Charcot Foot (Neuro-osteoarthropathy): Epidemiology, Pathogenesis, Anatomy & Biomechanics
Key Takeaway
Charcot neuro-osteoarthropathy, or Charcot foot, is a severe, progressive condition where peripheral neuropathy, primarily from diabetes, leads to joint dislocation, bone fractures, and foot collapse. It results from repetitive microtrauma to a denervated foot (neurotraumatic theory) combined with increased blood flow and osteolysis (neurovascular theory), exacerbated by inflammation.
Introduction & Epidemiology
Charcot neuro-osteoarthropathy, commonly referred to as Charcot foot, is a progressive, debilitating condition characterized by joint dislocation, bone fractures, and profound architectural collapse of the foot and ankle, often in the absence of significant trauma. It represents a severe manifestation of peripheral neuropathy, leading to a loss of protective sensation and proprioception, coupled with altered vascular physiology. While historically associated with tabes dorsalis and leprosy, diabetes mellitus now stands as the predominant etiology, accounting for over 80% of cases. Other neuropathic conditions contributing to Charcot foot include alcoholism, syringomyelia, spinal cord injury, congenital insensitivity to pain, and peripheral nerve injury.
The pathogenesis involves a complex interplay of neurotraumatic and neurovascular theories. The neurotraumatic theory posits that repetitive microtrauma to a denervated foot, unperceived by the patient due to sensory neuropathy, leads to progressive bone and joint destruction. The absence of protective sensation permits continued weight-bearing on an unstable, damaged structure. The neurovascular theory suggests that autonomic neuropathy causes increased blood flow to the affected limb, leading to osteopenia, increased osteoclastic activity, and bone resorption, which predisposes to microfractures and subsequent collapse. Recent understanding emphasizes a combined mechanism, where inflammatory mediators triggered by microtrauma are exacerbated by a hyperemic state, leading to an aggressive osteolytic process.
Epidemiologically, the lifetime risk of developing Charcot foot in diabetic patients ranges from 0.08% to 7.5%, with an annual incidence of 0.3% to 1.0%. It typically affects individuals in their fifth to seventh decades of life, with an average duration of diabetes preceding diagnosis often exceeding 10 years. Bilateral involvement occurs in approximately 10-20% of cases. Early recognition is paramount as delayed diagnosis significantly increases the risk of severe deformity, ulceration, osteomyelitis, and ultimately, limb amputation. The Eichenholtz classification system, though descriptive, stages the disease process:
*
Stage 0 (Prodromal):
Clinical signs of inflammation (swelling, warmth, erythema) but without radiographic changes.
*
Stage I (Developmental/Acute):
Acute fragmentation and joint dislocation with radiographic evidence of osseous destruction.
*
Stage II (Coalescence):
Decreased inflammation, absorption of fine debris, early callus formation and bone sclerosis.
*
Stage III (Reconstruction/Resolution):
Diminished inflammation, remodeling, and consolidation of fracture fragments, often resulting in a stable but deformed foot.
The Sanders classification provides a useful anatomical localization of the deformity:
*
Type I:
Isolated metatarsophalangeal (MTP) joint involvement.
*
Type II:
Tarsometatarsal (TMT) joints.
*
Type III:
Naviculocuneiform and talonavicular joints.
*
Type IV:
Talonavicular, subtalar, and ankle joints.
*
Type V:
Calcaneocuboid joint.
Surgical Anatomy & Biomechanics
A thorough understanding of foot and ankle surgical anatomy and biomechanics is critical for the effective management of Charcot neuro-osteoarthropathy. The foot is a complex structure designed for stability during static stance and flexibility during gait, achieved through the intricate interaction of 26 bones, 33 joints, over 100 ligaments, and numerous tendons. Neuropathy disrupts this delicate balance, rendering the intrinsic and extrinsic musculature ineffective and proprioception unreliable.
Key anatomical considerations include:
*
Hindfoot:
Comprising the talus and calcaneus. The subtalar joint (STJ) allows for inversion and eversion, critical for adapting to uneven surfaces. The ankle joint (tibiotalar) is a hinge joint providing dorsiflexion and plantarflexion. Loss of STJ stability often leads to severe valgus or varus hindfoot collapse.
*
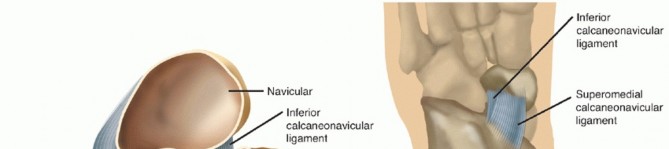
Midfoot:
Consisting of the navicular, cuboid, and three cuneiforms, articulating with the hindfoot and forefoot. The TMT joints are crucial for the integrity of the longitudinal arch. Midfoot collapse, often termed a "rocker-bottom" deformity (Sanders Type III, IV), occurs with disruption of the naviculocuneiform and TMT joints, leading to a plantar prominence that is highly prone to ulceration.
*
Forefoot:
Includes the metatarsals and phalanges. Forefoot involvement (Sanders Type I, II) typically manifests as MTP joint dislocations or TMT joint subluxations.
Biomechanical principles in the neuropathic foot are profoundly altered:
*
Weight-Bearing Axis:
In a healthy foot, weight is distributed through the calcaneus, the metatarsal heads, and the phalanges, maintaining the medial and lateral longitudinal arches. In Charcot foot, disruption of these arches leads to abnormal plantar pressure distribution, particularly prominent in the midfoot with a rocker-bottom deformity.
*
Ligamentous Instability:
Neuropathy and the inflammatory cascade lead to ligamentous laxity and destruction, contributing significantly to joint instability and eventual osseous collapse. The plantar fascia and spring ligament, crucial for medial arch support, are often compromised.
*
Muscle Imbalance:
Intrinsic muscle atrophy and extrinsic muscle weakness or imbalance contribute to contractures and abnormal loading patterns, further propagating deformity.
*
Autonomic Neuropathy:
Vasodilation and increased bone turnover secondary to sympathetic denervation result in regional osteopenia, making bones more susceptible to fracture and fragmentation with normal physiological loads. This hyperemic state also exacerbates the inflammatory response.
Surgical intervention aims to restore a plantigrade, stable foot through meticulous realignment of the weight-bearing axis, arthrodesis of unstable joints, and reconstruction of bone defects. Understanding the specific anatomical structures involved in the deformity (e.g., TMT joint disruption in a midfoot collapse) guides surgical planning for appropriate osteotomies and fixation strategies. Protection of neurovascular structures, particularly the posterior tibial neurovascular bundle, anterior tibial neurovascular bundle, and superficial peroneal nerve branches, is paramount during all approaches.
Indications & Contraindications
The decision-making process for surgical intervention in Charcot neuro-osteoarthropathy is complex, balancing the potential benefits of deformity correction and limb salvage against the significant risks in this often medically compromised patient population. Non-operative management, primarily total contact casting (TCC), is the cornerstone of acute Charcot management. Surgery is generally reserved for situations where non-operative measures have failed or are predicted to fail, or when specific limb-threatening conditions exist.
Indications for Operative Management:
-
Acute Unstable Deformity:
- Eichenholtz Stage 0-I: Impending ulceration due to acute instability or severe displacement without chronic ulceration.
- Irreducible dislocations/fractures: Where realignment cannot be achieved with casting.
- Gross instability: Despite appropriate immobilization, progressive collapse or instability is noted.
-
Chronic Stable Deformity (Eichenholtz Stage III):
- Recurrent Plantar Ulceration: Due to a non-plantigrade foot or bony prominences (e.g., rocker-bottom deformity) that are refractory to conservative measures (offloading, custom orthotics, accommodative footwear).
- Unbraceable Deformity: Deformities so severe that custom bracing or footwear cannot accommodate or protect the foot, leading to recurrent skin breakdown.
- Progressive Deformity: Despite offloading, the deformity continues to worsen.
- Osteomyelitis: Associated with an ulceration that requires debridement, ostectomy, and stabilization for limb salvage.
- Neuroarthropathic Ankle and Hindfoot: Severe instability or deformity involving the tibiotalar or subtalar joints that cannot be managed non-operatively.
Contraindications for Operative Management:
- Acute Active Infection (Uncontrolled): Systemic signs of sepsis, uncontrolled osteomyelitis. Source control (debridement, antibiotics) must precede definitive arthrodesis.
- Severe Peripheral Arterial Disease (PAD): Unreconstructable vascular supply (ABI <0.4, TcPO2 <30 mmHg) in the operative area. Revascularization must precede elective Charcot reconstruction.
- Uncontrolled Systemic Conditions: Poor glycemic control (HbA1c >8-9%), severe cardiac disease, end-stage renal disease, or other comorbidities that significantly elevate surgical and anesthetic risks.
- Non-Compliance: Patients unable or unwilling to adhere to strict non-weight-bearing protocols and long-term follow-up.
- Severe Bone Loss/Quality: Insufficient host bone stock to achieve stable fixation, leading to a high likelihood of hardware failure or nonunion.
- Untreated Edema: Significant peripheral edema must be managed preoperatively to minimize wound complications.
- Active Eichenholtz Stage I: Unless there's impending ulceration or severe instability. Otherwise, initial TCC is preferred until the foot enters the coalescence stage (Eichenholtz II).
Operative vs. Non-Operative Indications
| Feature | Operative Indications | Non-Operative Indications |
|
Primary Goal
| Restore stable, functional, plantigrade foot to prevent recurrent ulceration and potential amputation. | Immobilize the foot to achieve clinical stability and minimize further joint destruction; prevent skin breakdown. |
|
Disease Stage
| Eichenholtz I, II, or III with significant instability or refractory complications. |
|
Foot Character | Neuropathic foot with acute inflammation, edema, deformity, and potential impending ulceration or severe instability. Radiographs show osseous fragmentation or dislocation. |
|
Key Issues
| Irreducible bony deformities, instability, persistent ulceration despite aggressive offloading, severe instability rendering orthotics ineffective, or progressive deformity. | |
|
Primary Indication | Unstable Charcot deformity (Eichenholtz stage 0-I with impending ulceration/amputation), Chronic stable deformity with recurrent ulceration/infection, unbraceable deformity, severe pain. | Acute Charcot (Eichenholtz stage 0-I) without impending ulceration or severe instability, stable chronic deformity with well-controlled symptoms via bracing/orthotics, medically unstable for surgery, severe comorbidities. |
|
Potential Risks | Surgical site infection (SSI), osteomyelitis, hardware failure, nonunion, recurrent deformity, amputation, neurological deficits, persistent pain. |
|
Likely Outcome | Significant improvement in foot architecture, reduction of ulceration risk, improved function, prevention of amputation. |
|
Key Objectives
| Restore a stable, plantigrade foot; achieve durable soft tissue coverage; preserve limb length; maximize functional mobility and quality of life. |
|
Anesthesia/Blood Mgmt.
| Spinal/regional with conscious sedation or general anesthesia. Consider local infiltrative blocks. Ensure adequate blood product availability (PRBCs, FFP, platelets) and blood-sparing techniques (tranexamic acid). |
|
Severity of Deformity
| Severe | Mild to None |
|
Severity of Comorbidities
| Mild-Moderate: Optimized to improve surgical candidacy. |
|
Vascular Status
| Adequate peripheral arterial flow to sustain healing and prevent complications. If diminished, potential for revascularization. |
|
Patient Adherence
| Expected to be highly compliant with post-operative instructions. |
|
Vascular Disease (PAD)
| Revascularization status allows for safe surgical intervention and healing. | Critical PAD, or poor revascularization potential. |
|
Vascular Assessment
| Full peripheral vascular assessment including bilateral ABI, PVR, and potentially duplex ultrasound or angiography. Adequate perfusion (e.g., TcPO2 >30mmHg) is essential. | Clinical assessment indicates adequate perfusion, or minor non-limb-threatening PAD that is being managed conservatively. |
|
Medication Considerations
| Optimize blood sugar control. Consider factors affecting wound healing (ePatient comorbidities, nutritional status). |
|
Medical Stability
| Medically stable; controlled comorbidities. |
|
Infection Status
| No active infection. If infection exists, it should be surgically debrided and optimized with antibiotics prior to bone reconstruction. | Current management successfully controlling local infection; no clear indication for further surgical treatment of infection. |
|
Medical History
| Diabetes with neuropathy, possible history of Charcot or previous foot reconstruction. No major contraindications. |
|
Financial Resources
| Sufficient for recovery and long-term care. | Insufficient financial resources for required management or potential long-term care. |
|
Expected Compliance
| High |
|
Complications
| Wound dehiscence, infection (SSI, osteomyelitis), hardware failure, nonunion, recurrent deformity, amputation. |
|
Additional Factors
| Prior surgical history, presence of deformity/Charcot arthropathy in the contralateral limb, social support system, home environment, patient mobility, and functional status. |
|
Contralateral Foot Involvement
| No history of Charcot or active acute disease. Potentially prior reconstruction. |
|
Contralateral Foot Involvement
| Char Active Charcot arthropathy or ulceration/infection necessitating simultaneous or staged contralateral limb surgery. |
|
Imaging Guidance
| Preoperative CT and/or 3D reconstruction for complex deformities. |
|
Current Treatment
| Failed non-operative treatment, or acute complications demanding surgery. | Initial management is conservative, aiming to reduce inflammation and stabilize the foot. Failure to achieve stability or to prevent ulceration after appropriate conservative management may be an indication for surgery. |
Pre-Operative Planning & Patient Positioning
Successful Charcot reconstruction necessitates meticulous preoperative planning and precise intraoperative patient positioning. These steps are fundamental to achieving the reconstructive goals of creating a stable, plantigrade foot, amenable to bracing, and free from ulceration.
Pre-Operative Planning:
-
Patient Optimization:
- Glycemic Control: Strict perioperative blood glucose management is critical (target HbA1c < 8% and fingerstick glucose 80-180 mg/dL). This reduces infection risk and promotes wound healing.
- Nutritional Status: Optimize protein, albumin, and vitamin levels. Poor nutrition significantly impairs wound healing.
- Vascular Assessment: Comprehensive non-invasive and potentially invasive vascular studies (angiography) are mandatory to ensure adequate perfusion for wound healing. Revascularization procedures should precede orthopedic reconstruction in cases of significant peripheral arterial disease (ABI <0.7, TcPO2 <30 mmHg, significant claudication/rest pain).
- Infection Screening: Clinical suspicion (fever, erythema, purulent discharge, elevated inflammatory markers) warrants aspiration/biopsy and broad-spectrum antibiotics. Osteomyelitis must be surgically debrided and treated with a prolonged antibiotic course. Definitive reconstruction may be staged after infection eradication.
- Medical & Anesthesia Clearance: Comprehensive cardiac, renal, and pulmonary evaluations are essential given the common comorbidities. Neuropathy may mask angina.
- Smoking Cessation: Patients must cease smoking at least 6-8 weeks prior to surgery.
-
Imaging & Deformity Analysis:
- Weight-bearing Radiographs: Essential for evaluating the extent of deformity, fragmentation, and alignment in the sagittal, coronal, and axial planes. Obtain bilateral views for comparison.
- CT Scan with 3D Reconstruction: Indispensable for complex deformities, providing detailed visualization of osseous architecture, joint destruction, bone loss, and identification of specific fracture patterns or malunions. This guides osteotomy planning and implant selection.
- MRI: Useful for assessing soft tissue inflammation, identifying osteomyelitis, abscesses, or sinus tracts, and delineating areas of active Charcot fragmentation versus stable deformity.
- Bone Scan (Tc-99m): Differentiates active Charcot (diffuse uptake) from osteomyelitis (focal uptake, often with WBC scan correlation). Indium-111 WBC scan can further increase specificity for infection.
-
Surgical Strategy & Implant Selection:
- Deformity Correction Plan: Detailed plan outlining necessary osteotomies (e.g., medial closing wedge for valgus, lateral closing wedge for varus, sagittal plane for rocker-bottom), bone resection, and soft tissue releases (e.g., Achilles lengthening for equinus contracture). Aim for a plantigrade, stable foot that fits into a custom brace.
-
Implant Selection (Superconstruct Principle):
Charcot feet require robust, high-strength fixation.
- Intramedullary (IM) Nailing: Preferred for hindfoot and ankle arthrodesis, offering superior biomechanical stability compared to plates alone. Can be used in combination with screws.
- Large Fragment Screws & Plates: Often used in the midfoot and forefoot. Low-profile plates are generally avoided. Larger, thicker plates (e.g., 3.5mm, 4.5mm) with locking screw capabilities are preferred. Consider multiple plates and screw trajectories.
- External Fixation (Circular/Hybrid): Useful for severe instability, gross infection, significant bone loss requiring bone transport, or compromised soft tissues. Offers modularity and adjustable compression. Can be combined with internal fixation (hybrid constructs).
- Arthrodesis Cages/Allografts: For substantial bone defects to maintain length and provide structural support.
- Bone Grafting: Autograft (iliac crest, calcaneus) or allograft (cancellous chips, structural) typically used to enhance fusion in arthrodesis sites.
-
Wound Management Plan: Pre-existing ulcerations should be debrided, cultured, and managed by a wound care team. Surgical incisions must be meticulously planned to avoid existing or impending ulcerations, often utilizing medial or lateral approaches rather than plantar.
Patient Positioning:
- Supine Position: Most common, allowing access to the medial and lateral aspects of the foot and ankle.
- Contralateral Hip Flexion: The contralateral hip may be flexed and abducted, allowing the surgical leg to rest on the table for easier access to the medial aspect of the foot or the Achilles tendon for lengthening.
- Image Intensifier (Fluoroscopy): Essential. Position the C-arm to obtain true AP, lateral, and oblique views of the foot and ankle without repositioning the patient.
- Thigh Tourniquet: Used for hemostasis; typically inflated to 250-300 mmHg depending on patient's blood pressure. Pre-exsanguination may be performed carefully or omitted depending on vascular status.
- Bony Prominence Padding: Meticulous padding of all pressure points is vital due to the patient's insensate skin and prolonged surgical times.
- Stabilizing Bump: A small bump or roll under the ipsilateral hip may facilitate internal rotation of the limb for improved access.
Detailed Surgical Approach / Technique
Charcot reconstruction is technically demanding, requiring precise execution of osteotomies, meticulous debridement, and robust internal or external fixation. The goal is to create a stable, plantigrade, braceable foot, free of ulceration, and with solid arthrodesis.
General Principles:
- Debridement and Osteotomy: Remove all necrotic bone, cartilage, and inflamed synovium. Perform necessary osteotomies to correct deformity and create healthy cancellous bone surfaces for fusion.
- Realignment: Restore anatomical alignment, particularly the weight-bearing axis, to prevent future plantar pressure points.
- Arthrodesis: Fuse involved joints to achieve stability. This often involves multiple joints (e.g., pan-talar, triple arthrodesis).
- Robust Fixation (Superconstructs): Employ strong, large-diameter implants, often in combination (plates, screws, IM nails, external fixators) to withstand the significant forces in a neuropathic limb.
- Soft Tissue Management: Carefully plan incisions to avoid plantar skin and areas of prior ulceration. Achieve tension-free wound closure. Consider local or free flaps for large defects.
- Equinus Correction: Address any equinus contracture (often with an Achilles lengthening or gastrocnemius recession) to reduce forefoot pressures and facilitate dorsiflexion.
Surgical Approaches & Step-by-Step Technique:
The specific approach varies based on the location and type of deformity (Sanders classification).
Midfoot Reconstruction (Rocker-Bottom Deformity - Sanders Type III, IV):
Often requires a combination of medial and lateral approaches.
-
Incision:
- Medial Approach: Longitudinal incision along the medial aspect of the foot, extending from the navicular to the first metatarsal base. Identify and protect the saphenous nerve and vein. Retract the tibialis anterior tendon dorsally and the tibialis posterior tendon plantarly.
- Lateral Approach: Longitudinal incision along the lateral aspect, often curvilinear, from the calcaneocuboid joint extending towards the cuboid-fifth metatarsal junction. Identify and protect the sural nerve. Retract the peroneus brevis and longus tendons.
-
Soft Tissue Dissection & Debridement:
- Subperiosteal dissection to expose the collapsed midfoot joints (TMT, naviculocuneiform, talonavicular, calcaneocuboid).
- Debride all fragmented bone, necrotic tissue, and unstable cartilage. This creates a cavity for deformity correction and bone grafting.
- Carefully excise any plantar callus or bursa associated with the rocker-bottom prominence, being cautious to avoid plantar skin perforations.
-
Deformity Correction & Osteotomies:
- Rocker-Bottom Correction: A large dorsal wedge osteotomy or resection arthrodesis is typically performed through the apex of the deformity (often at the naviculocuneiform or TMT joints). This may involve resecting a dorsal wedge of bone and shortening the dorsal aspect to allow reduction of the plantar prominence.
- Equinus Correction: If present, perform a percutaneous Achilles lengthening or gastrocnemius recession to achieve a neutral ankle dorsiflexion.
- Hindfoot Realignment: Address any associated hindfoot valgus or varus by manipulating the subtalar joint.
-
Reduction & Temporary Fixation:
- Manually reduce the deformity, aiming for a plantigrade foot with restored arches. The critical goal is a flat plantar surface, not necessarily anatomic reconstruction.
- Use multiple large K-wires (e.g., 2.0-2.5mm) to temporarily stabilize the corrected alignment. Ensure reduction of the plantar prominence.
-
Definitive Fixation (Superconstruct):
- Dorsal Plating: Often involves one or two dorsal locking plates (e.g., 3.5mm or 4.5mm) across the arthrodesis sites. Place plates to span multiple joints and bones, distributing stress.
- Medial/Lateral Plating: Supplemental plates can be applied medially or laterally to enhance stability, particularly for extensive fusions.
- Intramedullary Nailing (for Hindfoot Extension): If the fusion extends into the hindfoot (e.g., naviculocuneiform fusion extending to talonavicular or subtalar), a large hindfoot intramedullary nail can provide excellent primary stability. This typically extends from the calcaneus, through the talus, into the tibia.
- Large Fragment Screws: Use multiple 6.5mm or 7.0mm cannulated or solid screws strategically placed for compression and anti-rotation, spanning fusion sites.
- Bone Grafting: Pack autograft (from calcaneus or iliac crest) or allograft into all fusion sites to promote osteogenesis.
-
Wound Closure: Meticulous layered closure. Avoid tension. Consider a drain if significant dead space. Apply a bulky dressing and immediate splint or cast.
Ankle/Hindfoot Reconstruction (Sanders Type IV, V):
Often requires a combined approach for pan-talar or tibiotalocalcaneal (TTC) arthrodesis.
-
Incision:
- Lateral Transfibular Approach: Longitudinal incision centered over the distal fibula. Fibula is often resected to gain wide access to the ankle and subtalar joints. Identify and protect superficial peroneal nerve and sural nerve branches.
- Medial Approach: Longitudinal incision posterior to the tibia, curving around the medial malleolus. Identify and protect the posterior tibial neurovascular bundle.
- Posterior Approach: For extensive hindfoot fusion, a posterior approach can facilitate access to the subtalar and calcaneocuboid joints, and for Achilles lengthening.
-
Debridement & Osteotomies:
- Debride all unstable bone, cartilage, and synovium from the ankle (tibiotalar) and subtalar (talocalcaneal) joints.
- For TTC arthrodesis, the talus may be completely removed (talectomy) in severe cases, or extensively debrided.
- Correct equinus contracture with Achilles lengthening.
-
Reduction & Temporary Fixation:
- Reduce the foot into a neutral, plantigrade position. Ensure proper rotation and eliminate hindfoot valgus/varus.
- Temporarily stabilize with large K-wires.
-
Definitive Fixation:
- Intramedullary Nailing: The gold standard for TTC arthrodesis. A large diameter (e.g., 10-14mm) IM nail is inserted antegrade through the plantar aspect of the heel, up through the calcaneus, talus, and into the tibia. Multiple locking screws are used in the calcaneus and tibia to create a strong construct.
- Plates & Screws: In cases where IM nailing is not feasible or as supplemental fixation, strong plates (e.g., pre-contoured locking plates) and large fragment screws can be used. Lateral plates after fibular excision, or medial plates.
- Bone Grafting: Pack fusion sites with autograft or allograft.
-
Wound Closure: Meticulous layered closure, attention to the subcutaneous tissue and skin.
Forefoot Reconstruction (Sanders Type I, II):
Typically less common and less severe than midfoot/hindfoot.
- Incision: Dorsal longitudinal incisions over the affected TMT or MTP joints. Care to protect dorsal nerves and tendons.
- Debridement & Correction: Resect prominent bony fragments. Reduce dislocations.
- Fixation: Small fragment locking plates (e.g., 2.7mm or 3.5mm) and/or large fragment screws. K-wires for temporary fixation. Arthrodesis of involved joints is common.
- Wound Closure: Standard layered closure.
External Fixation Considerations:
- Indications: Severe infection, extensive soft tissue defects, significant bone loss, or failed internal fixation.
- Technique: Utilize circular or hybrid external fixation frames (e.g., Ilizarov-type). Rings or half-pins are strategically placed, connected by rods or wires, allowing for gradual correction of deformity, compression across fusion sites, and stability. Can be used as a primary stabilization tool or as a temporary bridge to definitive internal fixation.
- Hybrid Constructs: Often internal fixation is combined with external fixation for maximal stability, especially in grossly unstable hindfoot fusions.
Complications & Management
Complications following Charcot foot reconstruction are frequent and can be severe, reflecting the complex pathology and patient comorbidities. A robust understanding of these potential issues and their management is essential for limb salvage.
| Complication | Incidence (approximate) | Management / Salvage Strategy |
|
Primary Goal
| Achieve stable, fused foot in a plantigrade position, promoting ambulation and preventing recurrent ulceration/infection. |
|
Contralateral Foot Involvement
| No history of prior Charcot or current acute involvement. |
|
Post-Op Care
| Adherence to a strict, prolonged period of non-weight-bearing (minimum 12-16 weeks) in a protective cast or boot, gradual rehabilitation, custom orthotics/shoes for life, regular follow-up for skin integrity and deformity assessment. | |
|
Severity of Comorbidities
| Mild to None. |
|
Severity of Deformity
| Moderate. |
|
Current Treatment
| Non-operative management with strict offloading. |
|
Current Treatment
| Non-operative management, usually involving strict offloading (e.g., total contact cast (TCC), walker boot, customized orthoses). |
|
Current Treatment
| Failed non-operative treatment with persistent ulceration or pain. |
|
Current Treatment
| Non-operative (e.g., TCC, custom orthotics). Patient might have a history of previous successful Charcot reconstruction on the other foot.
You Might Also Like