique
The lateral approach to the lateral malleolus is a direct and versatile incision, providing excellent exposure for fibular fracture management.
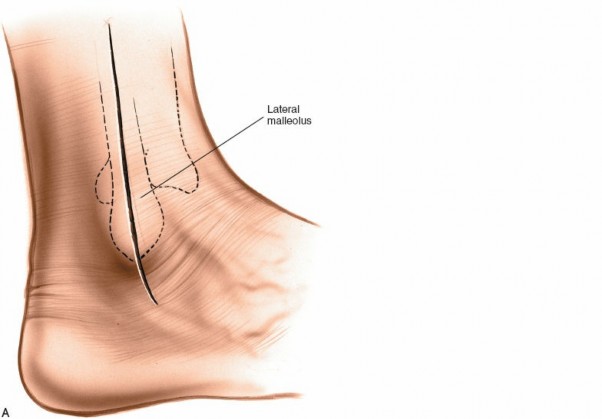
Landmarks and Incision
- Palpation: Carefully palpate the subcutaneous surface of the fibula and the lateral malleolus at its distal end. Identify the posterior border of the fibula.
-
Short Saphenous Vein:
Before exsanguination, observe the course of the short saphenous vein, typically running along the posterior border of the lateral malleolus. This aids in its intraoperative identification and protection.
-
-
-
Incision:
Make a longitudinal skin incision approximately 10 to 15 cm in length. The incision is typically centered over the fracture site and extends distally to the tip of the lateral malleolus, continuing for an additional 2 cm. Proximally, it extends along the posterior margin of the fibula. For higher fibular fractures, the incision can be extended proximally as needed. The incision should be carefully planned to avoid skin tension lines and minimize the risk of wound complications.
-

-
Dissection
- Skin and Subcutaneous Tissues: Incise the skin and subcutaneous tissues with a scalpel. Bleeding vessels should be cauterized.
-
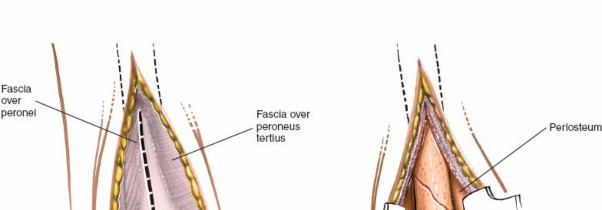
Neurovascular Protection:
- Sural Nerve and Short Saphenous Vein: These structures lie superficially along the posterior border of the incision. Identify and gently retract them posteriorly. Care must be taken to avoid direct injury or excessive stretch.
- Superficial Peroneal Nerve: Although less commonly encountered in a posterior fibular incision, branches of the superficial peroneal nerve may cross the surgical field, especially if the incision curves anteriorly. Blunt dissection and careful retraction are crucial.
- Internervous Plane: There is no true internervous plane in this approach because the dissection is being performed directly down to a subcutaneous bone. The fibula, particularly its lateral and posterior aspects, is covered by only thin soft tissue layers (skin, subcutaneous fat, and periosteum). The key is meticulous sharp and blunt dissection directly to the fibular periosteum.
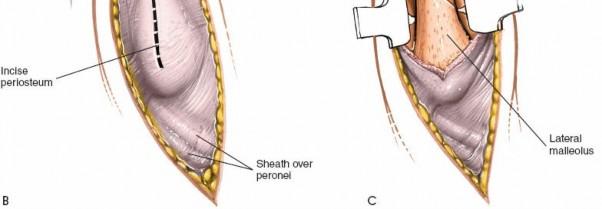
- Periosteal Incision: Once the fibula is exposed, make a longitudinal incision in the periosteum directly over the fracture site and extending proximally and distally along the bone. Elevate the periosteum carefully using a Cobb elevator or similar instrument to expose the fracture fragments. Minimize periosteal stripping to preserve blood supply, especially in comminuted fractures.
Fracture Exposure and Assessment
- Debridement: Clear the fracture hematoma, necrotic tissue, and any loose fragments that are not amenable to fixation and may impede reduction.
- Fragment Identification: Thoroughly identify all fracture fragments, assessing the fracture pattern, degree of comminution, and any articular involvement. Confirm the stability of the fracture under gentle stress.
Reduction Techniques
The primary goal is anatomical reduction of the fibula, restoring its length, rotation, and alignment.
1.
Direct Reduction:
Use small pointed reduction clamps (e.g., Verbrugge, small fragment clamps) to grasp the main proximal and distal fragments. Apply gentle traction and rotational forces to achieve reduction.
2.
Indirect Reduction:
For highly comminuted fractures or significant shortening, indirect reduction techniques may be employed.
*
Ligamentotaxis:
Distraction across the ankle joint (e.g., using an external fixator or manual traction) can help realign the fibula by tensioning the intact ligaments.
*
Leverage:
Use a periosteal elevator or a K-wire as a joystick to manipulate fragments.
3.
Temporary Fixation:
Once anatomical reduction is achieved, maintain it with temporary K-wires, which can be placed perpendicularly to the fracture line or in an oblique fashion to provide rotational control.
4.
Mortise Restoration:
Crucially, verify the restoration of the ankle mortise using fluoroscopy (AP, lateral, and mortise views). Ensure that the talus is centered and that there is no medial clear space widening.
Fixation Strategies
The choice of fixation depends on the fracture pattern, comminution, bone quality, and surgeon preference.
1.
Plate Osteosynthesis:
*
Plate Selection:
Common choices include 1/3 tubular plates, pre-contoured locking plates (which are particularly useful in osteoporotic bone or comminuted fractures), or specialized fibular plates.
*
Plate Positioning:
The plate is typically contoured and applied to the lateral or posterolateral aspect of the fibula. Applying it posterolaterally can enhance stability by placing it in tension for oblique fractures (anti-glide principle).
*
Screw Placement:
*
Lag Screws:
For oblique fractures, a lag screw placed across the fracture site prior to plate application provides interfragmentary compression. Alternatively, a lag screw can be placed through a plate hole.
*
Cortical Screws:
Bicortical screws are generally preferred for maximum purchase. Ensure adequate thread engagement in both cortices.
*
Locking Screws:
Used with locking plates, these provide angular stability, preventing screw pull-out and collapse, especially useful in comminuted fractures or poor bone quality.
*
Contouring:
The plate must be meticulously contoured to match the natural curvature of the fibula to avoid creating new stress risers or malalignment.
*
-
Syndesmotic Fixation:
- Assessment: After fibular fixation, reassess syndesmotic stability. This is typically done by external rotation stress testing, manual hook test (grasping the fibula and attempting to translate it), or using a fluoroscopic stress view (Cotton test). If the syndesmosis is found to be unstable, fixation is required.
-
Technique:
- Syndesmotic Screw(s): One or two cortical screws (e.g., 3.5mm or 4.5mm) are typically placed from the fibula across the interosseous membrane into the tibia. The screws should be placed approximately 2-4 cm proximal to the ankle joint line, aiming postero-medially, ideally engaging three cortices (tricortical fixation). Care must be taken to avoid overtightening, which can lead to loss of ankle dorsiflexion or screw breakage. Traditionally, the foot is dorsiflexed to neutral during screw insertion to ensure optimal talar position.
- Suture Button Devices: These are increasingly popular and consist of cortical buttons connected by a high-strength suture, allowing for dynamic stabilization of the syndesmosis. They are often associated with a lower rate of reoperation for hardware removal.
-

Closure
- Irrigation: Thoroughly irrigate the surgical site with sterile saline solution.
- Hemostasis: Ensure meticulous hemostasis.
- Periosteal Repair: If feasible without undue tension, approximate the incised periosteum.
- Subcutaneous Closure: Close the subcutaneous tissue layer using absorbable sutures.
- Skin Closure: Close the skin with non-absorbable sutures or staples.
- Dressing and Immobilization: Apply a sterile dressing. A well-padded posterior splint or short leg cast is applied to provide immediate post-operative immobilization and support.
Complications & Management
Despite meticulous surgical technique, complications can arise following operative fixation of lateral malleolus fractures. Comprehensive understanding and proactive management are paramount.
Common Complications and Management Strategies
| Complication | Incidence (%) | Salvage / Management Strategies Initial Patient Positioning is typically supine with the arm of the affected limb abducted. The foot is placed towards the distal end of the table for unimpeded access to fluoroscopy. A small bump under the ipsilateral buttock will internally rotate the leg, bringing the lateral malleolus into a more accessible anterior position.
Surgical Exposure and Fracture Management
- Skin Incision and Dissection: The initial skin incision is made carefully, extending through the subcutaneous tissue to the deep fascia overlying the fibula. Identify the short saphenous vein and sural nerve posteriorly, retracting them safely.
- Periosteal Exposure: Incise the periosteum longitudinally along the palpable border of the fibula, centered over the fracture. Subperiosteal dissection is performed anteriorly and posteriorly to expose the fracture fragments. Minimize extensive stripping to preserve soft tissue attachments and blood supply.
- Fracture Assessment: Debride any hematoma or debris from the fracture site. Assess the fracture pattern, comminution, and alignment.
-
Reduction:
- Length Restoration: This is paramount. Manual traction can help restore length. For significant shortening, a temporary external fixator can be applied from the tibia to the talus/calcaneus to distract the joint and achieve ligamentotaxis.
- Rotation: Ensure anatomical rotation of the distal fibula. The fibula naturally has an anterior bow.
- Alignment: Reduce any angulation or translation.
- Temporary Fixation: Once length, rotation, and alignment are restored, secure the reduction with small-pointed reduction clamps or K-wires.
-
Definitive Fixation – Plate Osteosynthesis:
- Plate Contouring: Select an appropriate plate (e.g., 1/3 tubular, locking plate, hook plate). Contour the plate precisely to the lateral or posterolateral surface of the fibula using a bending press or bending irons. The plate should lie flush against the bone.
- Plate Placement: For simple transverse or short oblique fractures, a lateral plate may suffice. For long oblique or comminuted fractures, a posterolateral "anti-glide" plate can be advantageous. The anti-glide principle uses the plate to buttress the posterior aspect of an oblique fracture, preventing posterior and superior migration of the distal fragment.
-
Screw Insertion Sequence:
- Typically, place a screw (often a lag screw, if applicable) across the most stable part of the fracture to provide interfragmentary compression. This can be placed outside the plate or through an oblong plate hole.
- Secure the plate proximally and distally with cortical or locking screws. For cortical screws, ensure bicortical purchase. For locking screws, angle guidance is crucial.
- Verify fibular length and alignment using intraoperative fluoroscopy (AP, lateral, and mortise views). Confirm absence of talar shift and restoration of the syndesmosis.
-

-
Syndesmotic Assessment and Fixation:
- Intraoperative Stress Test: After definitive fibular fixation, assess syndesmotic stability. The "Cotton Test" or "External Rotation Stress Test" are commonly employed. With the fibula anatomically reduced and fixed, grasp the fibula with a bone clamp and apply an external rotation force while viewing the ankle mortise with fluoroscopy. Medial clear space widening of >2mm relative to the superior clear space, or loss of tibiofibular overlap, indicates instability.
-
Syndesmotic Screw Placement:
If unstable, a syndesmotic screw (typically 3.5mm or 4.5mm cortical screw) or a suture button device is used.
- Position the screw 2-4 cm proximal to the ankle joint line, traversing from the fibula (usually through one of the plate holes or a dedicated drill hole) into the tibia.
- Aim approximately 30 degrees posterior from the coronal plane and 15 degrees superior from the transverse plane to maximize purchase.
- While controversially debated, traditionally, the foot is dorsiflexed to a neutral position (0 degrees) during screw insertion to prevent overtightening and allow for physiological movement. Engaging three cortices (tricortical fixation) is generally preferred over four cortices (quadricortical) to mitigate the risk of overtightening.
- The use of one or two screws remains surgeon preference, with some studies suggesting no significant difference in outcome.
- Suture Button Devices: These are dynamic fixation options that allow some physiologic motion and typically do not require removal. They are placed similarly, but with a drill hole through both cortices of the fibula and tibia for button passage.
-

Closure
- Irrigation and Hemostasis: Copious irrigation of the wound. Achieve meticulous hemostasis to prevent hematoma formation.
- Periosteal/Fascial Closure: Close the deep fascial layer/periosteum if possible, without tension, using absorbable sutures.
- Subcutaneous Closure: Approximate subcutaneous tissues using absorbable sutures to obliterate dead space.
- Skin Closure: Close the skin with non-absorbable sutures or staples.
- Dressing and Immobilization: Apply a sterile dressing. A well-padded posterior splint or short leg cast is applied to maintain the ankle in a neutral position and protect the fixation.
Complications & Management
Despite meticulous surgical technique, complications can arise following operative fixation of lateral malleolus fractures. Comprehensive understanding and proactive management are paramount.
Common Complications and Management Strategies
| Complication | Incidence (%) | Salvage / Management Strategies ## Introduction & Epidemiology
Ankle fractures are among the most common traumatic injuries managed by orthopedic surgeons, presenting a wide spectrum from isolated, stable fractures to complex intra-articular injuries with associated ligamentous pathology. The lateral malleolus, specifically the distal fibula, is the most frequently affected osseous structure. These injuries are associated with significant morbidity, including chronic pain, instability, and post-traumatic osteoarthritis, underscoring the importance of accurate diagnosis and appropriate treatment.
Epidemiologically, ankle fractures exhibit a bimodal distribution. A higher incidence is observed in younger, active males due to high-energy sports-related trauma, and in older, often osteoporotic, females due to low-energy falls. The annual incidence of ankle fractures is reported to be between 100 to 200 per 100,000 person-years, with lateral malleolus fractures constituting approximately 70-80% of all ankle fractures. The increasing prevalence of osteoporotic fractures in an aging population suggests a continued rise in the overall burden of these injuries. Surgical intervention, particularly open reduction and internal fixation (ORIF) via the lateral approach, is frequently indicated for displaced or unstable lateral malleolus fractures to restore ankle mortise congruity and optimize long-term functional outcomes.
Surgical Anatomy & Biomechanics
A detailed understanding of the osseous and soft tissue anatomy, along with the biomechanical principles governing ankle stability, is fundamental for surgeons utilizing the lateral malleolus approach.
Osseous Structures
- Fibula: The distal fibula forms the lateral malleolus, a crucial component of the ankle mortise. It extends approximately 1 cm distal to the medial malleolus and posteriorly to the talus. The fibula acts as a lateral buttress, preventing lateral translation and external rotation of the talus. Its anatomical length, rotation, and alignment are critical determinants of ankle joint congruity and load distribution.
- Tibia: The distal tibia forms the medial malleolus and the posterior malleolus (if fractured), as well as the tibial plafond (the superior articular surface). The incisura fibularis of the tibia provides an articulation for the fibula, forming the distal tibiofibular joint.
- Talus: The talus articulates with the tibia and fibula, forming the primary ankle joint. Its dome-shaped trochlea fits snugly within the ankle mortise. Any loss of congruity due to fracture displacement or ligamentous injury can significantly alter joint mechanics.
Ligamentous Structures
The stability of the ankle is maintained by a robust ligamentous complex.
*
Lateral Collateral Ligaments:
Comprising three distinct bands that resist inversion and internal rotation.
*
Anterior Talofibular Ligament (ATFL):
Originates from the anterior margin of the lateral malleolus and inserts onto the talar neck. It is the weakest and most frequently injured lateral ligament.
*
Calcaneofibular Ligament (CFL):
Extends from the tip of the lateral malleolus to the lateral aspect of the calcaneus, deep to the peroneal tendons.
*
Posterior Talofibular Ligament (PTFL):
The strongest of the lateral ligaments, connecting the posterior aspect of the lateral malleolus to the posterior talus.
*
Syndesmotic Ligaments:
These ligaments connect the distal tibia and fibula, forming the distal tibiofibular syndesmosis, which maintains the integrity of the ankle mortise.
*
Anterior Inferior Tibiofibular Ligament (AITFL):
Connects the anterior tubercle of the tibia to the anterior aspect of the fibula.
*
Posterior Inferior Tibiofibular Ligament (PITFL):
Connects the posterior tubercle of the tibia to the posterior aspect of the fibula. This ligament is stronger and thicker than the AITFL.
*
Interosseous Ligament:
A robust fibrous band, continuous with the interosseous membrane, providing significant stability to the syndesmosis.
*
Medial Deltoid Ligament Complex:
A strong, fan-shaped ligament originating from the medial malleolus and inserting onto the talus, navicular, and calcaneus. It resists eversion and external rotation. Injury to the deep component of the deltoid ligament (tibiotalar part) is often indicative of significant medial instability, frequently associated with lateral malleolus fractures.
Tendons and Neurovascular Structures
- Peroneal Tendons: The peroneus longus and brevis tendons run posterior to the lateral malleolus within a fibro-osseous groove, deep to the superior and inferior peroneal retinacula. The peroneus brevis is anterior to the longus at the malleolus. Careful retraction is necessary to protect these tendons and their retinacula.
-
Neurovascular Structures:
- Sural Nerve: Arises from the tibial and common peroneal nerves, runs with the short saphenous vein, and provides sensation to the posterolateral lower leg and lateral foot. It typically lies along the posterior border of the fibula and lateral malleolus and is vulnerable during posterior dissection or plate placement.
- Short Saphenous Vein: Accompanies the sural nerve superficially along the posterior border of the lateral malleolus and drains into the popliteal vein. It is easily identifiable pre-exsanguination.
- Superficial Peroneal Nerve: Pierces the deep fascia proximally (typically 10-15 cm above the lateral malleolus) and divides into terminal branches that supply sensation to the dorsum of the foot. It is at risk with incisions that extend too far anteriorly or with excessive anterior retraction.
-

Biomechanics of Ankle Stability
The ankle joint is inherently stable due to its congruent mortise and strong ligamentous restraints. The fibula plays a critical role as a lateral buttress. Even small changes in fibular length (<2-3mm shortening), rotation, or alignment can significantly alter the contact pressures across the talar dome, leading to premature articular degeneration and post-traumatic arthritis. Restoration of the fibular anatomy is paramount for restoring normal ankle kinematics and load distribution. The integrity of the syndesmosis is equally important, preventing pathologic widening and talar shift.
Indications & Contraindications
The decision to proceed with operative fixation for a lateral malleolus fracture is based on a comprehensive assessment of fracture stability, displacement, associated injuries, and patient factors.
Indications for Operative Fixation
Operative management via the lateral approach is indicated for:
*
Displaced Lateral Malleolus Fractures:
* Any articular step-off >2mm.
* Fibular shortening >2mm compared to the contralateral side.
* Lateral or posterior talar shift/subluxation.
*
Unstable Ankle Fractures:
*
Medial Instability:
Widening of the medial clear space on AP or mortise radiographs (>4mm or > superior clear space), indicative of deep deltoid ligament rupture or displaced medial malleolus fracture.
*
Syndesmotic Instability:
* Widening of the tibiofibular clear space (>6mm on AP or mortise views).
* Loss of tibiofibular overlap (<6mm on AP or <10mm on mortise views).
* Positive intraoperative stress tests (e.g., external rotation stress test, hook test).
*
Open Fractures:
Require urgent surgical debridement, washout, and stabilization.
*
Associated Posterior Malleolus Fracture:
If displaced and large enough to compromise stability or function (typically >25% of the articular surface or >2mm displacement). While primary access for the posterior malleolus may be a posterolateral approach, the lateral approach allows for fibular fixation and often for assessment of posterior malleolus stability.
*
Polytrauma Patients:
Early stabilization of ankle fractures in poly-traumatized patients can contribute to overall patient stability and facilitate rehabilitation.
*
Specific Fracture Classifications:
* Lauge-Hansen classifications such as Supination-External Rotation (SER) Stage II-IV, Pronation-Abduction (PA), or Pronation-External Rotation (PER).
* Weber B and C fractures with evidence of instability.
Contraindications for Operative Fixation
-
Absolute Contraindications:
- Severe Soft Tissue Compromise: Full-thickness skin loss, severe degloving, or severe fracture blisters that preclude safe incision and wound closure. In such cases, external fixation with delayed ORIF or definitive external fixation may be considered.
- Active Local or Systemic Infection: Active osteomyelitis or sepsis.
- Patient Unable to Tolerate Anesthesia/Surgery: Severe uncompensated medical comorbidities.
-
Relative Contraindications:
- Non-Displaced, Stable Lateral Malleolus Fractures: Without medial or syndesmotic instability, these are typically managed non-operatively with a cast or boot.
- Pre-Existing Severe Peripheral Vascular Disease or Uncontrolled Diabetes: Significantly increases the risk of wound complications and infection.
- Morbid Obesity: Increases surgical complexity and risk of complications, though often still indicated for unstable fractures.
- Severe Osteopenia/Osteoporosis: While not an absolute contraindication (often an indication for locking plates), extremely poor bone quality may challenge stable fixation.
- Limited Functional Goals: In some very elderly or debilitated patients, a non-operative approach may be chosen, accepting some malunion to avoid surgical risks.
Operative vs. Non-Operative Indications Table
| Feature | Operative Indication | Non-Operative Indication (Generally) |
|---|---|---|
| Fracture Displacement | >2mm articular step-off or fibular shortening, talar shift | <2mm displacement, anatomically stable |
| Medial Stability | Medial clear space widening (>4mm), displaced medial malleolus fx | No medial clear space widening, intact deltoid (clinically/radiographically) |
| Syndesmotic Stability | Radiographic widening, positive intraoperative stress test, diastasis | Stable syndesmosis (no widening or laxity) |
| Associated Injuries | Displaced posterior malleolus fracture, open fracture | Isolated lateral malleolus fracture with no other significant injuries |
| Soft Tissue Status | Intact, viable soft tissue envelope | Severe soft tissue compromise (e.g., extensive blistering, necrosis) |
| Patient Comorbidities | Medically optimized, able to tolerate surgery | Significant uncompensated comorbidities precluding surgery |
| Fracture Pattern (e.g.) | Lauge-Hansen SER II-IV, PA, PER; Weber B/C with instability | Lauge-Hansen SER I; stable Weber A, or stable Weber B |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and careful patient positioning are paramount for optimizing surgical exposure, minimizing complications, and ensuring reproducible outcomes.
Pre-Operative Planning
-
Clinical Assessment:
- Thorough history: Mechanism of injury, previous ankle injuries, medical comorbidities (diabetes, peripheral vascular disease, neuropathy, smoking status).
- Physical examination: Assess skin integrity (blisters, open wounds, edema), neurovascular status (dorsalis pedis and posterior tibial pulses, sensation in superficial peroneal, sural, and tibial nerve distributions), and limb alignment.
- Timing of surgery: Open fractures require urgent management. Closed fractures with significant swelling or blistering may benefit from a delayed approach (5-10 days) after soft tissue subsidence to reduce wound complications.
-
Radiographic Evaluation:
- Standard Ankle Series: AP, lateral, and mortise views are essential. Evaluate fibular length, rotation, comminution, articular congruity, and presence of medial clear space widening or syndesmotic diastasis.
- Stress Radiographs: May be utilized to assess syndesmotic or deltoid ligament instability if not obvious on routine views.
- Contralateral Ankle Views: Useful for baseline comparison of fibular length and syndesmotic measurements.
- Computed Tomography (CT) Scan: Indicated for complex fracture patterns, significant comminution, suspected articular involvement (e.g., anterior process of calcaneus, talar dome), or to delineate the size and displacement of posterior malleolus fragments.
- Magnetic Resonance Imaging (MRI): Rarely indicated acutely but can define purely ligamentous injuries (e.g., syndesmotic disruption without fibular fracture).
-
Implant Selection:
- Determine the type of plate (e.g., 1/3 tubular, pre-contoured locking plate, anti-glide plate, hook plate) and screw sizes (e.g., 3.5mm cortical, 3.5mm locking).
- Plan for syndesmotic fixation (e.g., 3.5mm or 4.5mm cortical screws for static fixation, or suture button devices for dynamic fixation).
- Ensure availability of reduction clamps, provisional fixation (K-wires), and appropriate instruments.
-
Anesthesia and Prophylaxis:
- Anesthesia: General or regional anesthesia (e.g., spinal or epidural block) is common. A popliteal block can be a useful adjunct for postoperative pain management.
- Antibiotics: Administer intravenous prophylactic antibiotics (e.g., Cefazolin) within 60 minutes prior to incision.
- DVT Prophylaxis: Implement according to institutional protocols (e.g., low-molecular-weight heparin or mechanical compression devices).
Patient Positioning
- Operating Table: Position the patient supine on a radiolucent operating table. This allows for unrestricted intraoperative fluoroscopy in multiple planes without repositioning the patient.
-
Limb Exsanguination and Tourniquet:
- Elevate the affected limb for 3 to 5 minutes to achieve exsanguination of venous blood.
- Inflate a pneumatic tourniquet on the proximal ipsilateral thigh to a pressure typically 100 mmHg above the patient's systolic blood pressure, or 250-300 mmHg.
-
Medial Rotation of the Limb:
- Place a sandbag or bolster under the ipsilateral buttock of the affected limb. This maneuver internally rotates the entire limb, bringing the lateral malleolus and fibula into a more anteriorly oriented position. This facilitates direct access to the posterior border of the fibula, simplifies plate contouring, and reduces the need for excessive retraction of soft tissues.
-
 -

- Sterile Preparation and Draping: Prepare the limb circumferentially from the mid-calf to the toes, including the foot, using an antiseptic solution. Sterile drape the limb, leaving the toes exposed for assessment of capillary refill if a tourniquet is used for an extended period, or for manipulation if required.
Detailed Surgical Approach / Technique
The lateral approach to the lateral malleolus is a direct, extensile incision providing excellent exposure for fibular reduction and fixation.
Landmarks and Incision
- Palpation: Accurately palpate the subcutaneous border of the fibula and its distal-most extent, the lateral malleolus. Identify the palpable fracture deformity.
-
Short Saphenous Vein:
Before exsanguination and tourniquet inflation, visualize the course of the short saphenous vein, which typically runs superficially along the posterior border of the lateral malleolus. This aids in intraoperative identification and protection.
-

-
-
Incision:
Make a longitudinal skin incision, typically 10 to 15 cm in length. The incision should be centered over the fracture site. It is made along the posterior margin of the fibula, extending distally to the tip of the lateral malleolus and continuing approximately 2 cm beyond. Proximally, it extends along the posterior fibular shaft as needed for adequate exposure of the fracture fragments. In complex or comminuted fractures, the incision may need to be slightly longer to ensure full visualization. Careful planning to avoid pressure areas or skin tension is crucial, especially in the setting of soft tissue swelling.
-

-
Dissection
- Skin and Subcutaneous Tissues: Incise the skin with a scalpel. Extend the dissection through the subcutaneous fat using a scalpel or electrocautery, taking care to achieve hemostasis.
-
Neurovascular Protection:
- Sural Nerve and Short Saphenous Vein: These structures lie superficially along the posterior aspect of the incision. Identify them early. Using careful blunt dissection, gently retract them posteriorly to protect them from direct injury or excessive stretch.
- Superficial Peroneal Nerve: While less commonly in the direct field of a posterior fibular incision, distal branches may be encountered if the incision extends more anteriorly. Maintain sharp dissection along the bone to avoid straying into nerve pathways.
- Internervous Plane: There is no true internervous plane in the traditional sense for this approach, as the fibula is a largely subcutaneous bone distally. The dissection proceeds directly through the subcutaneous fat to the periosteum. This direct access necessitates careful soft tissue handling to protect the overlying neurovascular structures.
- Periosteal Incision and Elevation: Once the fibula is exposed, make a longitudinal incision in the periosteum directly over the fracture site and extending proximally and distally. Using a periosteal elevator (e.g., Cobb elevator), carefully elevate the periosteum to expose the fracture fragments. Minimize periosteal stripping to preserve blood supply, particularly in comminuted fractures, where excessive stripping can devitalize fragments.
Fracture Exposure and Assessment
- Debridement: Remove any hematoma, necrotic tissue, or loose cancellous bone fragments that are not amenable to fixation or may impede reduction. Retain any large, well-vascularized fragments.
- Fragment Identification: Thoroughly visualize and assess the fracture pattern, including comminution, obliquity, and any associated impaction or articular involvement. This guides the choice of fixation.
Reduction Techniques
The goal is anatomical reduction of the fibula, restoring its length, rotation, and alignment.
1.
Direct Reduction:
Use small pointed reduction clamps (e.g., Verbrugge, small fragment clamps, articulated reduction forceps) to grasp the main proximal and distal fragments. Apply gentle traction and rotational forces to achieve accurate reduction. Fluoroscopic guidance helps confirm alignment.
2.
Indirect Reduction:
For highly comminuted fractures or significant shortening:
*
Ligamentotaxis:
Distraction across the ankle joint, either manually or with a temporary external fixator, can help restore fibular length by tensioning intact ligaments and soft tissues.
*
"Joy-stick" Technique:
K-wires or a periosteal elevator can be used as a joystick to manipulate fragments into position.
3.
Temporary Fixation:
Once anatomical reduction is achieved, maintain it with provisional K-wires inserted perpendicularly to the fracture plane or obliquely to control rotation. These K-wires should not interfere with planned plate placement.
4.
Mortise Restoration:
Critically, verify the restoration of the ankle mortise. Utilize intraoperative fluoroscopy with AP, lateral, and mortise views to confirm:
* Anatomical fibular length (compare to contralateral side if doubt exists).
* Absence of talar shift.
* Congruity of the joint.
* No medial clear space widening (indicating stable deltoid or healed medial malleolus).
Definitive Fixation Strategies
The choice of fixation depends on the fracture morphology, bone quality, and stability requirements.
1.
Plate Osteosynthesis:
*
Plate Selection and Contouring:
*
1/3 Tubular Plates:
Versatile for simple fibular fractures. They must be meticulously contoured to the complex anterior bow and posterior twist of the fibula.
*
Pre-contoured Locking Plates:
Increasingly popular, especially for comminuted fractures, osteoporotic bone, or higher Weber C fractures. They offer angular stability, reducing the risk of screw pull-out. They still require accurate contouring to prevent plate prominence.
*
Anti-glide Plates:
For long oblique fractures (e.g., Weber B), a posterolateral plate position acts as an anti-glide construct, resisting superior and posterior migration of the distal fragment.
*
Hook Plates:
May be used for avulsion fractures of the lateral malleolus tip or for severely comminuted distal fragments, providing distal purchase.
*
Plate Application:
*
Lag Screws:
For oblique fractures, a lag screw placed across the fracture site (either through a plate hole or as an independent screw prior to plate application) provides primary interfragmentary compression.
*
Plate Fixation:
Secure the plate proximally and distally with cortical or locking screws. For cortical screws, bicortical purchase is generally preferred. For locking screws, ensure proper alignment with the plate holes.
*
Screw Sequence:
Typically, apply a lag screw first, then secure the plate to one main fragment, reduce the other fragment to the plate, and secure it.
*

-
Syndesmotic Assessment and Fixation:
- Intraoperative Stress Test: After definitive fibular fixation, reassess syndesmotic stability. Common tests include the external rotation stress test and the hook test (grasping the fibula with a bone clamp and attempting to translate it laterally and anteriorly relative to the tibia). Fluoroscopic visualization is essential to confirm stability. Medial clear space widening (>2mm compared to superior clear space) or widening of the tibiofibular clear space suggests instability requiring fixation.
-
Syndesmotic Screw Placement (Static Fixation):
- Typically, one or two cortical screws (e.g., 3.5mm or 4.5mm) are inserted from the fibula, across the interosseous membrane, into the tibia.
- Placement is usually 2-4 cm proximal to the ankle joint line, aiming approximately 30 degrees posteromedially and 15 degrees superiorly to ensure good purchase in the tibia.
- Traditionally, the foot is dorsiflexed to neutral (0 degrees) during screw insertion to optimize talar position and prevent overcompression, which can lead to limited dorsiflexion and premature screw breakage. Engaging three cortices (tricortical fixation) is generally considered sufficient and often preferred over four cortices to reduce the risk of overcompression.
-
Suture Button Devices (Dynamic Fixation):
- These devices (e.g., TightRope™) provide dynamic stabilization, allowing physiologic motion at the syndesmosis. They consist of cortical buttons connected by a high-strength suture.
- A guidewire and cannulated drill are used to create a tunnel through the fibula and tibia (typically tricortical). The device is then passed through, and the buttons are secured on the medial tibial and lateral fibular cortices, tensioning the syndesmosis.
- Advantages include a lower rate of hardware removal compared to syndesmotic screws.
-

Closure
- Irrigation and Hemostasis: Copiously irrigate the wound with sterile saline. Achieve meticulous hemostasis to prevent hematoma formation, which can compromise wound healing.
- Periosteal/Fascial Repair: If possible, approximate the incised periosteum or deep fascia over the fibula using absorbable sutures to cover the hardware and restore anatomical planes. Avoid excessive tension.
- Subcutaneous Closure: Close the subcutaneous tissue layer using interrupted absorbable sutures to eliminate dead space and reduce tension on the skin closure.
- Skin Closure: Close the skin with non-absorbable sutures or staples.
- Dressing and Immobilization: Apply a sterile, non-adherent dressing. A well-padded posterior splint or short leg cast is applied to maintain the ankle in a neutral position and protect the fixation.
Complications & Management
Despite meticulous surgical technique, complications can arise following operative fixation of lateral malleolus fractures. Comprehensive understanding and proactive management are paramount.
Common Complications and Management Strategies
| Complication | Incidence (%)
| Salvage / Management Strategies
Approximate range for common types. Exact figures vary by specific population and definitions. |
|
Healing Complications
|
Incidence:
5-15% (higher in certain patient populations) |
Prevention:
Meticulous surgical technique, gentle soft tissue handling, timely surgery (after swelling subsides), strict aseptic technique, prophylactic antibiotics.
Management:
Superficial Infection:
Oral antibiotics, wound care.
Deep Infection:
Surgical debridement, IV antibiotics, hardware removal (if fixation is healed), or staged reconstruction.
Wound Dehiscence/Necrosis:
Debridement, local wound care, vacuum-assisted closure (VAC), skin grafting or flap coverage for extensive defects. |
|
Nonunion / Malunion
|
Incidence:
<5% for lateral malleolus (higher for comminuted/open fractures or poor patient compliance) |
Prevention:
Anatomical reduction, stable fixation, appropriate rehabilitation, addressing underlying patient factors (smoking, nutrition).
Management:
Nonunion:
Revision ORIF with bone grafting (autograft/allograft), structural augmentation (e.g., plating with bone substitute).
Malunion (symptomatic):
Corrective osteotomy to restore fibular length/rotation, addressing syndesmotic and talar alignment. Asymptomatic malunion may be observed. Post-traumatic arthritis may necessitate arthrodesis. |
|
Hardware Irritation / Failure
|
Incidence:
10-30% (related to plate prominence, screw length, syndesmotic screws) |
Prevention:
Correct plate contouring, appropriate screw length, flush hardware placement, careful assessment of syndesmotic screw tension.
Management:
Symptomatic Hardware:
Elective hardware removal after fracture union (typically 6-12 months post-op). Syndesmotic screws are often removed between 6-12 weeks, though some literature supports retention.
Hardware Failure (nonunion):
Revision surgery, often with stronger implants, bone grafting, and potentially different fixation construct. |
|
Nerve Injury
|
Incidence:
1-5% (Superficial Peroneal Nerve, Sural Nerve) |
Prevention:
Meticulous soft tissue dissection, identification and careful retraction of nerves, limiting excessive traction.
Management:
Neuropraxia:
Observation, typically resolves within weeks to months. Physical therapy to prevent contractures.
Neurotmesis/Axonotmesis (severe injury):
Referral to peripheral nerve specialist, neurolysis, or nerve repair/grafting if indicated. Persistent painful neuroma may require excision. |
|
Post-Traumatic Arthritis
|
Incidence:
10-20% (long-term, especially with articular incongruity or sustained malreduction) |
Prevention:
Anatomical reduction of articular surface, stable fixation, proper rehabilitation.
Management:
Mild/Moderate:
Conservative management (NSAIDs, activity modification, bracing, injections, physical therapy).
Severe:
Ankle arthrodesis (fusion) or total ankle arthroplasty (replacement) in selected cases. |
|
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE)
|
Incidence:
DVT 10-20% (clinical); PE <1% (symptomatic) |
Prevention:
Pre-operative risk assessment, chemical prophylaxis (LMWH, Factor Xa inhibitors) and/or mechanical prophylaxis (compression stockings, intermittent pneumatic compression devices) as per institutional guidelines.
Management:
Anticoagulation as per guidelines for DVT/PE. |
|
Complex Regional Pain Syndrome (CRPS) / Reflex Sympathetic Dystrophy
|
Incidence:
1-5% |
Prevention:
Minimizing surgical trauma, early pain management, early mobilization.
Management:
Multimodal approach: physical therapy, pain management (neuropathic pain medications, nerve blocks), psychological support. Early diagnosis is key. |
|
Loss of Syndesmotic Reduction / Malreduction
|
Incidence:
5-10% (can lead to malunion and arthritis) |
Prevention:
Accurate intraoperative assessment with stress testing and fluoroscopy, proper screw/suture button placement, avoidance of overtightening, dynamic versus static fixation choice.
Management:
Revision surgery to restore syndesmotic reduction and stabilize if symptomatic or leading to arthritis. Early intervention is preferred. |
* Incidence rates are approximate and can vary significantly based on patient population, fracture complexity, surgical technique, and study methodology.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring function and minimizing long-term disability following lateral malleolus fracture fixation. Protocols are typically individualized based on fracture stability, quality of fixation, patient comorbidities, and surgeon preference. The general progression is as follows:
Phase 1: Acute Protection (Weeks 0-2)
- Goal: Protect fixation, control pain and swelling, promote wound healing.
-
Immobilization:
- Initially, a well-padded posterior splint or short leg cast (non-weight bearing (NWB)).
- Once swelling subsides and sutures are removed (typically 10-14 days), transition to a removable walking boot (CAM boot) or a short leg cast.
- Weight-Bearing: Strictly Non-Weight Bearing (NWB) on the operative limb, using crutches or a walker.
-
Pain & Swelling Management:
- Elevation of the limb above heart level.
- Ice application (indirectly over the cast/dressing).
- Prescribed analgesics.
-
Early Motion:
- Active range of motion (ROM) for toes (flexion/extension) to promote circulation and prevent stiffness.
- Gentle, pain-free hip and knee ROM exercises.
- Wound Care: Daily wound inspection if not casted, keeping the incision clean and dry. Suture/staple removal at 10-14 days.
Phase 2: Early Mobilization & Protected Weight-Bearing (Weeks 2-6)
- Goal: Initiate gentle ankle motion, gradually introduce protected weight-bearing.
-
Weight-Bearing:
- Progress from NWB to Toe-Touch Weight-Bearing (TTWB) or Partial Weight-Bearing (PWB) in a CAM boot, as tolerated and dictated by fracture healing and stability.
- Gradually increase weight-bearing to 25-50% body weight.
-
Ankle ROM:
- Initiate gentle active and passive ankle ROM exercises (dorsiflexion, plantarflexion, inversion, eversion) out of the boot, within pain-free limits. Avoid excessive stress on the fracture site.
- Non-resistive ankle circles.
-
Strengthening:
- Isometric exercises for ankle musculature (e.g., gentle dorsiflexion/plantarflexion pushes against a wall).
- Start light resistance band exercises for ankle ROM (if appropriate for fracture stability).
- Proprioception: Begin gentle balance exercises while seated or using bilateral support.
Phase 3: Progressive Strengthening & Full Weight-Bearing (Weeks 6-12)
- Goal: Progress to full weight-bearing, restore full ankle ROM, improve strength and proprioception.
- Weight-Bearing: Gradually wean from the CAM boot to supportive shoes. Progress to full weight-bearing (FWB) as pain allows and radiographic healing progresses.
- Ankle ROM: Continue to work on achieving full, pain-free ankle ROM. Manual therapy techniques by a physical therapist may be beneficial.
-
Strengthening:
- Progressive resistive exercises for all ankle muscle groups (e.g., resistance bands, calf raises, toe raises, heel walks).
- Initiate eccentric loading exercises.
- Proprioception & Balance: Single-leg standing balance, wobble board exercises, uneven surface walking.
- Gait Training: Focus on normal gait mechanics without a limp.
Phase 4: Advanced Activity & Return to Sport (Weeks 12+)
- Goal: Achieve maximum functional recovery, return to recreational or sport-specific activities.
- Strengthening: Advanced strengthening, including plyometrics and power exercises.
- Sport-Specific Training: Gradually introduce agility drills, jumping, cutting, and sport-specific movements.
- Endurance: Progressive cardiovascular conditioning.
- Hardware Removal: If a syndesmotic screw was placed, it is often considered for removal between 6-12 weeks post-op, especially if symptomatic. Other hardware is typically left in situ unless symptomatic (usually >6-12 months post-union).
- Criteria for Return to Sport: Full pain-free ROM, symmetrical strength (>90% compared to contralateral limb), good balance and proprioception, and no gait abnormalities.
Note: Rehabilitation protocols are guidelines and should always be adapted based on individual patient progress, radiographic healing, and clinical assessment by the treating surgeon and physical therapist.
Summary of Key Literature / Guidelines
The management of lateral malleolus fractures has evolved considerably, guided by biomechanical research and clinical outcomes. Key tenets include:
- Anatomical Reduction: The overriding principle remains the anatomical reduction of the fibula, restoring its length, rotation, and alignment. Malreduction, even by a few millimeters, significantly increases joint contact pressures and the risk of post-traumatic arthritis. This is particularly emphasized in the classic works of Lauge-Hansen and Weber classifications, which describe injury patterns and guide treatment.
- Syndesmotic Stability: A major focus of contemporary literature is the accurate assessment and appropriate management of syndesmotic injuries. Intraoperative stress testing (e.g., external rotation stress test, hook test) with fluoroscopic guidance is crucial to identify subtle instability. The use of syndesmotic screws versus suture button devices (e.g., TightRope™) remains an area of ongoing research, with suture buttons gaining favor due to dynamic stabilization and potentially lower rates of hardware removal. However, precise placement and appropriate tensioning are critical for both methods.
- Plate Choice: Locking plates have become a standard option, especially for comminuted fractures, osteoporotic bone, or higher fibular fractures (Weber C), providing angular stability where conventional cortical screw fixation might be insufficient. The choice between lateral, posterolateral (anti-glide), or even anterior plating depends on fracture morphology and biomechanical considerations.
- Hardware Removal: While traditionally syndesmotic screws were routinely removed, particularly if tricortical, current evidence suggests that routine removal may not be necessary for all patients, especially with dynamic fixation devices. Symptomatic hardware or a clear indication of compromised ankle motion due to hardware impingement remain primary reasons for removal.
- Post-operative Weight-Bearing: Protocols have become increasingly aggressive, with early protected weight-bearing being initiated as early as 2 weeks post-op for stable fixation constructs, in contrast to historical prolonged non-weight bearing. This promotes early functional recovery without compromising fracture healing if the fixation is stable.
- Evidence-Based Guidelines: Organizations like the American Academy of Orthopaedic Surgeons (AAOS) provide clinical practice guidelines for the management of ankle fractures, synthesizing current evidence to aid decision-making. These guidelines often highlight the importance of careful soft tissue management, appropriate timing of surgery, and individualized rehabilitation protocols to optimize patient outcomes. The literature consistently emphasizes that successful outcomes hinge on restoring the anatomical integrity of the ankle mortise.
Clinical & Radiographic Imaging
You Might Also Like