Dorsal Midfoot Approaches: Surgical Anatomy, Indications, & Techniques
Key Takeaway
Dorsal midfoot surgical approaches provide critical access for diverse pathologies from the talonavicular to tarsometatarsal joints. These interventions are vital for treating Lisfranc injuries, midfoot fractures, painful degenerative arthritis, and excising exostoses. Mastery requires precise anatomical knowledge of the navicular, cuboid, cuneiforms, ligaments, and neurovascular structures, enabling effective fixation and fusion procedures.
Mastering Dorsal Approaches to the Middle Part of the Foot
Introduction & Epidemiology
The middle part of the foot encompasses the region from the calcaneocuboid (CC) and talonavicular (TN) joints proximally to the tarsometatarsal (TMT) or Lisfranc joints distally. This complex anatomical segment includes the navicular, cuboid, and three cuneiform bones, articulating with each other and with the bases of the metatarsals. While these bones and their associated joints are superficial and accessible via dorsal, medial, lateral, and plantar approaches, the dorsal approaches are paramount for a wide array of surgical interventions.
Operations in this area, though not as frequently performed as forefoot or ankle procedures, are critical for addressing specific pathologies related to trauma, degenerative conditions, and congenital or acquired deformities. The seed content correctly highlights the insertions of powerful muscles controlling foot inversion and eversion (tibialis anterior, peroneus longus, peroneus brevis, tibialis posterior), which are often involved in tendon transfers or repairs via dorsal or dorsomedial approaches. Beyond muscle imbalance and mobile flatfoot, dorsal approaches are primarily indicated for:
* Open reduction and internal fixation (ORIF) of midfoot fractures and fracture-dislocations, notably Lisfranc injuries.
* Arthrodesis for painful degenerative arthritis or severe deformities.
* Excision of symptomatic dorsal exostoses (tarsal bosses) or accessory navicular bones.
* Debridement of infections or biopsies of lesions.
Epidemiologically, Lisfranc injuries represent a significant, albeit relatively uncommon, traumatic pathology affecting approximately 1 in 55,000 people annually, with a high propensity for long-term disability if not accurately diagnosed and treated. Midfoot arthritis, often post-traumatic or associated with inflammatory conditions, is a prevalent cause of chronic foot pain, necessitating surgical intervention in advanced stages. Understanding the nuances of dorsal surgical exposures is fundamental for any orthopedic surgeon treating the foot and ankle.
Surgical Anatomy & Biomechanics
The middle part of the foot is a remarkably stable and complex region, crucial for load transfer, arch support, and adaptive pronation/supination during gait. Mastery of dorsal approaches demands an intimate understanding of its bony architecture, ligamentous stabilizers, musculotendinous units, and neurovascular pathways.
Bony Anatomy
The midfoot comprises seven bones: the navicular, cuboid, and the three cuneiforms (medial, intermediate, lateral), which articulate with each other and the bases of the first through fifth metatarsals.
*
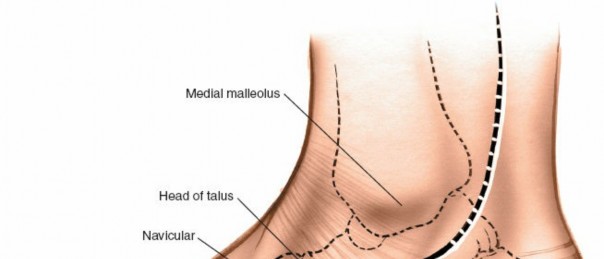
Navicular:
A boat-shaped bone articulating with the talar head proximally (talonavicular joint), the three cuneiforms distally, and the cuboid laterally. Its medial prominence, the tuberosity, is a key insertion site for the tibialis posterior tendon.
*
Cuneiforms:
Three wedge-shaped bones.
*
Medial Cuneiform:
The largest, articulating with the navicular proximally, intermediate cuneiform laterally, and the first and second metatarsals distally. It receives insertions from the tibialis anterior and peroneus longus.
*
Intermediate Cuneiform:
The smallest, articulating with the navicular, medial and lateral cuneiforms, and the second metatarsal.
*
Lateral Cuneiform:
Articulates with the navicular, intermediate cuneiform, cuboid, and the second, third, and fourth metatarsals.
*
Cuboid:
Roughly cuboidal, articulating with the calcaneus proximally (calcaneocuboid joint), lateral cuneiform and navicular medially, and the fourth and fifth metatarsals distally. The peroneus longus tendon grooves its plantar surface.
*
Metatarsal Bases:
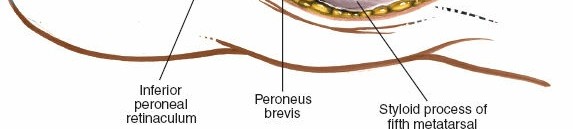
The proximal ends of the metatarsals articulate with the cuneiforms (1st, 2nd, 3rd) and cuboid (4th, 5th), forming the tarsometatarsal joints. The base of the fifth metatarsal has a prominent styloid process, an insertion point for the peroneus brevis.

Joint Architecture & Ligamentous Stability
The midfoot joints are primarily synovial joints with limited motion, contributing significantly to the stability of the longitudinal and transverse arches.
*
Talonavicular (TN) Joint:
A ball-and-socket joint allowing significant motion, especially in pronation and supination, acting as a critical component of the transverse tarsal joint.
*
Calcaneocuboid (CC) Joint:
A saddle-shaped joint, less mobile than the TN, but important for midfoot flexibility.
*
Tarsometatarsal (TMT) Joints (Lisfranc Joint Complex):
The articulation between the tarsals (cuneiforms and cuboid) and the metatarsal bases. The second metatarsal base is recessed between the medial and lateral cuneiforms, forming a "keystone" that enhances stability. The Lisfranc ligament, a strong plantar ligament connecting the medial cuneiform to the base of the second metatarsal, is the most crucial stabilizer of the Lisfranc complex. Dorsal ligaments are generally thinner and weaker than their plantar counterparts, which explains the propensity for dorsal displacement in Lisfranc injuries.
* Intercuneiform, cuneocuboid, and intermetatarsal ligaments further reinforce these articulations.

Musculotendinous Structures
The dorsal aspect of the midfoot is crossed by extrinsic extensor tendons, while several powerful intrinsic muscles insert into its bony elements.
*
Extensor Hallucis Longus (EHL):
Lies medially, extending the great toe.
*
Extensor Digitorum Longus (EDL):
Comprises four slips, extending the lesser toes.
*
Peroneus Tertius:
Often present as a slip of the EDL, inserting into the base of the fifth metatarsal, contributing to dorsiflexion and eversion.
*
Tibialis Anterior:
Inserts into the medial and inferior surfaces of the medial cuneiform and the base of the first metatarsal. Primary dorsiflexor and invertor.
*
Peroneus Longus:
Inserts into the lateral side of the medial cuneiform and the base of the first metatarsal (plantar aspect). Primary everter and plantarflexor of the first ray.
*
Peroneus Brevis:
Inserts into the base of the lateral side of the fifth metatarsal. Primary everter.
*
Tibialis Posterior:
Inserts into the tuberosity of the navicular bone, the inferior surface of the medial cuneiform, the intermediate cuneiform, and the bases of the second, third, and fourth metatarsals. Primary invertor and arch supporter.
The seed content correctly identifies these four powerful muscles (tibialis anterior, peroneus longus, peroneus brevis, tibialis posterior) as critical for controlling foot inversion and eversion, and their insertions are frequent targets for surgical procedures in the midfoot.

Neurovascular Structures
Precise identification and protection of neurovascular structures are paramount during dorsal midfoot approaches.
*
Arteries:
The
dorsalis pedis artery
, a continuation of the anterior tibial artery, runs distally over the talonavicular and cuneonavicular joints, typically between the EHL and the first slip of the EDL. It gives rise to the arcuate artery, which forms the dorsal metatarsal arteries.
*
Veins:
The
great saphenous vein
and its tributaries are often encountered medially. The dorsal venous arch collects blood from the foot and drains into the saphenous veins.
*
Nerves:
*
Deep Peroneal Nerve:
Accompanies the dorsalis pedis artery. It provides motor innervation to the extensor digitorum brevis and sensory innervation to the first dorsal web space. It is highly susceptible to iatrogenic injury during central dorsal approaches.
*
Superficial Peroneal Nerve:
Divides into medial dorsal cutaneous and intermediate dorsal cutaneous branches, supplying sensation to the majority of the dorsal foot. These branches are superficial and highly vulnerable during skin incision and subcutaneous dissection, especially laterally.
*
Saphenous Nerve:
A branch of the femoral nerve, provides sensory innervation to the medial aspect of the foot and ankle, often encountered during medial dorsal incisions.
Biomechanics
The midfoot acts as a crucial link in the kinetic chain, facilitating the transition from a mobile adaptor during pronation to a rigid lever arm during supination. The arches (longitudinal and transverse) are maintained by a combination of bony geometry, strong ligaments (especially plantar), and muscular forces. Dorsal approaches can disrupt these stabilizers, and reconstruction must respect the foot's biomechanical requirements. Malalignment or instability in the midfoot can significantly impair gait and lead to painful arthritis. The "keystone" effect of the second metatarsal base locked into the cuneiforms is essential for transverse arch stability, particularly at the Lisfranc joint.
Indications & Contraindications
Dorsal approaches to the midfoot are indicated for a spectrum of pathologies, primarily traumatic, degenerative, or related to deformity.
Indications for Dorsal Midfoot Approaches
-
Traumatic Injuries:
- Lisfranc Fracture-Dislocations: The most common indication. Requires anatomical reduction and stable internal fixation (ORIF) or primary arthrodesis for unstable purely ligamentous injuries or comminuted patterns. Dorsal incisions allow direct visualization and reduction of TMT joints.
- Navicular Fractures: Especially dorsal chip fractures, body fractures, or avulsion injuries where direct reduction and fixation are required.
- Cuneiform Fractures: Displaced or unstable fractures.
- Cuboid Fractures: Less commonly approached dorsally unless associated with other midfoot trauma.
- Talonavicular Joint Dislocation/Subluxation: Often part of a more complex midfoot injury.
-
Degenerative Conditions:
- Midfoot Arthrodesis: For painful, end-stage osteoarthritis (post-traumatic, inflammatory, or primary). Common targets include TN, NC, IC, or TMT joints. Dorsal approaches facilitate joint preparation, deformity correction, and hardware placement.
- Rheumatoid Arthritis: Correction of deformities and fusions for pain relief and stability.
-
Deformity Correction:
- Dorsal Exostosis (Tarsal Boss): Painful impingement or shoe wear irritation. Excision is performed directly via a dorsal approach.
- Accessory Navicular Syndrome: Symptomatic accessory navicular bone leading to posterior tibialis dysfunction. Excision of the accessory bone or Kidner procedure (excision with re-routing/re-attachment of tibialis posterior tendon) often involves a dorsomedial incision.
- Adult Acquired Flatfoot Deformity: Medial column stabilization and fusions (e.g., TN fusion, NC fusion) as part of a comprehensive reconstruction.
- Cavovarus Foot Deformity: Dorsal opening wedge osteotomies of the cuneiforms or cuboid, or fusions, to correct apex-dorsal deformity.
-
Tendon Pathology:
- Tibialis Anterior Tendon Repair/Transfer: For rupture or correction of muscle imbalance.
- Extensor Tendon Lengthening/Transfer: In cases of toe contractures or foot drop.
-
Other:
- Biopsy of dorsal midfoot lesions (tumors, infections).
- Debridement of chronic osteomyelitis.
Contraindications for Dorsal Midfoot Approaches
-
Absolute Contraindications:
- Acute Infection: Active cellulitis or osteomyelitis at the surgical site without prior debridement.
- Severe Peripheral Vascular Disease (PVD): Compromised circulation leading to poor wound healing potential.
- Uncontrolled Diabetes: Significantly increases risks of infection, nonunion, and wound complications.
-
Relative Contraindications:
- Poor Soft Tissue Envelope: Extensive scarring, thin skin, or open wounds that preclude safe dorsal incision and closure.
- Profound Neuropathy: Increases risk of delayed wound healing, unrecognized pressure points, and Charcot neuroarthropathy.
- Severe Edema: Optimization of soft tissue status pre-operatively is crucial.
- Extensive Plantar Pathology: If the primary pathology is exclusively plantar and cannot be addressed dorsally, alternative approaches are necessary.
Operative vs. Non-Operative Indications
The decision to proceed with surgical intervention via a dorsal midfoot approach is typically based on the severity of the condition, patient symptoms, failure of conservative management, and the specific pathology.
| Condition | Operative Indication | Non-Operative Indication ## Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is paramount for optimal outcomes in dorsal midfoot surgery, considering the critical neurovascular structures and complex biomechanics.
Pre-operative Planning
-
Clinical Assessment:
- History: Detailed account of pain characteristics (location, character, aggravating/alleviating factors), duration, previous injuries, neurological symptoms (numbness, weakness), functional limitations, and impact on activities of daily living.
-
Physical Examination:
- Inspection: Assessment for swelling, erythema, deformities (e.g., pes planus, pes cavus, dorsal bossing), skin integrity, and callosities.
- Palpation: Localize tenderness over specific joints or bony prominences (e.g., TN joint, Lisfranc ligament, dorsal midfoot exostosis). Assess pulses (dorsalis pedis, posterior tibial) and capillary refill.
- Range of Motion: Assess passive and active range of motion of the ankle, subtalar, and midfoot joints. Evaluate for pain with specific movements.
- Neurological Examination: Sensation to light touch and sharp/dull discrimination in the distribution of the deep and superficial peroneal nerves, and saphenous nerve. Motor strength of key ankle and foot muscles.
- Stability Assessment: For Lisfranc injuries, assess for gross instability, "gap" sign with stressing, and pain.
- Deformity Analysis: Evaluate hindfoot and forefoot alignment relative to the midfoot. For flatfoot, assess hindfoot valgus, forefoot abduction, and heel rise test. For cavovarus, assess hindfoot varus, forefoot adduction/supination, and Coleman block test.
-
Imaging Studies:
- Weight-Bearing Plain Radiographs: Essential. AP, lateral, and oblique views are standard. For Lisfranc injuries, stress views (AP and lateral with abduction/pronation) are crucial to identify subtle instability. Evaluate for midfoot arthritis (joint space narrowing, osteophytes), fractures, dislocations, or bony deformities.
- Computed Tomography (CT) Scan: The gold standard for evaluating bony anatomy, fracture patterns, comminution, intra-articular involvement, and subtle displacement. Indispensable for pre-operative planning of complex midfoot fractures or arthrodeses.
- Magnetic Resonance Imaging (MRI): Useful for assessing soft tissue injuries (ligamentous tears, tendon pathology, cartilage), bone edema, stress fractures, or occult lesions. Less critical for primary bony trauma unless soft tissue involvement is suspected.
- Bone Scan: May be used to identify areas of increased metabolic activity, useful in differentiating painful nonunion from pseudoarthrosis or infection.
-
Surgical Planning:
- Incision Placement: Precisely map out planned incisions, considering access to the pathology, avoidance of neurovascular structures, skin tension lines, and potential for future skin grafts. Dual incisions or modified single incisions may be necessary for complex injuries.
- Hardware Selection: Pre-operative templating based on CT scans helps select appropriate plates, screws, staples, or external fixators. Consideration of low-profile hardware for dorsal placement to minimize prominence.
- Surgical Sequence: Plan the order of steps: debridement, reduction strategy (direct vs. indirect), temporary fixation (K-wires), definitive fixation, bone grafting (if fusion).
- Patient Optimization: Ensure adequate nutritional status, glycemic control in diabetics, smoking cessation, and cessation of antiplatelet/anticoagulant medications as per protocol.
Patient Positioning
-
Position:
The patient is typically placed in the
supine position
on the operating table.
- A small bump or rolled towel may be placed under the ipsilateral hip to internally rotate the limb slightly, improving access to the medial aspect of the foot without excessive surgeon contortion.
- Tourniquet: A pneumatic tourniquet is applied to the proximal thigh to achieve a bloodless field, which is critical for identifying delicate neurovascular structures and achieving precise bony reduction.
- Image Intensifier (Fluoroscopy): The C-arm must be positioned to allow unrestricted access for AP, lateral, and oblique views of the midfoot. This typically involves positioning the C-arm from the opposite side of the table or at the foot of the bed.
- Draping: A sterile preparation and draping technique should be used, encompassing the entire foot and ankle, extending up to the mid-calf. This allows for manipulation of the foot and ankle to facilitate reduction and provides sterile access for potential bone graft harvest if needed.
- Preparation: The entire lower extremity is prepped with an antiseptic solution according to institutional protocol.
Detailed Surgical Approach / Technique
Dorsal approaches to the midfoot require a meticulous, layered dissection to minimize iatrogenic injury and achieve optimal exposure. The specific incision will vary based on the targeted anatomy and pathology.
General Principles of Dorsal Midfoot Dissection
- Skin Incision: Longitudinal incisions are preferred to minimize the risk of wound dehiscence and facilitate extension if necessary. Avoid transverse incisions over joints.
- Subcutaneous Dissection: Careful, sharp dissection through the skin and subcutaneous fat. Identify and protect the superficial peroneal nerve branches (medial dorsal cutaneous, intermediate dorsal cutaneous) which are highly variable and prone to injury. The great saphenous vein and saphenous nerve are protected medially.
- Deep Fascia: Incise the deep fascia longitudinally.
-
Neurovascular Bundle (Central Dorsal):
The deep peroneal nerve and dorsalis pedis artery typically run within the internervous plane between the extensor hallucis longus (EHL) and the first slip of the extensor digitorum longus (EDL). These structures must be identified, gently mobilized, and retracted. The deep peroneal nerve is usually lateral to the artery.
 - Extensor Tendons: The EHL, EDL, and peroneus tertius tendons can be retracted medially or laterally to expose the underlying joint capsules and bony structures. If extensive exposure is needed, a release of the extensor retinaculum may be required.
- Capsular Incision: Incise the joint capsule longitudinally to expose the articular surfaces. Preserve capsular attachments as much as possible for later repair.
Specific Dorsal Approaches
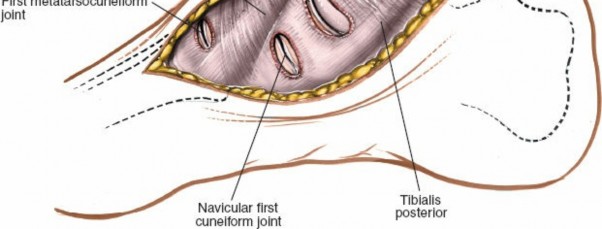
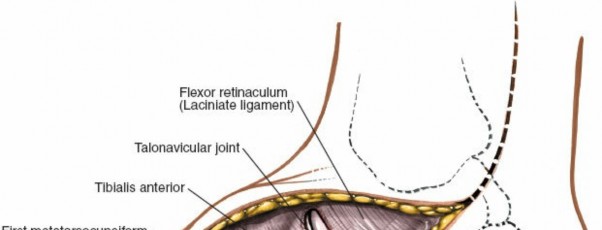
1. Medial Dorsal Approach (First Ray, Medial Cuneiform, Navicular, TN Joint)
-
Incision:
A longitudinal incision, 5-8 cm in length, centered over the medial cuneiform and extending proximally towards the navicular or distally towards the first metatarsal base. A slight curvilinear course may be used to enhance skin flap viability.
 -
Dissection:
- Skin and subcutaneous tissues are carefully incised. The saphenous nerve and great saphenous vein lie superficially and medially; they must be identified and protected, typically by retracting them inferiorly and medially.
- The deep fascia is opened. The tibialis anterior tendon is the most prominent structure. It can be retracted medially or laterally, depending on the precise area of interest.
- The EHL tendon is lateral to the tibialis anterior and can be retracted laterally.
- Exposure can be gained to the medial cuneiform-navicular (NC), navicular-talar (TN), and first tarsometatarsal (TMT) joints.
- Indications: Medial column arthrodesis (NC, TN, 1st TMT), excision of accessory navicular, fixation of medial cuneiform or navicular fractures, tibialis anterior tendon transfers.
2. Central Dorsal Approach (Cuneiforms, Lisfranc Joint Complex, 2nd & 3rd TMT Joints)
-
Incision:
A longitudinal incision, 6-10 cm, centered over the second metatarsal base and extending proximally over the intermediate and medial cuneiforms.
 -
Dissection:
- After incising skin and subcutaneous tissue, branches of the superficial peroneal nerve must be meticulously identified and protected, often by careful blunt dissection and retraction.
- The deep peroneal nerve and dorsalis pedis artery are the most critical structures. They typically lie deep to the extensor retinaculum, between the EHL and EDL tendons (specifically the first slip). These structures are mobilized together and gently retracted, usually medially, to protect them.
- The extensor retinaculum may need to be incised longitudinally to gain full exposure.
- The EHL and EDL tendons are retracted. This approach provides direct access to the intermediate cuneiform, lateral cuneiform, and the articulations of the second and third metatarsal bases with the cuneiforms.
- Indications: Lisfranc fracture-dislocations (ORIF or primary arthrodesis), central column fusions, cuneiform fractures. Often, two dorsal incisions (medial and central or central and lateral) are used for complex Lisfranc injuries to ensure comprehensive reduction and fixation.
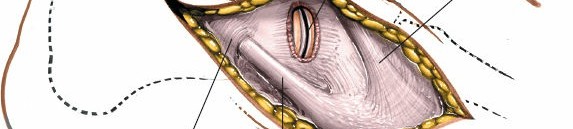
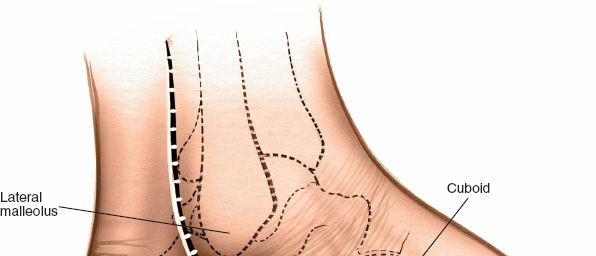
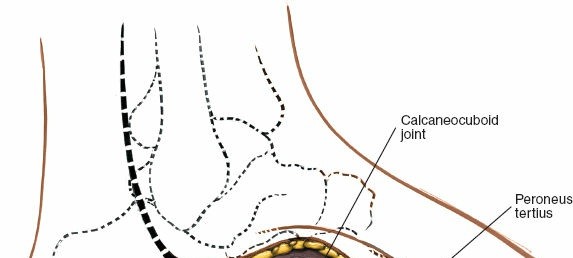
3. Lateral Dorsal Approach (Cuboid, 4th & 5th TMT Joints, CC Joint)
-
Incision:
A longitudinal incision, 5-8 cm, centered over the cuboid and extending distally over the bases of the fourth and fifth metatarsals.
 -
Dissection:
- Careful incision through the skin and subcutaneous fat is critical due to the presence of multiple branches of the superficial peroneal nerve . These branches are highly variable and should be identified, mobilized, and protected, typically by retraction.
- The EDL tendons (especially the lateral slips) and peroneus tertius are retracted medially. The peroneus brevis and longus tendons lie more laterally and inferiorly (plantar side of the cuboid) and are generally not directly in the field of a purely dorsal approach but should be considered if the incision extends more laterally or distally.
- This approach provides access to the cuboid-navicular, cuboid-lateral cuneiform, calcaneocuboid (CC), and fourth and fifth TMT joints.
- Indications: Cuboid fractures, lateral column arthrodesis, fixation of 4th/5th TMT injuries.
Reduction and Fixation Techniques
- Debridement: Remove hematoma, soft tissue interposition, and comminuted fragments that are non-articular.
-
Reduction:
- Achieve anatomical reduction of fractures or dislocations under direct visualization and fluoroscopic guidance.
- Traction and manipulation (often with an assistant) are applied.
- Small periosteal elevators or K-wires can be used as joysticks to maneuver fragments.
-
Temporary K-wire fixation is crucial to maintain reduction.

-
Fixation:
- Fractures/Dislocations: Utilize low-profile dorsal plates and screws, lag screws (e.g., across the TMT joints for Lisfranc injuries, specifically medial cuneiform to 2nd metatarsal base for the Lisfranc ligament), or absorbable screws. The goal is rigid internal fixation maintaining anatomical alignment. For Lisfranc injuries, current trends often favor primary arthrodesis, particularly for purely ligamentous injuries or extensively comminuted patterns, which involves joint preparation and fixation as described for fusions.
-
Arthrodesis:
- Prepare joint surfaces by excising articular cartilage down to bleeding subchondral bone.
- Correct any existing deformity.
- Apply compression across the fusion site using screws, staples, or low-profile plates.
- Bone graft (autograft from iliac crest or distal tibia, allograft, or demineralized bone matrix) is often packed into the prepared joint space to enhance fusion rates.
-
Hardware selection depends on the bone quality and desired stability.

-
Final Assessment:
Confirm anatomical reduction and stable fixation with fluoroscopy in AP, lateral, and oblique views. Assess range of motion of adjacent joints if not part of the fusion.
 -
Closure:
- Irrigate the wound thoroughly.
- Close the deep fascia loosely if possible.
- Address the extensor retinaculum; careful closure can help stabilize tendons, but avoid overtightening which could lead to nerve compression or tendon impingement.
- Close subcutaneous tissues and skin in layers. Avoid excessive tension on skin edges.
- Apply a sterile dressing and a well-padded splint or cast in a neutral position.
Complications & Management
Complications following dorsal midfoot surgery, while manageable, can significantly impact patient outcomes. Vigilant post-operative monitoring and timely intervention are crucial.
Common Complications and Management Strategies
| Complication | Incidence (Approx.) | Salvage Strategies
Clinical & Radiographic Imaging
You Might Also Like