Mastering Hindpart of the Foot Surgery: Essential Joint Anatomy
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Mastering Hindpart of the Foot Surgery: Essential Joint Anatomy. The hindpart of the foot features three primary surgical joints: the posterior subtalar, talocalcaneonavicular, and calcaneocuboid. Surgical access involves understanding landmarks like the tarsal canal and sinus tarsi. Dr. Mohammad Hutaif's guide further details the anatomy of these joints and comprehensive treatment strategies for osteomyelitis in children.
Introduction & Epidemiology
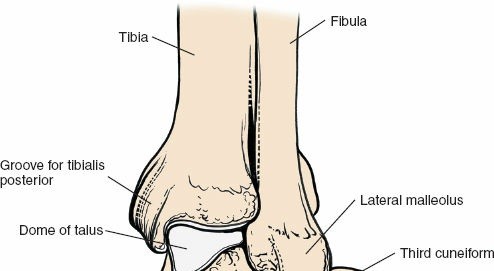
The hindfoot, comprising the talus and calcaneus, represents a critical anatomical and biomechanical unit integral to lower extremity function. Its complex articulation with the leg and midfoot facilitates adaptable ambulation over varied terrains, acting as a critical shock absorber and lever arm. Surgical intervention in this region is frequently indicated for a spectrum of pathologies including traumatic injuries (fractures, dislocations), degenerative conditions (arthritis), inflammatory processes (osteomyelitis, synovitis), congenital deformities, and acquired deformities (e.g., adult acquired flatfoot deformity). Mastery of hindfoot surgery hinges upon an exhaustive understanding of its intricate joint anatomy, ligamentous stabilizers, and neurovascular relationships.
Epidemiologically, hindfoot pathologies present a significant burden. Calcaneal fractures, predominantly intra-articular, represent approximately 60% of all tarsal bone fractures and 2% of all fractures, often resulting from high-energy axial loading. Talus fractures, while less common (around 0.3% of all fractures), carry a high risk of avascular necrosis and post-traumatic arthritis due to the precarious blood supply and extensive articular cartilage. Subtalar arthritis, whether post-traumatic, inflammatory, or idiopathic, is a common debilitating condition requiring fusion. Pediatric hindfoot conditions, such as congenital clubfoot, tarsal coalitions, or osteomyelitis, demand tailored approaches recognizing the developing osseous structures and growth plates. Surgical precision, informed by a detailed anatomical knowledge, is paramount to optimize outcomes and minimize complications in this complex region.
Surgical Anatomy & Biomechanics
The hindfoot articulates via three primary joints: the talocalcaneal (subtalar), talonavicular, and calcaneocuboid joints. Together, the talonavicular and calcaneocuboid joints form the transverse tarsal (Chopart's) joint. The subtalar joint is unique in its capacity to invert and evert the foot, while the Chopart's joint contributes significantly to the midfoot's flexibility and adaptability.
Talocalcaneal (Subtalar) Joint
The subtalar joint is functionally comprised of three distinct facets: anterior, middle, and posterior.
*
Posterior Facet:
This is the largest and most consistently identifiable facet. The inferior surface of the talus presents a large, convex posterior facet that articulates with a reciprocally concave posterior facet on the superior aspect of the calcaneus. The joint line for the posterior facet is often oblique, visible from a lateral surgical approach.
*
Middle Facet:
The talus bears a medial, slightly convex middle facet that articulates with the sustentaculum tali of the calcaneus.
*
Anterior Facet:
The talus has an anterior facet that articulates with a corresponding facet on the calcaneus, anterior to the sustentaculum tali.
*
Joint Capsule and Ligaments:
The subtalar joint is encapsulated and reinforced by several strong ligaments.
*
Interosseous Talocalcaneal Ligament (ITCL):
This robust, bilaminar ligament is situated within the tarsal canal, serving as the primary stabilizer of the subtalar joint. It effectively separates the posterior subtalar articulation from the anterior and middle facets, functionally linking the talus and calcaneus.
*
Cervical Ligament (Ligamentum Cervicis Tali):
A tough, extra-articular ligament located in the sinus tarsi, anterior and lateral to the ITCL. It provides significant stability and must often be divided or released during lateral approaches to the subtalar joint.
*
Lateral, Medial, Posterior, and Anterior Talocalcaneal Ligaments:
These are capsular thickenings providing further support.
The primary movements at the subtalar joint are pronation (eversion, abduction, dorsiflexion) and supination (inversion, adduction, plantarflexion) of the foot relative to the leg. These motions are crucial for shock absorption and adaptation to uneven ground.
Tarsal Canal and Sinus Tarsi
The
tarsal canal
is a critical anatomical landmark for surgical access and understanding hindfoot biomechanics. It runs obliquely through the foot, deep between the talus and calcaneus.
*
Formation:
It is formed by a deep groove on the inferior surface of the talus (sulcus tali) and a corresponding groove on the superior surface of the calcaneus (sulcus calcanei).
*
Contents:
The tarsal canal houses the robust interosseous talocalcaneal ligament, the medial root of the inferior extensor retinaculum, and vascular structures.
*
Significance:
It serves as a dividing line, functionally separating the posterior subtalar joint from the talocalcaneonavicular (TCN) joint complex, which includes the anterior and middle subtalar facets. The canal's obliquity is critical for understanding the coupled motions of the subtalar joint.

Laterally, the tarsal canal widens considerably into the
sinus tarsi
.
*
Contents:
The sinus tarsi is filled with adipose tissue (a large fat pad), the cervical ligament, and the inferior extensor retinaculum.
*
Surgical Relevance:
For direct access to the anterior and middle facets of the subtalar joint, or for comprehensive debridement (e.g., in osteomyelitis or arthroscopic synovectomy), the fat pad must be mobilized and the cervical ligament often divided. The extensor digitorum brevis muscle (EDB) originates from the anterior wall of the sinus tarsi; its detachment may be necessary for broader access, particularly towards the calcaneocuboid joint or for comprehensive exposure during calcaneal fracture fixation.


Talonavicular Joint
The talonavicular joint is the medial component of the transverse tarsal joint.
*
Articular Surfaces:
The head of the talus, which is convex and ovoid, articulates with the concave posterior surface of the navicular bone.
*
Ligaments:
It is supported by the dorsal talonavicular ligament superiorly and the crucial plantar calcaneonavicular (spring) ligament inferiorly. The spring ligament forms a critical sling supporting the talar head, essential for maintaining the medial longitudinal arch. Dysfunction of this ligament contributes significantly to adult acquired flatfoot deformity.
*
Biomechanics:
This joint permits gliding and rotation, contributing to the pronation-supination movements of the hindfoot and midfoot.
Calcaneocuboid Joint
The calcaneocuboid joint forms the lateral component of the transverse tarsal joint.
*
Articular Surfaces:
The anterior surface of the calcaneus, typically saddle-shaped (concavoconvex), articulates with the posterior surface of the cuboid, which is reciprocally shaped.
*
Ligaments:
This joint is heavily reinforced by strong ligaments:
*
Dorsal Calcaneocuboid Ligament:
Dorsal support.
*
Bifurcate Ligament:
Originating from the calcaneus, it divides into calcaneonavicular and calcaneocuboid components, stabilizing both the calcaneocuboid and talonavicular joints indirectly.
*
Long Plantar Ligament:
A very strong ligament running from the plantar aspect of the calcaneus to the cuboid and bases of the metatarsals, forming a tunnel for the peroneus longus tendon.
*
Short Plantar Ligament (Plantar Calcaneocuboid Ligament):
Located deep to the long plantar ligament, providing additional plantar support.
*
Biomechanics:
Often considered relatively rigid compared to the talonavicular joint, it still allows subtle gliding and rotation, playing a role in the "unlocking" and "locking" mechanism of the transverse tarsal joint during gait. Surgical access may require detachment of the extensor digitorum brevis.
Neurovascular Structures
Precise identification and protection of neurovascular structures are paramount.
*
Medial Side:
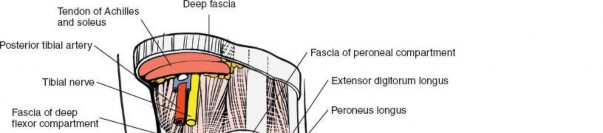
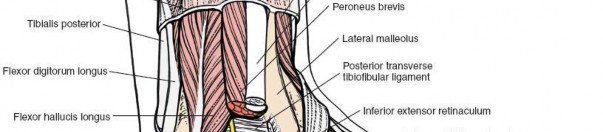
The posterior tibial artery, posterior tibial nerve, and tibialis posterior tendon traverse the tarsal tunnel posterior to the medial malleolus. The saphenous nerve and great saphenous vein are more superficial.
*
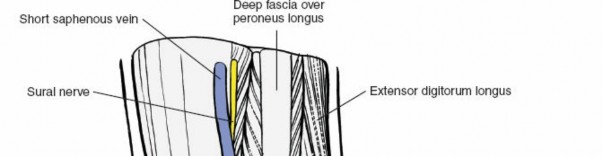
Lateral Side:
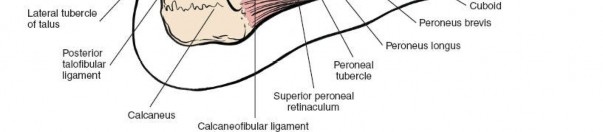
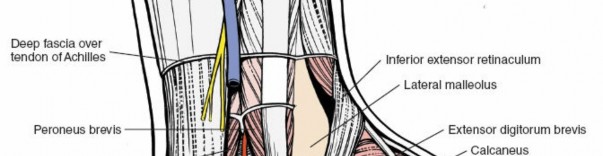
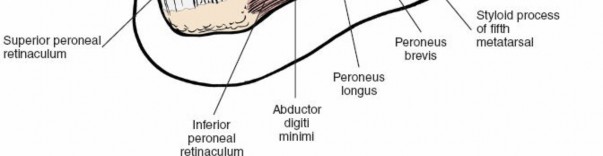
The sural nerve crosses posterior to the lateral malleolus and continues distally along the lateral foot. The superficial peroneal nerve typically passes anterior to the lateral malleolus, dividing into intermediate and medial dorsal cutaneous nerves. The peroneal tendons (longus and brevis) lie posterior to the lateral malleolus within their sheath.
*
Dorsal Side:
The dorsalis pedis artery and deep peroneal nerve run distally from the ankle joint, deep to the extensor retinaculum.
*
Plantar Side:
The plantar nerves and arteries (medial and lateral plantar) are terminal branches of the posterior tibial neurovascular bundle.
Indications & Contraindications
Indications for hindfoot surgery are diverse, encompassing traumatic, degenerative, inflammatory, and congenital etiologies. Contraindications typically revolve around patient comorbidities, local soft tissue status, or specific pathological considerations.
Indications
-
Traumatic Injuries:
- Displaced intra-articular calcaneal fractures (e.g., Sanders Type II, III, IV).
- Displaced talar neck/body fractures.
- Subtalar dislocations (irreducible or unstable).
- Chopart's joint fracture-dislocations.
- Traumatic arthritis of hindfoot joints refractory to conservative care.
-
Degenerative Conditions:
- Subtalar arthritis (post-traumatic, primary, inflammatory) leading to intractable pain and functional limitation.
- Talonavicular arthritis.
- Calcaneocuboid arthritis.
- Deformity correction secondary to arthritis (e.g., valgus or varus hindfoot malalignment).
-
Deformity Correction:
- Adult acquired flatfoot deformity (Stage IIb or III), requiring subtalar fusion, triple arthrodesis, or isolated talonavicular fusion in conjunction with soft tissue procedures.
- High-arched (cavovarus) foot deformities.
- Tarsal coalitions (resection or fusion).
- Residual clubfoot deformities requiring hindfoot osteotomies or fusions.
-
Infection:
- Osteomyelitis of the talus or calcaneus, especially in children, requiring debridement and antibiotic delivery.
- Septic arthritis of hindfoot joints unresponsive to aspiration and systemic antibiotics.
-
Tumors:
- Resection of benign or malignant tumors affecting the hindfoot bones.
Contraindications
-
Absolute Contraindications:
- Active local infection (unless the surgery is specifically for infection debridement and control).
- Severe vascular compromise precluding wound healing.
- Uncontrolled systemic comorbidities (e.g., severe diabetes, renal failure, cardiac disease) posing unacceptable anesthetic or surgical risks.
- Compromised skin envelope (e.g., severe blistering, non-viable skin, open wounds in the surgical field).
-
Relative Contraindications:
- Neuropathic arthropathy (Charcot foot) in an acute, unstable phase; definitive surgical reconstruction is often delayed until the quiescent phase.
- Severe osteopenia/osteoporosis compromising stable internal fixation.
- Patient non-compliance with post-operative protocols.
- Smoking (significantly increases complication rates, particularly nonunion and wound healing issues); strongly advised cessation pre-operatively.
- Significant edema or inflammation in the surgical area; often addressed with elevation and non-operative measures prior to surgery.
Table 1: Operative vs. Non-Operative Indications for Hindfoot Pathologies
| Pathology Type | Operative Indications | Non-Operative Indications |
|---|---|---|
| Traumatic Injuries | Displaced/unstable fractures (calcaneus, talus), irreducible dislocations, open fractures | Nondisplaced/stable fractures, minor sprains/ligamentous injuries, closed reductions with stable fixation |
| Degenerative Arthritis | Intractable pain/disability refractory to conservative care, significant deformity affecting function | Mild to moderate pain controlled by NSAIDs, orthotics, activity modification, injections |
| Deformity Correction | Progressive deformity (e.g., flatfoot, cavovarus) causing pain/dysfunction, failed orthotic management | Mild asymptomatic deformities, early-stage deformities responsive to orthotics/PT |
| Infection | Confirmed osteomyelitis (acute/chronic) requiring debridement, septic arthritis unresponsive to aspiration | Early-stage cellulitis without bone/joint involvement, controlled infection with systemic antibiotics only |
| Tumors | Symptomatic tumors, progressive lesions, suspected malignancy | Asymptomatic benign lesions, observational management |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is the cornerstone of successful hindfoot surgery. It minimizes surprises, optimizes efficiency, and enhances patient safety.
Pre-Operative Planning
- Clinical Assessment: Detailed history, physical examination assessing skin integrity, neurovascular status, range of motion, and stability. Documentation of pre-existing deformities or neurological deficits.
-
Imaging:
- Radiographs: Weight-bearing anteroposterior, lateral, and oblique views of the foot and ankle are standard. Specific views like Broden's (subtalar joint), Harris heel views (calcaneal body), or Canale views (talar neck) are crucial for specific fractures.
- Computed Tomography (CT): Essential for intra-articular fractures (calcaneus, talus) to define fracture morphology, fragment displacement, articular involvement, and guide surgical approach. Also valuable for tarsal coalitions and complex arthritic conditions.
- Magnetic Resonance Imaging (MRI): Indicated for soft tissue injuries (ligamentous, tendinous), avascular necrosis, osteomyelitis, and tumor evaluation.
- Bone Scintigraphy: May be useful for detecting early osteomyelitis or occult fractures.
- Templating: Utilize high-quality imaging (CT scans with 3D reconstructions) to pre-operatively plan osteotomies, guide implant selection (plates, screws, staples), and determine graft requirements. Consideration of hindfoot alignment (varus/valgus) is crucial for fusions and osteotomies.
- Surgical Approach Selection: Based on pathology location, fracture pattern, and desired exposure, determine the optimal incision(s) and potential need for extensile approaches.
- Equipment and Instruments: Ensure availability of necessary implants (e.g., cannulated screws, fusion plates, locking plates, external fixators), specialized instruments (e.g., distractors, osteotomes, burrs), and arthroscopic equipment if indicated.
- Antibiotic Prophylaxis: Administer appropriate intravenous antibiotics pre-incision.
- Deep Vein Thrombosis (DVT) Prophylaxis: Implement according to institutional protocols and patient risk factors.
Patient Positioning
Patient positioning depends on the specific surgical approach.
-
Lateral Approaches (e.g., for calcaneal fractures, subtalar fusion):
- Lateral Decubitus: Patient positioned on the unaffected side. Ipsilateral hip flexed, contralateral hip extended. Pelvis and torso secured with bolsters. The operative limb is draped free. This allows excellent access to the lateral hindfoot, subtalar joint, and calcaneocuboid joint. Fluoroscopy can be positioned for easy access.
- Supine with Ipsilateral Hip Bump: Patient supine with a roll under the ipsilateral hip to internally rotate the limb. This allows some lateral access but is less ideal for extensive exposure than full lateral decubitus.
-
Medial Approaches (e.g., for talonavicular fusion, medial calcaneal osteotomy, tarsal tunnel release, medial subtalar debridement):
- Supine: Patient supine. The operative leg can be externally rotated and the knee flexed, or positioned neutrally. This provides excellent access to the medial hindfoot structures.
-
Posterior Approaches (e.g., for posterior subtalar arthrodesis, Achilles tendon procedures):
- Prone: Patient prone with bolsters under the shins and pelvis. This offers optimal access to the posterior calcaneus and talus.
- Supine with a Bending Table: Less common but possible for limited posterior access.
- Arthroscopy: Patient supine or lateral decubitus, depending on the portals used and joints addressed. A non-invasive distractor may be employed.
For all approaches, meticulous padding of pressure points, appropriate tourniquet application, and careful preparation and draping are essential. The entire limb should be prepped and draped to allow for full range of motion of the foot and ankle, if required during the procedure.

Detailed Surgical Approach / Technique
Given the breadth of hindfoot surgery, we will detail a representative approach: the lateral extensile approach to the hindfoot , commonly used for intra-articular calcaneal fractures or subtalar arthrodesis, which directly interacts with the key anatomical structures discussed. This approach allows comprehensive visualization and manipulation of the sinus tarsi, subtalar joint, and calcaneocuboid joint.
Lateral Extensile Approach for Hindfoot Surgery (e.g., Calcaneal Fracture Fixation or Subtalar Fusion)
-
Incision:
- Position the patient in lateral decubitus. A curvilinear L-shaped or extended L-shaped incision is made.
- Start approximately 2 cm posterior and 2 cm superior to the tip of the lateral malleolus.
- Extend distally parallel to the lateral border of the Achilles tendon, curving anteriorly just above the calcaneal tuberosity.
- Continue anteriorly, remaining posterior to the peroneal tendons, and then gently curving inferiorly towards the calcaneocuboid joint, ending about 1 cm proximal to the joint line.
-
The incision creates an osteocutaneous flap containing the sural nerve and peroneal tendons. Care must be taken to minimize retraction on the flap, particularly at its apex.
-
Superficial Dissection and Flap Elevation:
- Deepen the incision through the subcutaneous tissue to the level of the deep fascia, preserving the sural nerve. The sural nerve typically courses inferior to the incision at the heel pad and then superiorly along the flap.
- Identify and protect the sural nerve and its branches, which are located superficial to the peroneal tendons.
- Elevate the full-thickness osteocutaneous flap (containing skin, subcutaneous tissue, and the peroneal retinaculum with peroneal tendons) from the lateral wall of the calcaneus and the sinus tarsi. This is a critical step to achieve broad exposure and minimize flap necrosis.
-
The anterior limb of the incision is deepened carefully to avoid injury to the intermediate dorsal cutaneous nerve (a branch of the superficial peroneal nerve) and the lateral plantar artery branches.


-
Exposure of Sinus Tarsi and Subtalar Joint:
- Once the flap is elevated, the underlying sinus tarsi is exposed. The sinus is filled with adipose tissue and the robust ligamentum cervicis tali.
- Mobilize or excise the fat pad from the sinus tarsi.
- Divide the ligamentum cervicis tali. This provides access to the floor of the sinus and the interosseous talocalcaneal ligament, which defines the superior boundary of the tarsal canal.
-
The extensor digitorum brevis (EDB) muscle originates from the anterior part of the sinus tarsi. For broader exposure of the calcaneocuboid joint or anterior calcaneus, the EDB may need to be carefully detached from its origin and reflected anteriorly. Preserve its neurovascular supply if possible.
-
Articular Visualization and Pathology Management:
- Subtalar Joint: With the sinus tarsi cleared, the anterior, middle, and posterior facets of the subtalar joint become accessible. The posterior facet is often visualized directly, and the anterior/middle facets are accessible through the sinus tarsi.
- Calcaneal Fractures: For calcaneal fractures, this approach allows direct visualization and reduction of articular fragments, particularly the posterior facet. A laminar spreader or custom distractor can be used in the sinus tarsi to restore calcaneal height and width, and to de-impact the posterior facet.
- Subtalar Fusion: For subtalar arthrodesis, the articular cartilage of the subtalar joint (all three facets) is debrided down to bleeding subchondral bone. This can be achieved with osteotomes, burrs, or curettes. Bone graft (autograft or allograft) is typically packed into the prepared joint space to promote fusion.
- Osteomyelitis: In cases of osteomyelitis (e.g., in children), this approach facilitates meticulous debridement of infected bone and soft tissue from the talus or calcaneus. Culture-guided antibiotic beads can be implanted, or a formal sequestrectomy performed. The goal is complete removal of necrotic and infected tissue while preserving viable bone and joint integrity as much as possible, particularly in pediatric patients to avoid growth plate damage.
-
Calcaneocuboid Joint:
If calcaneocuboid pathology (e.g., fracture or arthritis) is present, the EDB reflection allows direct access. Articular preparation for fusion involves cartilage removal and bone graft placement.

-
Reduction and Fixation (for Fractures/Fusions):
- Fractures: Using fluoroscopy and direct visualization, reduce the fracture fragments. Temporary K-wire fixation can be employed. Definitive fixation typically involves a low-profile plate contoured to the lateral wall of the calcaneus, combined with strategically placed screws (e.g., lag screws across the posterior facet, screws engaging the sustentaculum tali).
-
Fusions:
Once the joint is prepared and graft placed, compression is applied across the fusion site. This can be achieved with large-fragment cannulated screws (e.g., 6.5 mm or 7.3 mm) placed from the calcaneus into the talus, or vice versa, often two screws for rotational stability. Plate fixation across the fusion site may also be used, particularly for severe deformities or revision surgeries. Ensure adequate alignment (neutral to slight valgus) is achieved.
-
Closure:
- Meticulous hemostasis is achieved.
- Irrigate the wound thoroughly.
- Close the deep fascia (peroneal retinaculum and EDB origin) if detached.
- Redrape the osteocutaneous flap carefully, ensuring no tension at the skin edges.
- Close the subcutaneous layer and skin with absorbable sutures and non-absorbable sutures/staples, respectively. A drain may be considered if significant dead space or bleeding is anticipated.
- Apply a sterile dressing and a well-padded splint (e.g., posterior splint or sugar-tong) in a neutral position.
Complications & Management
Hindfoot surgery is associated with a range of potential complications, necessitating careful surgical technique, vigilant post-operative monitoring, and a well-defined management strategy.
Table 2: Common Complications of Hindfoot Surgery, Incidence, and Salvage Strategies
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Wound Healing Issues / Infection | 5-25% (higher in calcaneal fx, DM, smoking) | Aggressive debridement, negative pressure wound therapy, flap coverage, IV antibiotics, removal of hardware if infected. |
| Nonunion / Malunion (Fusion) | 5-20% (higher in smokers, poor bone quality) | Revision fusion with additional bone graft (autograft preferred), rigid internal fixation, possible external fixation, bone stimulator. For malunion: corrective osteotomy with fusion. |
| Avascular Necrosis (AVN) (Talus) | Up to 10-50% (depending on fracture type/displacement) | Core decompression, vascularized bone graft, subsequent fusion (subtalar/pantalar) if collapse and severe pain occur. |
| Post-Traumatic Arthritis | Up to 70-90% (calcaneal fx, talar fx) | Initial conservative management (NSAIDs, orthotics, injections). Definitive management: arthrodesis (subtalar, triple). |
| Nerve Injury (Sural, Peroneal) | 5-15% (traction, direct injury) | Conservative management initially (neuropathic pain meds), nerve blocks. Surgical exploration, neurolysis, or grafting for persistent deficits. |
| Hardware Irritation / Pain | 10-30% | Hardware removal after bone healing/fusion, typically 6-12 months post-op. |
| Complex Regional Pain Syndrome (CRPS) | 2-10% | Early diagnosis, multidisciplinary pain management (PT, OT, nerve blocks, medications, psychological support). |
| DVT / Pulmonary Embolism (PE) | 1-5% (DVT), <1% (PE) | Anticoagulation, early mobilization. Thrombectomy for severe PE. |
| Residual Deformity | Variable, depends on initial pathology | Corrective osteotomy, revision fusion, or soft tissue balancing procedures. |
Specific Considerations
- Wound Complications: The hindfoot, particularly the lateral calcaneal region, is susceptible to wound complications due to the thin soft tissue envelope, extensive dissection required for some approaches, and tenuous blood supply in certain patient populations (e.g., diabetics, smokers). Meticulous soft tissue handling, atraumatic retraction, and careful closure are crucial. Negative pressure wound therapy can be beneficial.
- Nonunion: Particularly in fusion procedures, nonunion is a significant concern. Risk factors include smoking, NSAID use, infection, inadequate immobilization, and poor bone graft incorporation. Strict adherence to weight-bearing restrictions and aggressive bone graft techniques are key.
- Avascular Necrosis of the Talus: The talus has a retrograde blood supply, making it vulnerable to AVN, especially after talar neck fractures. Early and accurate reduction, anatomical alignment, and stable fixation are paramount. The long-term sequelae often necessitate subsequent subtalar or pantalar arthrodesis.
- Infection Management: In pediatric osteomyelitis cases, surgical debridement must be thorough, removing all necrotic bone. Consideration of primary closure vs. open wound management with delayed closure, and local antibiotic delivery (e.g., calcium sulfate beads) is critical. Prolonged systemic antibiotic therapy based on culture sensitivities is essential.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a crucial determinant of long-term functional outcome, balancing protection of the surgical repair or fusion with early mobilization to prevent stiffness and muscle atrophy. Protocols are individualized based on the specific procedure, patient factors, and surgeon preference.
General Principles
- Protection: Initial phase focuses on protecting the surgical site, preventing weight-bearing, and controlling swelling.
- Immobilization: Appropriate splinting or casting is used to maintain reduction or fusion stability.
- Elevation & Edema Control: Critical in the early post-operative period to minimize swelling, reduce pain, and promote wound healing.
- Pain Management: Multimodal analgesia, including local nerve blocks, oral medications, and ice.
- Progressive Weight Bearing: Gradual increase in load as healing progresses.
- Range of Motion (ROM): Initiated based on stability of repair/fusion.
- Strengthening: Progressive strengthening exercises for intrinsic and extrinsic foot muscles, and lower leg muscles.
- Gait Training: Focus on restoring normal gait mechanics and proprioception.
Example Protocol: Subtalar Arthrodesis
This protocol is a general guideline; specific timelines may vary.
Phase I: Protection and Immobilization (Weeks 0-6)
- Goals: Protect fusion site, minimize pain and swelling, promote wound healing.
- Immobilization: Non-weight-bearing (NWB) in a well-padded posterior splint (Week 0-2), transitioning to NWB cast or CAM boot (Week 2-6).
- Activity: Strict NWB. Crutch or walker use. Ankle pump exercises (dorsiflexion/plantarflexion of ankle only) to promote circulation and prevent stiffness at ankle. Elevation of the limb above heart level.
- Pain/Edema Management: Ice, analgesics, compression.
- Suture Removal: 2-3 weeks post-op.
Phase II: Early Mobilization and Progressive Weight Bearing (Weeks 6-12)
- Goals: Gradually introduce weight-bearing, restore ankle/midfoot ROM (if not restricted by other fusions), maintain muscle strength.
- Immobilization: Continue CAM boot.
- Weight Bearing: Begin touch-down weight-bearing (TDWB) or partial weight-bearing (PWB) in CAM boot at Week 6-8, progressing to full weight-bearing (FWB) in CAM boot by Week 10-12, once radiographic signs of union are evident.
- Physical Therapy: Initiate gentle non-weight-bearing ankle ROM exercises. Progress to gentle resistance exercises for ankle and foot musculature. Initiate balance and proprioception exercises once FWB is achieved.
- Radiographic Assessment: Obtain serial radiographs to assess fusion progress. Clinical examination for tenderness and stability.
Phase III: Strengthening and Functional Integration (Weeks 12-24)
- Goals: Achieve full weight-bearing, restore functional strength and endurance, normalize gait.
- Immobilization: Transition from CAM boot to supportive shoe with orthotic inserts.
- Activity: Continue with progressive FWB. Gradually increase activity levels.
- Physical Therapy: Intensify strengthening exercises for the entire lower extremity. Focus on single-leg balance, gait training, stair climbing, and uneven surface ambulation.
- Return to Activity: Light impact activities (e.g., walking) can be considered at 4-5 months post-op. Gradual return to more demanding activities (running, sports) at 6-9 months, only after complete radiographic union and full strength recovery.
Phase IV: Advanced Activity and Return to Sport (Months 6-12+)
- Goals: Full return to desired activities, including sports.
- Activity: Continue with strength and conditioning. Sport-specific drills.
- Footwear: Continue use of supportive footwear and custom orthotics if beneficial.
- Long-term Monitoring: Regular follow-up for up to a year to monitor for residual symptoms or complications.
Rehabilitation for Other Procedures
- Calcaneal Fractures (ORIF): Similar principles to fusion, with NWB for 8-12 weeks depending on fracture stability and healing. Early ROM for ankle and subtalar joint (if appropriate for fracture pattern and stability of fixation) can be initiated if fixation is robust.
- Osteomyelitis Debridement: NWB and immobilization until infection is controlled and wound healing is adequate. Gradual weight-bearing then initiated, with close monitoring for recurrence or structural collapse.
- Soft Tissue Procedures (e.g., Spring Ligament Repair): Shorter NWB period (typically 4-6 weeks) followed by gradual weight-bearing in a boot, with emphasis on protecting the repaired soft tissues.
Summary of Key Literature / Guidelines
The management of hindfoot pathologies continues to evolve, guided by clinical research, randomized controlled trials, and expert consensus. Key literature and guidelines inform best practices for surgical intervention and post-operative care.
Calcaneal Fractures
- Indications for ORIF: The evidence generally supports open reduction and internal fixation (ORIF) for displaced intra-articular calcaneal fractures (Sanders Type II, III, IV) in appropriate candidates to restore articular congruity, calcaneal height, and width. Outcomes are generally superior to non-operative management for these specific fracture patterns in terms of anatomical restoration, though functional outcomes can be variable.
- Surgical Approach: The extended lateral approach (as detailed above) remains the most common and versatile for intra-articular fractures. Minimally invasive sinus tarsi approaches have shown promise for selected fracture patterns (e.g., tongue-type, some joint depression patterns) with potentially lower wound complication rates, but require specific surgeon expertise and specialized instrumentation.
- Timing of Surgery: Delayed surgery (7-14 days post-injury) once soft tissue swelling has subsided (wrinkle test positive) is generally recommended to minimize wound complications.
- Outcomes: While ORIF improves anatomical parameters, residual pain and post-traumatic subtalar arthritis are common, often necessitating subtalar arthrodesis in the long term. A meta-analysis by Dhillon et al. (2015) highlighted the high rate of subtalar arthritis regardless of operative or non-operative management for intra-articular fractures, but operative management generally led to better functional scores.
Subtalar Arthrodesis
- Gold Standard: Subtalar arthrodesis remains the gold standard for painful, debilitating subtalar arthritis refractory to conservative management, and for correcting rigid hindfoot deformities.
- Approaches: Lateral approaches are most common, often utilizing the sinus tarsi approach. Medial approaches are less common but may be indicated for specific deformities or when concomitant procedures require medial access. Arthroscopic subtalar arthrodesis is a less invasive option for appropriate cases (e.g., primary arthritis without significant deformity), demonstrating comparable fusion rates and potentially faster recovery.
- Fixation: Compression screw fixation (typically 1-3 cannulated screws) is the most common method. Plates may be used for additional stability, particularly in revision surgery or complex deformities.
- Outcomes: High fusion rates (85-95%) are reported, with significant pain relief and improved function. However, adjacent joint arthritis (ankle, midfoot) is a recognized long-term sequela due to altered biomechanics.
Adult Acquired Flatfoot Deformity (AAFD)
- Staging: The Johnson and Strom (modified by Myerson) classification system is widely used to guide treatment.
- Surgical Reconstruction: Surgical treatment varies based on stage. Stage II AAFD often involves complex soft tissue procedures (e.g., FDL transfer, spring ligament repair) combined with osseous procedures such as medializing calcaneal osteotomy and/or lateral column lengthening. Stage III (fixed deformity, subtalar arthritis) typically necessitates hindfoot arthrodesis (subtalar, triple, or double fusion).
- Evidence: Level I evidence comparing specific surgical techniques for AAFD is limited, but a consensus exists for staged reconstruction. Long-term studies emphasize the importance of achieving proper hindfoot alignment and stability.
Pediatric Hindfoot Osteomyelitis
- Diagnosis: Often challenging due to non-specific symptoms. MRI is the most sensitive imaging modality. Bone biopsy and culture are crucial for definitive diagnosis and guiding antibiotic therapy.
- Management: Management is typically a combination of surgical debridement and prolonged, culture-specific intravenous and oral antibiotics. Aggressive debridement of sequestra and infected tissue is paramount. Consideration must be given to preserving growth plates and articular cartilage in the developing foot.
- Outcome: Early diagnosis and comprehensive treatment typically lead to good outcomes, but potential for growth arrest, deformity, and chronic infection exists, particularly with delayed presentation or inadequate debridement.
In conclusion, the successful management of hindfoot pathologies necessitates a deep anatomical understanding, meticulous surgical technique, and individualized post-operative rehabilitation, all underpinned by a critical appraisal of current literature and evidence-based guidelines. Continual refinement of surgical strategies and rehabilitation protocols remains an ongoing pursuit in orthopedic foot and ankle surgery.
Clinical & Radiographic Imaging

You Might Also Like

