Navicular Fractures: Comprehensive Guide to Etiology, Anatomy, Biomechanics & Diagnosis

Key Takeaway
Navicular fractures are critical foot injuries, often caused by high-energy trauma or stress, threatening midfoot stability. Diagnosis relies on plain radiographs, revealing cortical disruptions or alignment changes, often supplemented by CT scans for detailed fracture morphology. Understanding the navicular's precarious blood supply and biomechanical role is crucial for managing AVN risk and preventing long-term morbidity.
Introduction & Epidemiology
Navicular fractures, while relatively uncommon, represent a critical subset of foot injuries due to the bone's pivotal role in midfoot stability, load transmission, and the maintenance of the medial longitudinal arch. Missed or inadequately treated navicular fractures carry a high risk of long-term morbidity, including post-traumatic arthritis, avascular necrosis (AVN), and chronic pain with functional impairment. These fractures typically result from high-energy trauma, often axial loading or crush injuries, but can also occur as stress fractures, particularly in athletic populations.
The navicular bone, often termed the "keystone" of the medial column, is positioned strategically between the talus and the cuneiforms. Its unique anatomical position and tenuous blood supply render it susceptible to complex fracture patterns and complications. Epidemiologically, navicular body fractures are rare, accounting for less than 1% of all foot fractures. Stress fractures of the navicular are more prevalent in athletes, particularly runners and jumpers, and can constitute up to 35% of all foot stress fractures in this cohort. Acute fractures commonly affect a younger, active population, often involving high-impact mechanisms. Careful radiographic assessment, frequently supplemented by advanced imaging, is paramount for accurate diagnosis and classification, which in turn dictates optimal management.
Surgical Anatomy & Biomechanics
The navicular is a boat-shaped tarsal bone articulating proximally with the head of the talus, distally with the three cuneiforms, and laterally with the cuboid. These articulations form the talonavicular, naviculocuneiform, and cuneonavicular joints, respectively. The medial aspect presents a prominent tuberosity, providing insertion for the tibialis posterior tendon and an attachment point for the spring ligament (plantar calcaneonavicular ligament). Dorsally, the navicular provides attachment for the bifurcate ligament and other dorsal midfoot ligaments.
Blood Supply: The blood supply to the navicular is precarious, contributing significantly to the risk of avascular necrosis (AVN) following fracture. Arterial supply is predominantly derived from branches of the dorsalis pedis artery dorsally and the medial plantar artery plantarly. These vessels form an anastomotic arcade that supplies the central portion of the bone. However, a relatively avascular watershed area often exists in the central one-third of the bone, making this region particularly vulnerable to ischemia after traumatic disruption of the vascular network. The vascularity is further compromised in comminuted or significantly displaced fractures.
Ligamentous and Tendinous Attachments:
*
Tibialis Posterior Tendon:
Inserts onto the navicular tuberosity, undersurface of the three cuneiforms, cuboid, and bases of the 2nd, 3rd, and 4th metatarsals. It is a primary stabilizer of the medial longitudinal arch.
*
Spring Ligament (Plantar Calcaneonavicular Ligament):
Crucial for dynamic support of the talar head and static support of the medial arch.
*
Deltoid Ligament:
Its deep fibers attach to the talonavicular joint capsule.
*
Talonavicular Joint Capsule:
Robust, reinforcing the proximal articulation.
Biomechanics: The navicular serves as a crucial mechanical link in the medial column of the foot, acting as a "keystone" in the medial longitudinal arch. It participates in complex triplanar motion, contributing to pronation and supination. Forces from the talus are transmitted through the navicular to the cuneiforms and metatarsals. Disruption of the navicular's integrity, whether through fracture or ligamentous injury, compromises the stability and load-bearing capacity of the entire medial column, potentially leading to acquired flatfoot deformity, altered gait mechanics, and debilitating pain. Axial loading with a dorsiflexed foot often generates compressive forces leading to body fractures, while powerful contractions of the tibialis posterior can result in avulsion fractures of the tuberosity.
Indications & Contraindications
Accurate diagnosis and classification of navicular fractures are paramount for determining appropriate management. Initial assessment begins with plain radiographs, often supplemented by advanced imaging.
Radiograph of the Foot: Uncover Navicular Fracture Clues
Plain radiographs are the initial diagnostic tool, requiring careful interpretation. Standard views include:
*
Anteroposterior (AP) View:
Assesses medial-lateral displacement and overall alignment. Look for cortical disruption, lucency, or altered joint spaces.
*
Lateral View:
Critical for evaluating dorsal-plantar displacement, sag in the medial column, and the integrity of the talonavicular articulation. The Meary's angle (angle between the long axis of the talus and the first metatarsal) is particularly important; divergence >15° suggests significant midfoot collapse. Calcaneal inclination and Talo-first metatarsal angle also provide clues.
*
Oblique View:
Can reveal subtle fractures not evident on AP or lateral views, particularly in the navicular body or tuberosity.
Subtle signs of navicular fracture on radiographs include:
* Cortical step-offs or disruptions.
* Focal lucency or sclerosis suggestive of a stress fracture (often poorly visualized acutely).
* Avulsion fragments, particularly from the medial tuberosity.
* Alteration of the cuneiform-navicular or talonavicular joint spaces.
* Sagittal plane malalignment or collapse of the medial column.
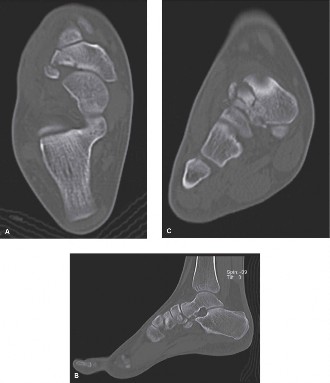
Figure 1: Plain radiograph illustrating potential signs of a navicular fracture, such as cortical irregularity or altered alignment.
Advanced Imaging:
*
Computed Tomography (CT) Scan:
Essential for detailed evaluation of fracture morphology, comminution, articular involvement, and displacement. It provides superior visualization of complex fracture patterns, helps delineate fragment size and location, and is crucial for pre-operative planning. Three-dimensional (3D) reconstructions are invaluable for understanding the spatial orientation of fragments and planning reduction strategies.
*
Magnetic Resonance Imaging (MRI):
Highly sensitive for stress fractures (showing marrow edema before cortical changes are visible on X-ray), occult fractures, and assessment of soft tissue injury. It can also evaluate for early signs of avascular necrosis.

Figure 2: Lateral radiograph demonstrating a navicular fracture with associated midfoot collapse and disruption of normal talo-first metatarsal alignment, indicative of significant injury.
Classification Systems:
*
Watson-Jones Classification (for Navicular Tuberosity Fractures):
* Type 1: Small avulsion fracture.
* Type 2: Larger fragment with involvement of the talonavicular articular surface.
* Type 3: Fracture extending into the navicular body.
*
Sangeorzan Classification (for Navicular Body Fractures):
The most widely accepted classification for acute body fractures, crucial for guiding treatment:
*
Type 1 (Coronal Shear):
Non-displaced or minimally displaced fracture in the coronal plane, often extending into the talonavicular and/or naviculocuneiform joints. Often stable.
*
Type 2 (Medial Dislocation/Compression):
Fracture involving the navicular body with significant medial displacement of the medial fragment, often with compression. Associated with medial column shortening.
*
Type 3 (Lateral Dislocation/Comminution):
Highly unstable, comminuted fracture of the navicular body with lateral dislocation and significant displacement of the lateral fragment. Often associated with significant midfoot disruption and soft tissue injury.
Figure 3: CT scan reconstruction displaying a comminuted navicular body fracture with articular involvement, highlighting the complexity requiring precise surgical planning.
Indications for Surgical Intervention:
Surgical management is generally favored for displaced navicular fractures, articular involvement, and instability.
-
Acute Navicular Body Fractures:
- Displacement ≥ 2mm (particularly Sangeorzan Type 2 and Type 3 fractures).
- Articular incongruity of the talonavicular or naviculocuneiform joints.
- Significant comminution leading to instability or loss of arch height.
- Open fractures.
- Failed non-operative management of initially non-displaced fractures.
-
Navicular Tuberosity Fractures:
- Large, significantly displaced fragments (Watson-Jones Type 2 and 3) causing instability or painful nonunion.
- Displaced avulsion fractures involving a significant portion of the tibialis posterior tendon insertion.
-
Stress Fractures:
- Persistent symptoms despite adequate non-operative treatment (e.g., 6-8 weeks of non-weight-bearing).
- Displaced stress fractures (rare).
- Complete cortical break on imaging.
Contraindications for Surgical Intervention:
Absolute contraindications are few and generally relate to the patient's overall health status or local wound conditions.
- Severe comorbidities precluding safe anesthesia and surgery.
- Active infection in the surgical field.
- Extremely poor soft tissue envelope or severe crush injury making hardware coverage difficult.
- Non-displaced, stable fractures amenable to conservative management.
Table 1: Operative vs. Non-Operative Indications for Navicular Fractures
| Indication Type | Non-Operative Management | Operative Management |
|---|---|---|
| Acute Body Fx | Non-displaced (<2mm displacement), stable (Sangeorzan Type 1) | Displaced (≥2mm), Articular incongruity, Comminution (Sangeorzan Type 2 & 3), Open Fx, Midfoot collapse |
| Tuberosity Fx | Small, non-displaced avulsion (Watson-Jones Type 1) | Large, displaced fragment, Tibialis posterior tendon disruption, Articular involvement (Watson-Jones Type 2 & 3) |
| Stress Fx | Non-displaced, incomplete cortical break | Persistent symptoms despite NWB, Complete cortical break, Displaced stress fracture (rare) |
| Soft Tissue Env. | Optimal, minimal swelling | Poor soft tissue (relative contraindication for immediate surgery), Blistering |
| Patient Factors | Medically unstable, High surgical risk (relative) | Medically stable, Able to tolerate surgery |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is crucial for successful outcomes in navicular fracture management, especially given the bone's complex anatomy and high complication rate.
Imaging Review:
*
CT scan with 3D reconstructions:
This is the cornerstone of planning. Meticulously review axial, coronal, and sagittal cuts to understand the fracture pattern, degree of comminution, fragment size, articular involvement, and overall midfoot alignment. 3D reconstructions aid in visualizing the spatial relationship of fragments and planning reduction strategies.
*
Plain radiographs:
Reconfirm overall alignment and fracture patterns.
*
MRI:
If AVN is suspected or for occult stress fractures.
Surgical Timing:
*
Acute fractures:
Ideally, surgery should be performed after soft tissue swelling has subsided, indicated by the presence of a "wrinkle sign." This typically allows for better wound healing and reduced complication rates. In the interim, the foot should be elevated and splinted.
*
Open fractures:
Require immediate debridement and stabilization according to ATLS principles.
*
Highly displaced fractures with threatened skin:
May warrant urgent reduction, potentially temporary external fixation, followed by definitive fixation.
Approach Selection:
The choice of surgical approach depends on the fracture pattern and fragment location.
*
Dorsomedial:
Most common for navicular body fractures, allowing access to the majority of the dorsal and medial aspects.
*
Dorsolateral:
Less common, for fractures with significant lateral involvement or in combination with a dorsomedial approach for extensive comminution.
*
Medial:
Primarily for isolated navicular tuberosity fractures.
Implant Selection:
*
Screws:
Cannulated headless compression screws (e.g., 3.0mm, 3.5mm) are often preferred for interfragmentary compression and minimal profile, especially in articular areas. Cortical screws (e.g., 2.7mm, 3.5mm) can also be used.
*
Plates:
Low-profile locking plates (e.g., specifically designed navicular plates or small fragment plates) may be used for comminuted fractures, where screw-only fixation is insufficient for stability, or for dorsal comminution.
*
K-wires:
Useful for temporary reduction and stabilization, or for fixation of very small fragments.
*
Bone Graft:
Autologous (iliac crest or distal tibia) or allograft may be required for significant bone loss or to enhance union, particularly in comminuted or delayed cases.
Patient Positioning:
*
Supine position:
The patient is placed supine on the operating table.
*
Hip bolster:
A bolster is placed under the ipsilateral hip to internally rotate the limb slightly, improving access to the medial aspect of the foot.
*
Tourniquet:
A pneumatic tourniquet is applied high on the thigh to ensure a bloodless field, which is critical for meticulous dissection and fracture reduction.
*
Fluoroscopy:
The C-arm fluoroscope should be positioned to allow easy access for AP, lateral, and oblique views of the foot.
*
Preparation and draping:
Standard sterile preparation and draping from the thigh to the toes.
Detailed Surgical Approach / Technique
Surgical intervention for navicular fractures aims to achieve anatomical reduction of articular surfaces, restore medial column length and alignment, and provide rigid internal fixation.
Anesthesia: General or regional anesthesia (e.g., popliteal block) is appropriate.
Tourniquet: Inflate the thigh tourniquet to a pressure of 250-300 mmHg after limb exsanguination.
Incision & Approach (Dorsomedial Approach for Body Fractures – most common):
1.
Incision:
A curvilinear incision is made dorsomedially, centered over the navicular bone. The incision extends from the talonavicular joint proximally to the naviculocuneiform joints distally.
2.
Soft Tissue Dissection:
Meticulously identify and protect the saphenous nerve and superficial veins dorsally and medially. The internervous plane is typically between the tibialis anterior tendon (laterally) and the tibialis posterior tendon/flexor digitorum longus (medially).
3.
Capsular Incision:
Incise the joint capsule overlying the talonavicular and naviculocuneiform joints. Avoid excessive periosteal stripping, especially dorsally, to preserve tenuous blood supply.
Fracture Reduction:
1.
Distraction:
Initial longitudinal traction can aid in indirectly reducing collapsed or impacted fractures. A mini external fixator can provide controlled distraction.
2.
Visualization:
Clear the fracture hematoma to visualize the fracture fragments and articular surfaces.
3.
Indirect Reduction:
Use ligamentotaxis or manipulate the forefoot/hindfoot to help bring fragments into alignment.
4.
Direct Reduction:
* Utilize small pointed reduction clamps, bone hooks, or K-wires used as joysticks to manipulate fragments.
* Focus on restoring the talonavicular and naviculocuneiform articular congruity first. This is crucial for preventing post-traumatic arthritis.
* Restore the length of the medial column. Loss of length often indicates significant collapse.
* Fluoroscopic guidance is essential throughout the reduction process to confirm fragment alignment in multiple planes.
* Address comminution. Small, non-articular fragments may be excised if they impede reduction, but preservation is generally preferred. Articular fragments must be meticulously reduced.
5.
Temporary Fixation:
Once reduced, secure fragments with K-wires to maintain alignment.
Internal Fixation:
1.
Screw Fixation:
*
Interfragmentary compression:
Cannulated headless compression screws are frequently used for articular fragments. Place screws bicortically where possible, ensuring they do not penetrate the articular surface.
*
Lag screw principle:
Insert screws perpendicular to the fracture plane for maximal compression.
*
Talonavicular and Naviculocuneiform fixation:
Screws can be placed across these joints, or from the cuneiforms into the navicular, or from the navicular into the talus, depending on the fracture pattern and stability required.
*
Stress fracture fixation:
Often requires two cancellous screws placed perpendicular to the fracture plane for optimal compression and stability.
2.
Plate Fixation:
* For comminuted or unstable body fractures (Sangeorzan Type 3), a low-profile locking plate may be necessary to bridge comminuted segments and restore arch height.
* The plate is typically applied dorsally, ensuring minimal soft tissue stripping.
* Screws are placed through the plate into the intact bone segments (e.g., talus proximally, cuneiforms distally).
3.
Bone Grafting:
* If there is significant bone loss, a structural bone graft (autograft from iliac crest or distal tibia, or allograft) may be packed into the defect to support the reduction and promote healing. This is particularly relevant in type 2 or 3 fractures with associated compression and shortening.
* Cancellous bone graft chips can be used for smaller defects or to augment union in stress fractures.
Specific Considerations:
*
Navicular Tuberosity Fractures:
A separate medial incision over the tuberosity allows direct reduction and fixation with small screws (e.g., 2.7mm or 3.0mm) or K-wires, ensuring the tibialis posterior tendon is reattached securely.
*
Avascular Necrosis (AVN) Prevention:
Minimize periosteal stripping, maintain a bloodless field for only as long as necessary, and ensure stable fixation.
Closure:
1.
Irrigation:
Thoroughly irrigate the surgical site.
2.
K-wire removal:
Remove all temporary K-wires.
3.
Layered closure:
Close the capsule and subcutaneous layers with absorbable sutures. Close the skin with non-absorbable sutures or staples.
4.
Dressing:
Apply a sterile dressing and a well-padded splint (e.g., posterior splint with stirrups) in a neutral or slightly dorsiflexed position.
Complications & Management
Navicular fractures, particularly those involving the body, are associated with a high rate of complications due to the bone's tenuous blood supply, complex anatomy, and critical role in foot biomechanics.
Table 2: Common Complications of Navicular Fractures
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Avascular Necrosis (AVN) | 10-30% in body fractures | Non-operative: NWB, bracing. Operative: Core decompression, vascularized bone graft, talonavicular/naviculocuneiform arthrodesis (if symptomatic collapse/arthritis). |
| Nonunion/Malunion | 5-20% | Revision ORIF with bone grafting (autograft/allograft), structural allograft/autograft, interpositional arthrodesis, partial/total midfoot arthrodesis. |
| Post-traumatic Arthritis | 20-50% | Conservative (NSAIDs, injections, bracing), debridement, partial/total midfoot arthrodesis (talonavicular, naviculocuneiform). |
| Infection | 1-5% | Superficial: Oral antibiotics. Deep: IV antibiotics, surgical debridement, hardware removal (if stable union), implant retention (if no union). |
| Hardware Complications | 5-15% | Symptomatic hardware removal (after union), revision fixation if loosening/failure before union. |
| Nerve Injury | <5% (saphenous, sural) | Conservative (neuropathic pain management), neurolysis, surgical exploration if intractable. |
| Complex Regional Pain Syndrome (CRPS) | 1-5% | Multidisciplinary approach: physical therapy, pain management (nerve blocks, medications), psychological support. |
| Chronic Pain/Stiffness | Up to 30-40% | Aggressive physical therapy, bracing, custom orthotics, NSAIDs, injections. |
Detailed Management of Key Complications:
-
Avascular Necrosis (AVN):
- Pathophysiology: Disruption of the dorsal and plantar vascular supply, especially in the watershed area.
- Diagnosis: Persistent pain, imaging changes (sclerosis, collapse) on plain films, definitive diagnosis with MRI.
-
Management:
- Early/Pre-collapse: Strict non-weight-bearing, core decompression, potentially vascularized bone grafting (e.g., medial femoral condyle flap) to revascularize the fragment.
- Late/Collapse with Arthritis: If symptomatic and structural collapse has occurred, talonavicular and/or naviculocuneiform arthrodesis may be necessary to stabilize the medial column and alleviate pain.
-
Nonunion/Malunion:
- Pathophysiology: Inadequate reduction, unstable fixation, poor biology, excessive comminution, or unrecognized AVN. Malunion often results in residual deformity and mechanical symptoms.
- Diagnosis: Persistent pain, local tenderness, motion at the fracture site (nonunion), visible deformity or altered biomechanics (malunion), confirmed by plain films and CT scan.
-
Management:
- Nonunion: Revision ORIF with robust internal fixation, often augmented with autologous bone grafting (e.g., iliac crest or distal tibia) to stimulate healing. Structural allograft may be used for significant defects. If arthritis is present or joint congruence cannot be restored, a talonavicular and/or naviculocuneiform arthrodesis may be indicated.
- Malunion: Corrective osteotomy to restore alignment, potentially with bone grafting, followed by stable fixation. Arthrodesis may be considered if articular incongruity is severe or post-traumatic arthritis is established.
-
Post-traumatic Arthritis:
- Pathophysiology: Inadequate articular reduction, chondral damage at the time of injury, or altered biomechanics leading to accelerated degenerative changes.
- Diagnosis: Chronic pain, stiffness, crepitus, and joint space narrowing/osteophyte formation on radiographs, confirmed by CT.
-
Management:
- Conservative: NSAIDs, activity modification, custom orthotics, bracing, corticosteroid injections.
- Surgical: If conservative measures fail, arthrodesis of the involved joints (talonavicular and/or naviculocuneiform) is the definitive treatment to eliminate painful motion. Salvage procedures might involve joint debridement or partial arthroplasty in highly selected cases.
-
Infection:
- Pathophysiology: Introduction of bacteria during surgery or an open fracture.
- Diagnosis: Erythema, swelling, warmth, purulent drainage, elevated inflammatory markers.
- Management: Superficial infections may respond to oral antibiotics. Deep infections require aggressive surgical debridement, intravenous antibiotics, and potentially hardware removal (if union is achieved) or staged reconstruction.
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is essential for optimizing outcomes following surgical fixation of navicular fractures. The protocol must be individualized based on the fracture pattern, stability of fixation, and presence of complications.
Phase 1: Initial Immobilization & Non-Weight-Bearing (typically 6-12 weeks)
*
Goal:
Protect fixation, promote bone healing, manage pain and swelling.
*
Immobilization:
* Post-operatively, a well-padded splint (posterior splint with stirrups) is applied.
* After the initial swelling subsides (usually 1-2 weeks), transition to a non-weight-bearing (NWB) cast or CAM boot (Controlled Ankle Motion).
* The ankle is typically positioned in a neutral dorsiflexion-plantarflexion.
*
Weight-Bearing:
Strict non-weight-bearing (NWB) on the operative extremity. Ambulation with crutches or knee scooter.
*
Therapy:
*
Elevation:
Continue strict elevation of the foot above heart level to control swelling.
*
Cryotherapy:
Apply ice packs for pain and swelling management.
*
Toe ROM:
Gentle active range of motion (ROM) of the toes to maintain flexibility and promote circulation.
*
Quadriceps/Gluteal Strengthening:
Isometric exercises to maintain proximal muscle strength.
*
Core Stability:
Initiate core strengthening exercises.
*
Imaging:
Follow-up radiographs at 2 and 6 weeks to assess for maintenance of reduction and early signs of healing.
Phase 2: Gradual Weight-Bearing & Initial Motion (typically 6-12 weeks post-op onwards)
*
Goal:
Initiate weight-bearing, restore pain-free ROM, maintain fixation stability.
*
Progression:
* Once radiographic evidence of fracture healing is observed (usually at 6-12 weeks, depending on fracture type and stability), transition from NWB to partial weight-bearing (PWB) in a CAM boot. PWB starts at 25% of body weight, progressing by 25% increments each week as tolerated.
* Discontinue the CAM boot when full weight-bearing (FWB) is achieved without pain, typically around 12-16 weeks post-op.
*
Therapy:
*
Ankle ROM:
Begin gentle active and passive ankle ROM exercises (dorsiflexion, plantarflexion, inversion, eversion). Avoid aggressive forced movements across the midfoot initially.
*
Subtalar ROM:
Gentle subtalar motion as tolerated.
*
Midfoot Mobilization:
Very gentle manual mobilization, ensuring no stress on the healing fracture.
*
Gait Training:
Focus on proper gait mechanics with progressive weight-bearing.
*
Scar Massage:
Once incision is healed, to prevent adhesions.
*
Imaging:
Follow-up radiographs every 4-6 weeks to monitor healing. CT scan may be indicated if there is concern for delayed union.
Phase 3: Strengthening & Advanced Function (typically 12-16 weeks post-op onwards)
*
Goal:
Restore full strength, flexibility, balance, and prepare for return to activity.
*
Progression:
* Once FWB is achieved without pain, transition out of the CAM boot into supportive athletic shoes.
* Progress from light resistance exercises to moderate and then advanced strengthening.
*
Therapy:
*
Targeted Strengthening:
* Tibialis anterior, tibialis posterior, peroneals, triceps surae.
* Intrinsic foot muscles (short foot exercises).
*
Proprioception & Balance:
Single-leg stance, wobble board, balance beam exercises.
*
Agility Drills:
Lateral shuffles, controlled cutting, low-impact plyometrics (as appropriate for athletic patients).
*
Cardiovascular Conditioning:
Cycling, swimming, elliptical trainer.
*
Return to Activity:
Gradual return to activities of daily living and work. For athletes, a phased return to sport typically begins at 4-6 months, guided by functional testing and pain levels. High-impact sports may require 6-12 months or longer.
Long-Term Considerations:
*
Orthotics:
Custom orthotics may be beneficial for ongoing arch support and biomechanical correction, especially in cases of residual midfoot instability or pronation.
*
Hardware Removal:
If symptomatic, hardware removal may be considered typically after 12-18 months, once complete fracture healing is confirmed.
Summary of Key Literature / Guidelines
The management of navicular fractures has evolved with advances in imaging and surgical techniques, though the fundamental principles remain centered on anatomical reduction and rigid internal fixation.
The Sangeorzan classification remains the cornerstone for acute navicular body fractures, guiding the decision-making process between non-operative and operative management. Type 1 fractures, if truly non-displaced, are often managed with non-weight-bearing cast immobilization for 6-8 weeks, followed by gradual return to weight-bearing. However, the literature emphasizes the critical need for advanced imaging (CT) to accurately assess displacement and articular involvement, as subtle displacement can be missed on plain radiographs.
For Sangeorzan Type 2 and 3 fractures , open reduction and internal fixation (ORIF) is the standard of care. Studies by Sangeorzan et al. and Main and Jowett underscored the poor outcomes associated with non-operative management of displaced fractures, leading to high rates of nonunion, malunion, and post-traumatic arthritis. The surgical goals are to restore anatomical alignment, reconstruct the medial column, and achieve stable fixation. Dorsomedial approaches are favored, and fixation typically involves cannulated headless compression screws for interfragmentary compression, often supplemented with low-profile dorsal locking plates for comminuted or unstable fractures. The use of bone graft, particularly autograft, is frequently recommended for defects or comminution to promote healing and restore structural integrity.
The risk of avascular necrosis (AVN) is a significant concern, especially in comminuted or highly displaced body fractures. While the exact incidence varies in literature, it is consistently reported as a major complication. Early, accurate diagnosis and meticulous surgical technique aimed at preserving periosteal blood supply are critical. Post-traumatic arthritis, particularly involving the talonavicular and naviculocuneiform joints, is a common long-term sequela, even with successful ORIF. This often necessitates secondary procedures such as midfoot arthrodesis.
Navicular stress fractures , prevalent in athletes, are typically managed non-operatively with strict non-weight-bearing for 6-8 weeks in a cast or boot. However, in cases of complete cortical breach on MRI/CT, displacement, or failure of conservative management, surgical fixation with two parallel cannulated screws is often performed to expedite healing and facilitate earlier return to sport. Torg et al.'s work in the 1980s highlighted the efficacy of surgical management for these recalcitrant stress fractures.
Current literature emphasizes:
*
Pre-operative CT:
Mandatory for comprehensive assessment and surgical planning of acute navicular body fractures.
*
Anatomic Reduction:
Paramount for minimizing the risk of post-traumatic arthritis.
*
Stable Fixation:
Use of a combination of screws and plates may be required for complex patterns.
*
Bone Grafting:
Consider for significant comminution or bone defects.
*
Aggressive Rehabilitation:
A structured and progressive rehabilitation protocol is key to restoring function and preventing stiffness.
Despite advancements, navicular fractures remain challenging injuries. While surgical outcomes have improved, long-term complications such as AVN, nonunion, and post-traumatic arthritis necessitate thorough pre-operative counseling and diligent follow-up. Continuous research aims to refine surgical techniques, improve implant design, and optimize biological healing to further enhance patient outcomes.
You Might Also Like


