Comprehensive Lisfranc Injury Case Study: Clinical Examination & Advanced Diagnostics

Key Takeaway
Diagnosing a Lisfranc injury requires evaluating high-energy trauma, severe midfoot pain, and swelling. Key clinical signs are plantar ecchymosis ('footprint sign') and TMT joint tenderness. Radiographs may reveal metatarsal widening or a 'fleck sign.' CT scans are crucial for confirming subtle fractures, articular incongruity, and ligament disruption, guiding treatment.
Patient Presentation & History
We present the case of a 38-year-old male, a previously healthy, active construction worker, who sustained a high-energy mechanism of injury. He was involved in a motor vehicle collision as a restrained driver, during which his foot was forced into a fixed equinus position on the floorboard, leading to an axial load with simultaneous hyperplantarflexion and pronation forces applied to the midfoot. The patient reported immediate, excruciating pain in his right midfoot, inability to bear weight, and rapid onset of swelling. There was no gross open injury, but ecchymosis was noted shortly after the incident.
His past medical history was significant for controlled hypertension, managed with an ACE inhibitor. He was a non-smoker, socially consumed alcohol, and denied any history of previous foot or ankle injuries, neuropathy, or systemic inflammatory conditions. Given the high-energy nature of the trauma, a comprehensive trauma workup was initiated to rule out other associated injuries.
Clinical Examination
Upon initial assessment in the emergency department, the patient was hemodynamically stable.
The physical examination of the right foot revealed:
- Inspection: Marked diffuse swelling and ecchymosis evident across the dorsal and plantar aspects of the midfoot. A particularly concerning finding was the presence of a "plantar ecchymosis" or "footprint sign," highly suggestive of a Lisfranc ligament disruption. The forefoot appeared abducted relative to the hindfoot. There was no evidence of skin compromise, tenting, or open wounds. Midfoot widening was palpable, though obscured by swelling.
- Palpation: Exquisite tenderness was localized over the Tarsometatarsal (TMT) joints, particularly at the base of the second metatarsal and the medial cuneiform. Significant pain was elicited with palpation along the entire Lisfranc ligament complex. Palpation of the cuboid, navicular, and cuneiforms also provoked discomfort, indicating potential associated injuries. A "piano key" sign was difficult to assess accurately due to severe pain and swelling but appeared to be positive for the first ray.
- Range of Motion (ROM): Active and passive range of motion of the ankle was restricted and painful, largely due to soft tissue swelling and patient guarding. Attempting to move the TMT joints elicited severe pain, and the foot was held in a relatively fixed, pronated, and abducted position. There was palpable instability of the second TMT joint with attempts at subtle manipulation.
- Neurological Assessment: Sensation was intact to light touch in all dermatomes (L4, L5, S1) corresponding to the foot. The deep peroneal nerve distribution (first web space) was intact. Motor function was limited due to pain, but dorsiflexion and plantarflexion of the ankle and toes were grossly intact, albeit weak.
- Vascular Assessment: Distal pulses (dorsalis pedis and posterior tibial) were palpable, albeit somewhat diminished due to swelling, but confirmed with Doppler. Capillary refill was brisk in all toes. The foot was warm and well-perfused. Due to the high-energy mechanism and significant swelling, the patient was closely monitored for signs of compartment syndrome, with serial clinical exams and compartment pressure measurements considered if suspicion increased.
Imaging & Diagnostics
Initial Radiographs
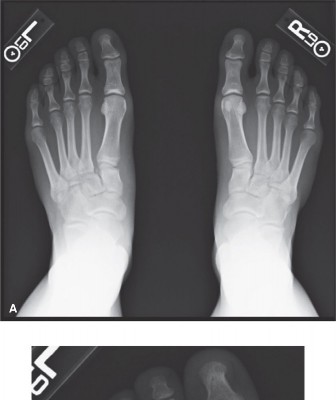
Initial weight-bearing radiographs were not obtained due to the patient's inability to bear weight. Standard non-weight-bearing radiographs of the right foot were obtained, including anteroposterior (AP), lateral, and 30-degree oblique views.
Key findings on plain radiographs included:
-
AP View:
- Widening of the interval between the first and second metatarsal bases, exceeding 2.5 mm, was clearly visible.
- Loss of alignment: The medial border of the second metatarsal shaft did not align with the medial border of the middle cuneiform.
- A "fleck sign" was observed, representing an avulsion fracture off the base of the second metatarsal or the medial cuneiform, indicative of a torn Lisfranc ligament.
- Mild lateral displacement of the second through fifth metatarsals was noted.
-
Lateral View:
- Dorsal displacement of the second metatarsal base relative to the middle cuneiform was present.
- Disruption of the normal midfoot arch could be inferred from the relationships.
-
Oblique View:
- Lateral displacement of the third, fourth, and fifth metatarsals from their respective cuneiform and cuboid articulations was evident.
- Loss of alignment: The medial border of the fourth metatarsal shaft did not align with the medial border of the cuboid.
Computed Tomography (CT)
Given the clear radiographic signs of midfoot injury and the high suspicion of a complex Lisfranc injury, a Computed Tomography (CT) scan of the right foot was performed. The CT provided invaluable detailed three-dimensional information about the bony architecture and fracture patterns.

The CT scan confirmed:
- Articular Incongruity: Significant subluxation and incongruity of the TMT joints, particularly involving the second through fifth metatarsals.
-
Fracture Patterns:
- Comminuted fracture at the base of the second metatarsal, extending into its articular surface.
- Small avulsion fracture from the plantar aspect of the medial cuneiform, corresponding to the attachment of the Lisfranc ligament.
- Impaction fracture of the middle cuneiform.
- Non-displaced fracture of the lateral cuneiform.
- Ligamentous Injury: While CT primarily assesses bony structures, the severe displacement and avulsion fractures strongly implied complete disruption of the Lisfranc ligament complex (dorsal, interosseous, and plantar components).
- Associated Injuries: No other significant bony injuries were identified in the hindfoot or ankle that would alter the primary management of the Lisfranc injury.
Magnetic Resonance Imaging (MRI)
An MRI was not deemed immediately necessary in this acute setting as the CT clearly demonstrated displaced bony Lisfranc injury requiring surgical intervention. MRI would primarily be indicated for subtle, purely ligamentous injuries where plain radiographs and stress views are inconclusive, or to evaluate associated soft tissue damage (e.g., cartilage, tendons) in a subacute or chronic setting if symptoms persist despite adequate bony reduction.
Pre-operative Templating
Pre-operative templating was performed meticulously using the CT scans. This involved:
- Identifying Fracture Lines: Precisely mapping the fracture lines and displacement patterns.
- Determining Reduction Strategy: Planning the sequence of reduction maneuvers (e.g., addressing the medial column stability first, then lateral).
- Fixation Construct Planning: Selecting appropriate screw lengths and diameters, determining optimal entry points and trajectories for cortical screws to reconstruct the Lisfranc ligament complex and stabilize the TMT joints. Consideration was given to the use of small fragment locking plates for additional stability, particularly for comminuted metatarsal bases or cuneiform fractures. The length and trajectory of the primary Lisfranc screw (from the medial cuneiform into the second metatarsal base) were carefully planned to ensure appropriate compression and stability without violating adjacent joint spaces or compromising other fixation elements.
Differential Diagnosis
A comprehensive differential diagnosis is crucial for any midfoot injury, especially when initial radiographs are equivocal for a Lisfranc injury. The following table compares common midfoot pathologies that could present similarly to a Lisfranc injury.
| Feature | Lisfranc Injury (Case Presentation) | Midfoot Sprain (High-Grade) | Cuboid Fracture / Subluxation | Navicular Fracture (Stress or Traumatic) |
|---|---|---|---|---|
| Mechanism | High-energy axial load with hyperplantarflexion/pronation. | Lower energy twist/fall, repetitive microtrauma. | Direct trauma to lateral foot, inversion/eversion. | Repetitive stress (athletic), direct trauma, avulsion. |
| Pain Location | Diffuse midfoot, centered at 1st/2nd TMT joint, plantar aspect. | Dorsal midfoot, diffuse, variable; may localize to TMT. | Lateral midfoot, over cuboid bone. | Dorsal midfoot, often localized over navicular. |
| Swelling / Ecchymosis | Marked, rapid onset; "plantar ecchymosis" common. | Variable, less severe than Lisfranc; plantar ecchymosis rare. | Localized to lateral midfoot, possibly diffuse. | Localized over navicular, variable. |
| Weight-Bearing | Severely painful, often impossible. | Painful, often possible with limp. | Painful, may be possible with limp. | Painful, especially with push-off; may be possible. |
| Radiographs (X-ray) | Widening of 1-2 intermetatarsal space, fleck sign, loss of alignment. | Usually normal; stress views may show subtle instability (<2mm). | Fracture line in cuboid; may show subluxation of calcaneocuboid. | Fracture line (often subtle); may require oblique views. |
| CT Scan | Confirms bony displacement, comminution, articular incongruity. | Normal bony alignment; may show subtle osteochondral lesions. | Defines fracture pattern, displacement, articular involvement. | Confirms fracture, comminution, non-union; bone marrow edema. |
| MRI Scan | Shows ligament disruption, cartilage injury, bone marrow edema. | Primarily shows ligament edema/tears (Lisfranc, intercuneiform). | Shows bone marrow edema, ligamentous injury. | Highly sensitive for stress fractures, cartilage, non-union. |
| Clinical Instability | Grossly unstable, "piano key" sign, abduction stress positive. | Minor instability on stress, or none. | May have subtle instability of lateral column. | Usually stable, pain primarily from bone injury. |
| Management | Operative fixation for displaced/unstable injuries. | RICE, NWB/PWB, bracing for stable injuries. | Operative for displaced/intra-articular; NWB/cast for stable. | Operative for displaced/avascular; NWB/cast for stable. |
| Long-Term Prognosis | High risk of post-traumatic arthritis, chronic pain, instability. | Generally good, but chronic pain/instability possible if high-grade. | Good, if stable and reduced; arthritis possible if intra-articular. | Variable, risk of avascular necrosis (especially body fractures). |
Surgical Decision Making & Classification
Surgical Decision Making
The decision for surgical intervention in this case was straightforward due to the clear evidence of a displaced and unstable Lisfranc injury on both plain radiographs and CT scan. Operative fixation is the gold standard for nearly all true Lisfranc injuries involving displacement or instability. Non-operative management is rarely indicated and typically reserved only for truly non-displaced, stable, purely ligamentous injuries without any bony involvement, confirmed by stress radiographs showing less than 2mm displacement compared to the contralateral foot. Even in such cases, close follow-up is imperative, and many surgeons advocate for prophylactic fixation given the high risk of secondary displacement and long-term functional impairment.
In our patient, the presence of:
1. Significant bony displacement and articular incongruity (widening of the first and second intermetatarsal space, loss of anatomical alignment).
2. Avulsion fractures ("fleck sign") indicative of complete Lisfranc ligament disruption.
3. Clinical instability and inability to bear weight.
...mandated urgent surgical intervention to restore anatomical alignment and stability. Delay in definitive management significantly increases the risk of post-traumatic osteoarthritis, chronic pain, midfoot collapse, and functional disability.
Classification
The Myerson Classification is the most widely accepted and clinically relevant classification system for Lisfranc injuries, primarily based on the pattern and direction of metatarsal displacement. Understanding the specific type aids in surgical planning.
- Type A (Homolateral Total Incongruity): All five metatarsals are displaced in the same direction, usually laterally, but without any widening between the first and second metatarsals. This type usually results from a high-energy direct crush injury or an indirect rotational force.
-
Type B (Partial Incongruity):
One or more metatarsals are displaced from the tarsus, but not all.
- Type B1 (Medial Dislocation): Involves displacement of the first metatarsal (often with the medial cuneiform) medially, sometimes with displacement of the second metatarsal medially as well.
- Type B2 (Lateral Dislocation): Involves displacement of the second through fifth metatarsals laterally, with the first metatarsal remaining in alignment. This is the most common pattern and often associated with the "fleck sign."
-
Type C (Divergent):
Characterized by displacement of the first metatarsal medially and the second through fifth metatarsals laterally, creating a divergent pattern. This usually indicates a more severe injury involving both medial and lateral columns.
- Type C1 (Partial Divergent): Only one or two metatarsals displaced divergently.
- Type C2 (Total Divergent): All metatarsals displaced divergently.
Based on the described radiographic and CT findings (widening between first and second metatarsals, lateral displacement of 2nd-5th metatarsals, and the presence of a fleck sign), our patient's injury was classified as a Myerson Type B2 Lisfranc injury . This implies a partial incongruity with lateral displacement of the lesser metatarsals, a common and often severely debilitating injury if not anatomically reduced.
Other classifications exist, such as the Quénu and Kuss classification (1909), which is more descriptive of injury patterns (homolateral, isolated, divergent), and the Hardcastle classification (1986), but Myerson remains the most practical for surgical planning.
Surgical Technique / Intervention
The primary goal of surgical intervention for a Lisfranc injury is to achieve and maintain an anatomical reduction of the TMT joints, thereby restoring the foot's structural integrity and preventing long-term sequelae such as post-traumatic arthritis and chronic pain.
Timing of Surgery
Surgery was performed after meticulous pre-operative planning, within 72 hours of injury. Early intervention is preferred once soft tissue swelling has adequately resolved, typically within a few days, to minimize complications and facilitate reduction. Excessive swelling, fracture blisters, or impending skin compromise would necessitate a delay, potentially with temporary external fixation to stabilize the foot and allow soft tissue healing.
Patient Positioning and Approach
- Patient Positioning: The patient was positioned supine on a radiolucent operating table. A bump was placed under the ipsilateral hip to allow for neutral alignment of the lower extremity. A high thigh tourniquet was applied to ensure a bloodless field, which is critical for identifying subtle anatomical landmarks and performing precise reduction.
- Fluoroscopy: A C-arm fluoroscopy unit was positioned to allow for intraoperative AP, lateral, and oblique views of the foot. Contralateral foot radiographs were obtained for comparison to assess the anatomical reduction more accurately.
-
Surgical Approach:
A dual dorsal incision approach was utilized to gain optimal access to both the medial and central columns.
- Medial Incision: A longitudinal incision was made over the first TMT joint, between the tibialis anterior and extensor hallucis longus tendons. This provides access to the first metatarsal-medial cuneiform joint.
- Lateral Incision: A second longitudinal incision was made between the second and third metatarsals, extending proximally over the TMT joints. This allows access to the second and third TMT joints and aids in visualizing the Lisfranc ligament complex. Meticulous dissection was performed to protect superficial nerves and veins.
- Capsulotomy: Limited capsulotomy was performed to expose the articular surfaces and facilitate direct visualization of the joint reduction. Hematoma and any interposed soft tissue fragments were debrided.
Reduction Techniques
Anatomical reduction is paramount. The reduction sequence typically focuses on restoring the critical medial column and then proceeding laterally.
-
Medial Column Reduction (1st TMT Joint):
- The first metatarsal-medial cuneiform joint was reduced under direct visualization. This often involves gentle traction and direct manipulation.
- Once reduced, provisional fixation was achieved with a 1.6 mm or 2.0 mm K-wire passing from the first metatarsal into the medial cuneiform.
-
Second Metatarsal-Cuneiform Reduction (Keystone):
This is the most critical step as the second metatarsal base acts as the "keystone" of the midfoot arch.
- The second metatarsal was anatomically reduced to the middle cuneiform. This often requires careful traction on the forefoot, direct pressure on the second metatarsal base, and manipulation of the cuneiforms. Small pointed reduction clamps or Hohmann retractors were used.
- The goal is to align the medial cortex of the second metatarsal with the medial cortex of the middle cuneiform.
- Provisional fixation was achieved with a K-wire passing from the base of the second metatarsal into the middle cuneiform.
-
Third, Fourth, and Fifth Metatarsal Reduction:
- Once the medial and central columns were stable, the lateral metatarsals (3rd, 4th, 5th) were reduced to their respective cuneiform and cuboid articulations.
- These reductions often follow the reduction of the keystone second metatarsal due to the intrinsic stability provided by the transverse arch. Direct manipulation and provisional K-wires were utilized.
-
 This image (GIF) could depict the sequential reduction of the metatarsals and their provisional fixation with K-wires, demonstrating the dynamic nature of reduction.
This image (GIF) could depict the sequential reduction of the metatarsals and their provisional fixation with K-wires, demonstrating the dynamic nature of reduction.
Throughout the reduction process, intraoperative fluoroscopy (AP, lateral, and oblique views) was extensively used to confirm anatomical alignment. Particular attention was paid to the 1st-2nd intermetatarsal space and the alignment of the medial borders of the second and fourth metatarsals with their respective tarsal bones.
Fixation Construct
Once anatomical reduction was achieved and confirmed, definitive fixation was performed.
-
Lisfranc Ligament Reconstruction/Fixation:
- The primary fixation was a cortical screw (typically 3.5 mm or 4.0 mm, fully threaded and non-compressive) placed from the medial cuneiform into the base of the second metatarsal. This screw effectively reconstructs the interosseous Lisfranc ligament, which is critical for midfoot stability. Care was taken to ensure the screw did not cross the joint space in a compressive manner, as this could lead to premature arthritis. The screw trajectory should be slightly plantar to dorsal.
- Additionally, a cortical screw was placed from the medial cuneiform into the base of the first metatarsal to stabilize the first TMT joint.
-
Intercuneiform and Metatarsal-Cuneiform Fixation:
- Additional cortical screws (e.g., 3.5 mm or 4.0 mm) or K-wires were used to stabilize other injured TMT joints (e.g., 3rd metatarsal to lateral cuneiform, 4th metatarsal to cuboid, 5th metatarsal to cuboid). These screws should primarily be transarticular to maintain reduction, not compressive.
-
Plate Fixation (as indicated):
- In cases of significant comminution, particularly at the base of the second metatarsal or the cuneiforms, dorsal locking plates (e.g., small fragment T-plates or straight plates) were used in addition to or instead of screws. Plates offer increased stability, especially in complex fracture patterns. They can be used to bridge comminuted segments, providing indirect reduction and stabilization.
- For the medial column (1st TMT), a mini-locking plate can provide robust fixation, particularly if the joint is unstable or if there is a fracture of the medial cuneiform.
- For the central and lateral columns, individual metatarsal plates can be used, or a longer bridge plate can be considered depending on the extent of injury.
-
Hardware Considerations:
- The hardware used should be strong enough to maintain reduction but allow for eventual removal.
- Temporary K-wires were removed after definitive screw or plate fixation was achieved.
- The choice between screws and plates is often debated. While screws directly restore ligamentous anatomy, plates offer broader stability, especially in comminuted or unstable injuries, and may reduce the need for hardware removal in some cases, although hardware prominence remains a concern.
- In this patient, a combination of cortical screws for the Lisfranc interval and 1st TMT joint, augmented by a dorsal mini-plate for the comminuted second metatarsal base, was employed to achieve robust, anatomical fixation.
After confirming the final reduction and fixation with fluoroscopy, the wounds were irrigated, and the incisions were closed in layers. A sterile dressing and a well-padded short-leg splint were applied.
Post-Operative Protocol & Rehabilitation
Post-operative management is as critical as the surgical technique in achieving optimal long-term outcomes for Lisfranc injuries.
Immediate Post-Operative Period (Weeks 0-6)
- Immobilization: The foot was placed in a non-weight-bearing (NWB) short-leg splint or cast.
- Elevation and Ice: Strict elevation of the limb and regular application of ice packs were prescribed to minimize swelling and pain.
- Pain Management: A multimodal approach to pain management was utilized, including opioids, NSAIDs, and regional nerve blocks as needed.
- Wound Care: Incision sites were monitored for signs of infection. Suture removal typically occurred at 2-3 weeks post-op.
- Deep Vein Thrombosis (DVT) Prophylaxis: Given the NWB status, DVT prophylaxis was initiated according to institutional guidelines.
- Physical Therapy (Early): Gentle, active range of motion of the ankle and toes was encouraged once wounds were stable, but strictly NWB for the midfoot. This helps prevent stiffness in adjacent joints.
Mid-Phase Rehabilitation (Weeks 6-12)
- Hardware Removal (Optional, but often recommended for screws): For patients with transarticular screws, particularly the Lisfranc screw, removal is often performed between 3-6 months post-operatively. This prevents screw breakage, allows normal midfoot motion, and reduces the risk of post-traumatic arthritis. In our patient, a staged hardware removal of the Lisfranc screw was planned at 4 months post-op. Plates may or may not be removed, depending on patient symptoms and surgeon preference.
-
Weight-Bearing Progression:
- After screw removal (if performed) or at approximately 8-10 weeks post-op if only plates or non-transarticular screws were used, protected weight-bearing (PWB) in a CAM walker boot was initiated.
- The progression was gradual, starting with 25% PWB, advancing to 50% over 2-4 weeks, as tolerated.
-
Physical Therapy (Progressive):
- Initiation of gentle, non-painful active and passive range of motion exercises for the midfoot.
- Manual therapy to restore joint mobility.
- Introduction of isometric strengthening exercises for ankle and foot musculature.
- Balance and proprioception exercises (e.g., single-leg stance, wobble board) once PWB is established.
Late-Phase Rehabilitation (Months 3-6 and Beyond)
- Full Weight-Bearing (FWB): Full weight-bearing was typically achieved by 4-6 months post-op, often initially in supportive footwear or an orthotic.
- Strengthening: Progressive resistive exercises for all foot and ankle muscle groups.
- Gait Training: Normalization of gait mechanics.
- Functional Progression: Introduction of functional activities, agility drills, and sport-specific training for athletes, guided by the patient's symptoms and recovery.
- Custom Orthotics: May be prescribed to support the arch and distribute pressure evenly, especially if there is a tendency for midfoot collapse or persistent pain.
Expected Outcomes and Complications
- Good to Excellent: Approximately 60-70% of patients achieve good to excellent functional outcomes with anatomical reduction and appropriate rehabilitation.
- Post-Traumatic Arthritis: The most common long-term complication, occurring in 20-50% of cases, even with anatomical reduction. May necessitate future salvage procedures such as midfoot arthrodesis.
- Chronic Pain: Due to arthritis, nerve irritation, or persistent instability.
- Hardware-Related Complications: Screw loosening, breakage, prominence, infection. This is a primary reason for routine hardware removal.
- Malunion/Nonunion: Failure to achieve or maintain anatomical reduction, leading to chronic instability or deformity.
- Complex Regional Pain Syndrome (CRPS): A rare but debilitating complication.
- Recurrent Instability: If the Lisfranc ligament complex does not heal adequately or fixation fails.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- High Index of Suspicion: Any patient presenting with midfoot pain and swelling after trauma, particularly a high-energy mechanism or a seemingly innocuous twist, should be evaluated for a Lisfranc injury. Don't dismiss it as a "sprain."
- Clinical Examination: Always look for the "plantar ecchymosis" or "footprint sign"—it's pathognomonic. Palpate the TMT joints specifically. Assess for midfoot widening and instability.
-
Radiographic Vigilance:
- Weight-bearing views: If possible and tolerated, these are crucial for detecting subtle instability in equivocal cases.
- Contralateral views: Always compare to the uninjured foot for subtle asymmetries.
- Key radiographic signs: Widening of the 1st-2nd intermetatarsal space (>2.5mm), "fleck sign," and disruption of the medial column alignment (medial border of 2nd metatarsal with medial cuneiform).
- Oblique view importance: Essential for assessing the lateral TMT joints (4th metatarsal with cuboid).
- CT Scan: The gold standard for pre-operative planning, definitively identifying bony displacement, comminution, and articular incongruity. Don't rely solely on plain X-rays if suspicion is high.
- Anatomical Reduction: This is the single most important factor determining long-term outcomes. Any residual displacement, even 1-2 mm, significantly increases the risk of post-traumatic arthritis. Prioritize reduction of the keystone (2nd TMT joint).
- Stable Fixation: Use appropriate hardware (cortical screws, plates) to maintain reduction. The Lisfranc screw (medial cuneiform to 2nd metatarsal base) is critical. Ensure non-compressive technique if crossing joint lines to avoid arthrodesis.
- Compartment Syndrome: Maintain a high suspicion, especially in high-energy injuries with significant swelling. Monitor clinically and be prepared for pressure measurements/fasciotomy.
- Hardware Removal: Routine removal of transarticular screws (typically 3-6 months) is often recommended to prevent breakage and allow normal midfoot motion.
Pitfalls
- Missed Diagnosis: The most significant pitfall. Often misdiagnosed as a "sprain" leading to delayed treatment, chronic pain, and early arthritis. This is particularly true for subtle, purely ligamentous injuries.
- Inadequate Reduction: Failure to achieve or maintain true anatomical reduction leads to poor outcomes. Over-reduction or under-reduction are equally detrimental. Use intraoperative fluoroscopy aggressively in multiple planes.
- Premature Weight-Bearing: Applying weight too early can lead to loss of reduction, hardware failure, and progression of deformity. Adhere strictly to NWB protocols.
- Hardware-Related Complications: Screw malposition (e.g., entering wrong joint, too long/short), breakage, loosening, or soft tissue irritation are common. Non-compressive screws across joints are critical to avoid premature arthrodesis.
- Failure to Address Associated Injuries: Overlooking other concomitant fractures (e.g., navicular, cuboid) or soft tissue injuries can compromise overall recovery.
- Ignoring Soft Tissue Envelope: Operating through severely swollen or blistered skin increases infection risk. Temporize with external fixation if necessary.
- Neglecting Rehabilitation: Inadequate or inconsistent post-operative physical therapy can lead to stiffness, weakness, and persistent functional deficits. A structured, progressive rehabilitation program is essential.
- Underestimating the Severity: Even seemingly "minor" Lisfranc injuries can have devastating long-term consequences if not managed meticulously. Always treat with respect and thoroughness.
You Might Also Like