Tibialis Posterior Tendon Debridement: A Comprehensive Review of Indications, Anatomy, and Outcomes in PTTD Management

Key Takeaway
Tibial tendon debridement is a surgical procedure for chronic posterior tibial tendon dysfunction (PTTD), often called adult-acquired flatfoot. It's indicated for recalcitrant tendinosis, partial tears, or inflammatory tenosynovitis when non-operative treatments fail, particularly in Stage I PTTD. It may also be an adjunctive procedure in more advanced reconstructive strategies, restoring foot mechanics.
Introduction & Epidemiology
Chronic foot pain attributable to the tibialis posterior tendon is a prevalent and often debilitating condition, primarily stemming from posterior tibial tendon dysfunction (PTTD), also known as adult-acquired flatfoot deformity (AAFD). This progressive disorder affects the primary dynamic stabilizer of the medial longitudinal arch, leading to a spectrum of pathologies ranging from isolated tendinosis to complete tendon rupture and subsequent progressive flatfoot deformity.
Epidemiologically, PTTD predominantly affects middle-aged and older adults, with a higher incidence observed in women, particularly those who are obese or have co-morbidities such as hypertension, diabetes, or inflammatory arthropathies. The prevalence is estimated to be between 3% and 10% in the adult population over 40 years of age, though exact figures are challenging due to its often insidious onset and variable clinical presentation. The condition typically manifests as medial ankle and foot pain, swelling, and progressive loss of arch height, eventually leading to hindfoot valgus and forefoot abduction.
Tibial tendon debridement, as a surgical intervention, is typically indicated for recalcitrant tendinosis, partial tears, or inflammatory tenosynovitis of the tibialis posterior tendon that has failed comprehensive non-operative management. While isolated debridement may be considered for early-stage pathology (Johnson & Strom Stage I), it is more frequently performed as an adjunctive procedure within the context of a broader reconstructive strategy for more advanced stages (e.g., Stage II PTTD), where it is combined with procedures such as flexor digitorum longus (FDL) tendon transfer, calcaneal osteotomies, and/or spring ligament repair. This review aims to delineate the rationale, indications, techniques, and outcomes associated with tibial tendon debridement in the contemporary orthopedic surgical landscape.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the tibialis posterior tendon and its surrounding structures is paramount for effective diagnosis and surgical management of PTTD.
The tibialis posterior muscle originates from the posterior surface of the tibia, fibula, and interosseous membrane. Its tendon courses distally, passing posterior to the medial malleolus within a synovial sheath, where it occupies the most anterior compartment of the tarsal tunnel. Distal to the medial malleolus, the tendon broadens and trifurcates, with its primary insertion onto the navicular tuberosity. Secondary insertions include the sustentaculum tali, all three cuneiforms, the cuboid, and the bases of the second, third, and fourth metatarsals. These widespread insertions allow the tibialis posterior to effectively invert and adduct the foot, as well as powerfully plantarflex the ankle.
Vascular supply to the tibialis posterior tendon is segmental, primarily derived from branches of the posterior tibial artery and its perimalleolar anastomoses. Areas of relative hypovascularity, particularly posterior to the medial malleolus, are theorized to predispose the tendon to degenerative changes and tendinosis, contributing to its vulnerability. Innervation is provided by the tibial nerve (L4-S1).
Biochemically, the tibialis posterior tendon is the primary dynamic stabilizer of the medial longitudinal arch. Its concentric contraction facilitates supination of the subtalar joint and adduction of the forefoot, effectively "locking" the midtarsal joint and elevating the arch during the propulsive phase of gait. During the stance phase, it acts eccentrically to control pronation. Dysfunction of this tendon leads to a cascade of biomechanical failures:
1.
Loss of Arch Support:
As the tendon degenerates and elongates, its ability to support the arch diminishes, leading to progressive midfoot collapse.
2.
Hindfoot Valgus:
The calcaneus moves into a valgus position relative to the tibia, resulting in a 'too many toes' sign from a posterior view.
3.
Forefoot Abduction:
The forefoot abducts on the hindfoot, disrupting the alignment of the talonavicular and calcaneocuboid joints.
4.
Secondary Ligamentous Laxity:
Chronic stress leads to attenuation or rupture of secondary stabilizers such as the spring ligament (plantar calcaneonavicular ligament) and the deltoid ligament complex.
5.
Compensatory Gastroc-Soleus Contracture:
Often, an equinus contracture develops, further exacerbating the collapse and increasing stress on the medial structures.
Adjacent structures that are intimately involved in PTTD and often require concurrent attention include the flexor digitorum longus (FDL) and flexor hallucis longus (FHL) tendons, which also course through the tarsal tunnel. The FDL tendon is particularly relevant as it serves as the most common choice for transfer procedures when the tibialis posterior tendon is irreparably diseased. The spring ligament, located inferior and medial to the talar head, is a crucial static stabilizer; its integrity is often compromised in PTTD and must be assessed. The deltoid ligament complex, on the medial aspect of the ankle, provides stability against valgus stress; its attenuation can lead to ankle valgus in advanced PTTD (Stage IV). Understanding these intricate relationships is crucial for precise surgical planning and execution, ensuring comprehensive restoration of foot mechanics.
Indications & Contraindications
The decision to proceed with tibial tendon debridement, whether as a standalone procedure or part of a larger reconstruction, is predicated on a careful assessment of the patient's symptoms, physical examination findings, and imaging studies, within the context of the Johnson and Strom classification system for PTTD.
Indications for Tibial Tendon Debridement
- Stage I PTTD (Johnson & Strom Classification): This represents the earliest stage, characterized by pain and swelling along the course of the tibialis posterior tendon, tendinosis or tenosynovitis without significant lengthening or rupture of the tendon, and a flexible flatfoot deformity with normal hindfoot alignment. Surgical debridement is considered only after a minimum of 6-9 months of comprehensive non-operative management (e.g., orthotics, physical therapy, NSAIDs, activity modification) has failed to alleviate symptoms.
- Early Stage II PTTD: In cases where the tibialis posterior tendon exhibits significant tendinosis, partial tearing, or inflammatory changes, but retains reasonable structural integrity and function, debridement may be performed as part of a multi-component reconstruction. This often involves excising diseased segments of the tendon and repairing any longitudinal tears, usually in conjunction with a flexor digitorum longus (FDL) tendon transfer and a medializing calcaneal osteotomy to correct hindfoot valgus.
- Chronic Tenosynovitis: Isolated debridement and tenosynovectomy may be indicated for chronic, symptomatic tenosynovitis of the tibialis posterior tendon where imaging demonstrates significant synovial inflammation and hypertrophy, particularly if it contributes to impingement or pain, without substantial intrinsic tendon degeneration.
- Intratendinous Mucoid Degeneration: Surgical exploration may reveal areas of mucoid degeneration or ganglion formation within the tendon, which can be debrided to alleviate pain and improve function.
- Adjunctive to Tendon Transfer: When an FDL transfer is performed for Stage II PTTD, the diseased tibialis posterior tendon is often debrided. If a significant portion is irreparable, it might be excised and the FDL tendon tenodesed into the remaining distal stump or bone.
- Failed Previous Debridement with Residual Pathology: In select cases, if a prior debridement was incomplete or the pathology has recurred locally, a revision debridement might be considered, provided the tendon quality is still adequate.
Contraindications for Tibial Tendon Debridement
-
Advanced PTTD (Stage III and IV):
- Stage III: Characterized by a rigid flatfoot deformity, often with fixed hindfoot valgus and forefoot abduction, and degenerative arthritis of the subtalar and/or talonavicular joints. Debridement alone or even with soft tissue procedures is insufficient; arthrodesis (e.g., triple arthrodesis) is typically indicated.
- Stage IV: Involves ankle valgus and deltoid ligament insufficiency in addition to the Stage III deformities. Requires more extensive fusion procedures, possibly including tibiotalocalcaneal arthrodesis.
- Complete Tibial Tendon Rupture: If the tendon is completely ruptured and retracted, isolated debridement is inappropriate. Primary repair, if feasible, or more commonly, tendon transfer with or without augmentation, is required.
- Severe Underlying Deformity: If the primary issue is a significant bony deformity (e.g., severe hindfoot valgus, forefoot abduction, equinus contracture) that is not addressed by debridement, the procedure will likely fail.
- Active Infection: Any active local or systemic infection is a contraindication to elective surgical intervention.
- Severe Peripheral Vascular Disease: Compromised vascularity can impair wound healing and tendon repair, increasing complication rates.
- Uncontrolled Systemic Conditions: Uncontrolled diabetes, severe inflammatory arthropathy, or other conditions that compromise healing should be optimized prior to surgery.
- Unrealistic Patient Expectations or Non-Compliance: Patients must understand the potential limitations of debridement and commit to a rigorous post-operative rehabilitation protocol.
Operative vs. Non-Operative Indications
The table below summarizes the key differential indications for operative debridement versus continued non-operative management for tibialis posterior tendon pathology.
| Indication Category | Operative (Debridement) | Non-Operative |
|---|---|---|
| Pain/Dysfunction | Persistent, severe medial ankle/foot pain localized to the tibialis posterior tendon, unrelieved by conservative measures for >6-9 months. Functional limitations due to pain or weakness. | Mild-to-moderate pain, intermittent symptoms, or symptoms of recent onset. Functional limitations that are tolerable or respond well to activity modification. |
| Tendon Pathology (MRI/US) | Documented tendinosis (thickening, signal changes), partial longitudinal tears (<50% tendon involvement), significant tenosynovitis with effusion/hypertrophy, or intratendinous mucoid degeneration. Mild elongation without complete rupture. | Mild inflammatory changes, minimal tendinosis, no definitive tears or only early, subtle signal changes. Tendon largely intact and functional. |
| Deformity (Clinical/XR) | Johnson & Strom Stage I (flexible flatfoot, normal alignment), or early Stage II (flexible hindfoot valgus, forefoot abduction) where the tibialis posterior tendon is salvagable. Surgical debridement often combined with adjunctive bony/ligamentous procedures for Stage II. | Flexible flatfoot with normal or easily correctable alignment. Early signs of arch collapse without fixed deformity. Hindfoot can be passively corrected to neutral or slight valgus. |
| Conservative Treatment | Failure of an extended course (e.g., 6-9 months) of structured non-operative management including custom orthotics/bracing, physical therapy, NSAIDs, activity modification, and sometimes corticosteroid injections (used judiciously to avoid tendon weakening or rupture). | Initial presentation of symptoms. Successful alleviation or significant improvement of symptoms with orthotics, physical therapy, NSAIDs, and activity modification. |
| Patient Factors | Patient is medically fit for surgery, has realistic expectations, and demonstrates commitment to post-operative rehabilitation. | Co-morbidities precluding safe surgery. Unwillingness or inability to comply with post-operative restrictions and rehabilitation. Advanced age or low functional demand where conservative measures suffice. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for optimizing surgical outcomes and minimizing complications in tibial tendon debridement.
Diagnostic Workup
-
Clinical Assessment:
A comprehensive history identifying the onset, duration, character, and aggravating/alleviating factors of pain. Physical examination focuses on:
- Inspection: Assessment of arch height, hindfoot alignment (too many toes sign), forefoot abduction.
- Palpation: Tenderness along the tibialis posterior tendon sheath posterior to the medial malleolus and at its insertion.
- Range of Motion (ROM): Ankle dorsiflexion, plantarflexion, subtalar inversion/eversion. Assessment for equinus contracture.
- Strength Testing: Resistance to ankle inversion and plantarflexion.
- Functional Tests: Single limb heel rise test (inability to perform or pain is highly indicative of PTTD), gait analysis.
- Flexibility Assessment: Passive correction of hindfoot valgus and forefoot abduction to differentiate flexible from rigid deformities.
-
Imaging Studies:
- Weight-Bearing Radiographs: AP, lateral, and oblique views of the foot and ankle. Essential for assessing arch collapse (e.g., Talo-Navicular Coverage Angle, Meary's Angle), hindfoot alignment (Harris view for hindfoot valgus), and ruling out associated bony pathology or arthritis.
- Magnetic Resonance Imaging (MRI): The gold standard for soft tissue evaluation. Provides detailed information on tendon integrity (tendinosis, partial tears, full ruptures, tenosynovitis), assessment of the spring ligament, and identification of associated inflammatory changes or stress responses in surrounding bone. This is crucial for guiding the extent of debridement and determining the need for adjunctive procedures.
- Ultrasound (US): A dynamic and cost-effective alternative for assessing tendon pathology, particularly tenosynovitis and partial tears, though operator-dependent.
Pre-Operative Consultation & Consent
Discuss the diagnosis, surgical plan (including potential adjunctive procedures), expected outcomes, and comprehensive list of potential risks and complications (infection, nerve injury, persistent pain, stiffness, recurrence, hardware issues). Ensure patient understanding and realistic expectations.
Anesthesia
Regional anesthesia (e.g., popliteal block, spinal, or epidural) often combined with general anesthesia is preferred. A regional block provides excellent post-operative pain control, reducing the need for systemic narcotics.
Patient Positioning
The patient is positioned supine on the operating table.
* A padded tourniquet is applied to the proximal thigh or calf to ensure a bloodless field during the procedure.
* The operative extremity is prepared and draped in a sterile fashion, typically from the mid-calf to the toes.
* The hip on the operative side is often abducted and externally rotated, or a small bump/pillow can be placed under the ipsilateral hip, to allow for optimal access to the medial aspect of the ankle and foot. The foot should be positioned to allow easy manipulation and visualization of the medial aspect of the hindfoot and midfoot.
* Consideration should be given to intraoperative fluoroscopy if concomitant osseous procedures (e.g., calcaneal osteotomy, navicular drill hole for FDL transfer) are planned, requiring C-arm access.

Figure 1: Pre-operative MRI depicting significant posterior tibial tendon pathology (tendinosis, partial tearing, and tenosynovitis) consistent with early-stage PTTD.
Detailed Surgical Approach / Technique
The surgical approach for tibial tendon debridement requires precision, careful soft tissue handling, and an understanding of potential concomitant pathologies. The following describes a standard open technique, which remains the gold standard for extensive debridement or when combined with reconstructive procedures.
Incision
A curvilinear or straight longitudinal incision is typically made on the medial aspect of the ankle and foot, extending from approximately 2 cm proximal to the tip of the medial malleolus distally to the level of the navicular tuberosity. The incision should be centered over the palpable course of the tibialis posterior tendon. Careful planning is essential to avoid direct placement over future potential sites of hardware if osteotomies or fusions are anticipated.
Dissection
- Skin and Subcutaneous Tissue: The incision is carried through the skin and subcutaneous fat. Meticulous hemostasis is achieved.
- Identification of Neurovascular Structures: Extreme care must be taken to identify and protect the great saphenous vein and the saphenous nerve, which typically lie anterior to the incision line, superficial to the deep fascia. These structures should be gently retracted anteriorly. The medial calcaneal nerve branches, arising from the tibial nerve, may also be encountered posteriorly and require protection.
- Deep Fascia & Tendon Sheath: The deep fascia overlying the tibialis posterior tendon sheath is incised longitudinally. The synovial sheath itself is then opened carefully along its entire length, exposing the tendon. A segment of the tendon sheath may be excised if severely inflamed (tenosynovectomy), or left for primary closure later.
Tendon Examination
Once the tendon is exposed, a thorough visual inspection and palpation of its entire accessible length are performed.
*
Assessment of Pathology:
Note areas of hyperemia, edema, fibrillar disorganization, intratendinous degeneration, mucoid changes, fraying, or longitudinal partial tears. The quality and thickness of the tendon are assessed.
*
Dynamic Assessment:
Gentle manipulation of the foot (dorsiflexion, plantarflexion, inversion, eversion) can help visualize the tendon's excursion and identify areas of impingement or restricted movement.
Debridement
- Synovectomy: If significant tenosynovitis is present, inflamed and hypertrophied synovial tissue is meticulously excised using fine instruments (e.g., tenotomy scissors, small scalpel, or rongeur). This reduces inflammation and provides better visualization of the tendon.
- Excision of Degenerated Tissue: Areas of frank mucoid degeneration, necrotic tissue, or severely frayed tendon fibers are carefully excised. This is typically performed using a scalpel, making longitudinal incisions into the diseased areas, followed by debridement. The goal is to remove non-viable tissue while preserving as much healthy, functional tendon as possible.
- Repair of Partial Tears: If longitudinal partial tears are identified, the edges are debrided minimally to healthy tissue. The tear is then repaired with a running locking stitch using a non-absorbable, braided suture (e.g., 2-0 or 3-0 Fiberwire, Ethibond) to restore the tendon's bulk and prevent further propagation of the tear. Transverse tears are much less common in PTTD, but if present and small, can be repaired. If a large segment is completely ruptured, isolated debridement is insufficient, and tendon transfer is indicated.
- Tendon Augmentation (If Necessary): In some cases, after debridement, the remaining tendon may appear significantly attenuated. Augmentation with local tendon tissue (e.g., tenodesing the FDL to the tibialis posterior) or allograft may be considered, although this moves beyond isolated debridement into reconstructive territory.
Concurrent Procedures (Most Commonly Performed with Debridement)
Given that isolated debridement often has a high failure rate in the presence of underlying biomechanical instability, it is frequently combined with other procedures for Stage II PTTD:
-
Flexor Digitorum Longus (FDL) Tendon Transfer:
- The FDL tendon, located posterior to the tibialis posterior within the tarsal tunnel, is identified and isolated.
- It is detached distally, typically through a separate plantar incision or via the primary medial incision by carefully identifying its crossing with the FHL (Master Knot of Henry).
- The FDL tendon is then rerouted anteriorly through the tibialis posterior tendon sheath or subcutaneously.
- A drill hole is created in the navicular tuberosity or the plantar aspect of the medial cuneiform. The FDL is passed through this tunnel and secured with an interference screw, suture anchor, or tenodesed to the remaining tibialis posterior tendon stump. The tension must be meticulously set with the foot in slight plantarflexion and inversion.
-
Medializing Calcaneal Osteotomy:
- A lateral approach to the calcaneus is utilized (distinct from the medial incision for the PTT).
- A laterally based wedge or a simple transverse osteotomy is performed through the posterior tuberosity of the calcaneus, perpendicular to the long axis of the bone.
- The distal fragment is then translated medially, correcting the hindfoot valgus.
- Fixation is achieved with two or more cancellous screws.
-
Gastrocnemius Recession or Achilles Lengthening:
- Performed if an equinus contracture (restricted ankle dorsiflexion) is present.
- Multiple techniques exist (e.g., Strayer, Baumann, Vulpius, percutaneous Achilles lengthening). The specific choice depends on surgeon preference and the severity of the contracture.
-
Spring Ligament Repair/Reconstruction:
- If the spring ligament is attenuated or ruptured, it can be directly repaired with non-absorbable sutures or augmented with local tissue or allograft.
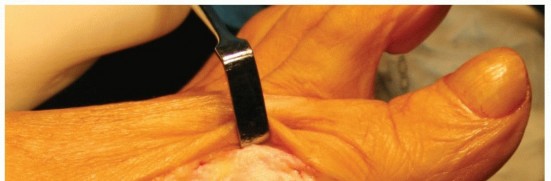
Figure 2: Intra-operative view demonstrating debridement of the posterior tibial tendon. Note the areas of fibrillar disorganization being meticulously resected, while healthy tendon tissue is preserved. Concomitant FDL transfer to the navicular has already been performed, indicated by the suture passing through the drill hole.
Wound Closure
- The tibialis posterior tendon sheath may be loosely closed or left open to minimize pressure on the healing tendon, depending on the amount of soft tissue swelling.
- The deep fascia is approximated.
- Subcutaneous tissues are closed in layers with absorbable sutures.
- Skin is closed with non-absorbable sutures or staples.
- A sterile dressing is applied, followed by a well-padded splint (typically a short leg posterior splint with the foot in slight plantarflexion and inversion) to protect the repair.
Complications & Management
While tibial tendon debridement can significantly improve outcomes, both general surgical and specific complications can occur. Comprehensive pre-operative counseling and vigilant post-operative care are essential for early detection and effective management.
General Surgical Complications
- Infection (1-5%): Superficial wound infection or deep space infection. Management involves culture-directed antibiotics, surgical debridement, and potentially hardware removal if involved.
- Wound Dehiscence (2-8%): Especially common in patients with diabetes, obesity, or venous insufficiency. Managed with local wound care, secondary closure, or skin grafting in severe cases.
- Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE) (<1%): Prophylaxis (chemical and mechanical) is often employed, especially for higher-risk patients or prolonged immobilization.
-
Nerve Injury (5-15%):
- Saphenous Nerve: Sensory nerve along the medial ankle/foot. Injury can cause paresthesias or numbness. Typically managed conservatively with NSAIDs and nerve blocks; surgical neurolysis for persistent symptomatic neuromas.
- Sural Nerve: Often affected with lateral approach for calcaneal osteotomy.
- Medial Calcaneal Nerve: Can be injured during dissection along the medial heel.
- Vascular Injury: Extremely rare with meticulous dissection.
Specific Complications Related to Tibial Tendon Debridement and Reconstruction
| Complication | Incidence (%) | Management Strategy |
|---|---|---|
| Persistent Pain / Failed Symptom Resolution | 10-30 |
Cause:
Inadequate debridement, unaddressed concomitant pathology (e.g., spring ligament rupture, undiagnosed tarsal coalition, subtalar arthritis), progression of PTTD, incomplete correction of deformity, or development of new pathology.
Management: Thorough diagnostic re-evaluation (clinical exam, repeat imaging - MRI, CT). Non-operative measures (PT, orthotics, injections). If surgical, may require revision surgery with more comprehensive reconstruction (e.g., FDL transfer if not done, calcaneal osteotomy, lateral column lengthening, subtalar or triple arthrodesis for rigid deformity). |
| Tendon Rupture (Post-debridement) | 5-10 |
Cause:
Excessive debridement leaving an attenuated tendon, failure of initial repair, or continued stress on a compromised tendon.
Management: If functional loss and pain are significant, revision surgery is often necessary. This typically involves an FDL tendon transfer (if not previously performed), allograft reconstruction, or, in severe cases of recurrent failure or high demand, considering a primary arthrodesis to stabilize the foot. |
| Overcorrection / Undercorrection of Deformity | 5-15 |
Cause:
Inaccurate execution of osteotomies (e.g., calcaneal osteotomy, lateral column lengthening) or inadequate soft tissue balancing.
Management: For minor asymptomatic deviations, conservative management with orthotics. For symptomatic, significant malalignment, revision osteotomy may be required after adequate bone healing (typically 6-12 months post-op), or potentially arthrodesis for salvage in severe, painful deformities. |
| Stiffness / Reduced Range of Motion (ROM) | 10-20 |
Cause:
Prolonged immobilization, scar tissue formation, or inadequate post-operative physical therapy.
Management: Aggressive physical therapy focused on early ROM and stretching. Dynamic splinting. Manipulation under anesthesia may be considered for refractory stiffness, although caution is advised if tendon repair sites are still healing. |
| Recurrence of Flatfoot Deformity | 5-15 |
Cause:
Often due to progression of underlying disease, inadequate initial correction of all components of the deformity (bony, ligamentous, tendinous), or non-compliance with post-operative rehabilitation and orthotic use.
Management: Similar to persistent pain, requiring re-evaluation and typically revision surgery with more extensive reconstructive procedures, potentially including additional osteotomies, ligament reconstructions, or arthrodesis for fixed deformities. |
| Hardware Irritation / Prominence | 5-10 (if osteotomies performed) |
Cause:
Screws or plates used for osteotomies or tendon transfers causing impingement on soft tissues, particularly in the subcutaneous medial ankle region.
Management: Symptomatic hardware removal is typically performed after complete bone healing, usually 6-12 months post-operatively. |
| Sural Nerve Irritation / Neuroma | 5-15 |
Cause:
Direct trauma during lateral approach for calcaneal osteotomy or scar tissue impingement.
Management: Conservative management for neuropraxia (NSAIDs, gabapentin, local injections). Surgical exploration and neurolysis for persistent, debilitating symptoms; excision of neuroma with transposition or burial if necessary. |
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is paramount to the success of tibial tendon debridement and associated reconstructive procedures. Adherence to these protocols is critical for tendon healing, restoration of strength, and functional recovery. The timeline outlined below is a general guideline; individual progression should be based on patient healing, pain levels, and surgeon's assessment.
Phase I: Immobilization and Non-Weight Bearing (Weeks 0-6)
- Goals: Protect surgical repair, minimize pain and swelling, promote initial soft tissue healing.
-
Week 0-2:
- Immobilization: Short leg posterior splint (or cast) with the foot in slight plantarflexion and inversion.
- Weight Bearing: Strict non-weight bearing (NWB) with crutches or walker.
- Activity: Strict elevation of the operative limb, regular icing, pain medication as prescribed.
- Exercises: Gentle range of motion (ROM) of non-involved joints (knee, hip). Toe wiggles within the splint to encourage circulation.
-
Week 2-6:
- Immobilization: Transition to a removable short leg walking boot (CAM walker) or continued casting, still maintaining some plantarflexion and inversion.
- Weight Bearing: Continued NWB or touch-down weight bearing (TDWB) only, with strict instruction not to load the operative foot.
- Exercises: Begin gentle active and passive ankle ROM exercises (dorsiflexion, plantarflexion, inversion, eversion) within a pain-free range, only if cleared by surgeon and for isolated debridement cases without significant tendon repair or transfer. If FDL transfer or significant PTT repair, delay active ROM for at least 4-6 weeks to allow tendon integration. Initiate isometric exercises for glutes, quadriceps, and hamstrings of the operative leg to maintain muscle bulk.
Phase II: Protected Weight Bearing and Early Mobilization (Weeks 6-12)
- Goals: Gradually restore full weight bearing, improve ankle and foot ROM, initiate muscle strengthening.
-
Week 6-8:
- Weight Bearing: Gradual progression from TDWB to partial weight bearing (PWB) in the CAM boot, advancing as tolerated based on pain and surgeon's assessment.
-
Exercises:
- Continue with full pain-free ankle ROM exercises.
- Begin gentle resisted exercises for ankle dorsiflexion, plantarflexion, inversion, and eversion, using therapist assistance, elastic bands, or light weights. Focus on tibialis posterior strengthening (inversion/plantarflexion).
- Initiate stationary cycling with light resistance (in CAM boot initially).
- Gait training with crutches, focusing on proper heel-to-toe pattern.
-
Week 8-12:
- Weight Bearing: Progressive increase to full weight bearing (FWB) in the CAM boot, then transition to a supportive lace-up shoe with a custom or over-the-counter orthotic.
-
Exercises:
- Continue and advance strengthening exercises for all ankle and foot musculature.
- Begin proprioceptive training: single leg balance, wobble board activities (within controlled range).
- Stretching exercises for the gastroc-soleus complex if any tightness is present.
- Pool exercises (walking, gentle swimming) can be beneficial for buoyancy-assisted movement.
Phase III: Advanced Strengthening and Return to Function (Weeks 12-24+)
- Goals: Restore full strength, endurance, agility, and return to prior activity levels.
-
Week 12-16:
- Weight Bearing: FWB in supportive shoes with orthotics.
-
Exercises:
- Progressive resistance exercises with increased weight/bands.
- Eccentric calf raises and heel raises, focusing on controlled descent.
- Initiate functional activities: walking on uneven surfaces, stepping up/down, lunges.
- Begin light jogging/running progression on soft surfaces if pain-free and strength is sufficient, but with caution for PTTD patients.
-
Month 4-6+:
-
Exercises:
- Sport-specific drills, agility training (cutting, jumping).
- Plyometrics (if appropriate for the individual and initial injury).
- Continued focus on strengthening, endurance, and proprioception.
- Return to Activity: Gradual return to full work duties and recreational activities, typically by 6 months. High-impact sports may require 9-12 months or longer. Long-term use of supportive footwear and custom orthotics is often recommended to maintain arch support and protect the tibialis posterior tendon from recurrent stress.
-
Exercises:
Key Considerations:
*
Patient Education:
Emphasize the importance of long-term compliance with orthotics and a home exercise program.
*
Listen to Pain:
Pain should be the guiding factor for progression. Any sharp increase in pain, swelling, or signs of inflammation warrants a re-evaluation by the surgeon.
*
Individualization:
Protocols must be tailored to the specific surgical procedure (debridement alone vs. debridement with FDL transfer, osteotomy, etc.), the extent of pathology, and the patient's individual healing capacity and functional goals.
Summary of Key Literature / Guidelines
The body of literature concerning posterior tibial tendon dysfunction (PTTD) and its surgical management, including tibial tendon debridement, has evolved significantly, leading to a generally accepted staging system and treatment algorithms.
Staging Systems and Their Impact on Treatment
The most widely adopted classification system is the
Johnson and Strom (1989)
system, later modified by
Myerson (1996)
. This system guides treatment decisions:
*
Stage I:
Characterized by tenosynovitis and/or tendinosis of the tibialis posterior tendon, with intact tendon length, no deformity, and mild pain. Non-operative management is the cornerstone. If refractory, isolated debridement and tenosynovectomy
may
be considered, though long-term outcomes for isolated debridement for Stage I have shown variable success, with some studies indicating a potential for progression.
*
Stage II:
Involves tendon elongation and dysfunction, flexible hindfoot valgus, and forefoot abduction. The literature strongly supports a reconstructive approach for Stage II, typically involving an
FDL tendon transfer, medializing calcaneal osteotomy
, and frequently
tibial tendon debridement/excision of pathological segments
. Spring ligament repair/reconstruction and gastrocnemius recession are often added. Studies consistently show good to excellent outcomes in 80-90% of patients undergoing this combined approach, with significant pain relief and deformity correction at medium-term follow-up (Haddad et al., 2007; Saxena et al., 2011).
*
Stage III:
Defined by a rigid flatfoot deformity, often with significant degenerative changes in the subtalar and/or talonavicular joints. Soft tissue procedures are ineffective.
Arthrodesis (e.g., triple arthrodesis)
is the gold standard for pain relief and stable deformity correction (Pomeroy et al., 1999).
*
Stage IV:
Includes the deformities of Stage III plus ankle valgus due to deltoid ligament insufficiency. Management typically involves
ankle fusion (tibiotalar arthrodesis)
in addition to hindfoot fusion.
Role of Imaging
Magnetic Resonance Imaging (MRI) is consistently highlighted as the most valuable imaging modality for diagnosing PTTD, staging the disease, and guiding surgical planning. It allows for detailed assessment of tendon integrity (tendinosis, partial/full tears), tenosynovitis, and concurrent pathologies such as spring ligament tears or fatty degeneration of the tibialis posterior muscle. Weight-bearing radiographs remain crucial for assessing bony alignment and deformity.
Outcomes of Tibial Tendon Debridement (Standalone vs. Adjunctive)
- Isolated Debridement: For true Stage I PTTD, characterized by tendinosis and inflammation without significant deformity or tendon elongation, isolated debridement (including tenosynovectomy and excision of degenerative tissue) can provide symptomatic relief. However, the literature suggests that its efficacy as a standalone procedure is limited if the underlying biomechanical deficiencies contributing to the tendinopathy are not addressed. Rates of persistent pain or recurrence can be significant, leading some authors to advocate for considering early bony procedures (e.g., medializing calcaneal osteotomy) even in Stage I if there is subtle biomechanical compromise.
- Adjunctive Debridement in Stage II Reconstruction: When performed as part of a comprehensive Stage II reconstruction (FDL transfer, calcaneal osteotomy), debridement of the tibialis posterior tendon is a standard component. Its role is to remove a source of ongoing pain and inflammation, and to prepare the site for FDL transfer if the PTT stump is utilized. The excellent outcomes seen in Stage II reconstructions are attributed to the synergistic effect of addressing all components of the deformity (tendon, bone, ligament), rather than isolated debridement alone.
Current Trends and Future Directions
Current literature emphasizes a comprehensive, individualized approach to PTTD. Key themes include:
*
Early Diagnosis:
Prompt recognition and aggressive non-operative management are crucial.
*
Multifaceted Surgical Correction:
For Stage II and beyond, surgical plans should address all aspects of the deformity (tendon dysfunction, hindfoot valgus, forefoot abduction, equinus contracture, spring ligament insufficiency).
*
Biologic Augmentation:
The use of platelet-rich plasma (PRP) or stem cells as an adjunct in tendon healing remains an area of ongoing research, with inconclusive evidence for routine use in PTTD.
*
Minimally Invasive Approaches:
Arthroscopic or endoscopic tenosynovectomy and debridement are emerging techniques for highly selected cases of early, isolated tendinopathy, aiming to reduce morbidity. However, these are often limited in scope and may not be suitable for comprehensive reconstruction.
In conclusion, while tibial tendon debridement can be a valuable component of managing chronic foot pain related to the tibialis posterior tendon, its indications are increasingly refined. For true Stage I tendinosis, it is a secondary option after failed conservative care. For Stage II, it is almost invariably an adjunctive procedure within a broader reconstructive framework. Surgeons must meticulously stage the disease, evaluate all contributing factors, and formulate a comprehensive treatment plan to achieve durable clinical success.
You Might Also Like