Ankle Sprains: Epidemiology, Pathophysiology, and Surgical Anatomy of Ligamentous Injuries
Key Takeaway
Ankle sprains are ligamentous injuries, affecting millions annually, ranging from mild stretches (Grade I) to complete ruptures (Grade III). They often lead to chronic instability. Key involved structures include the lateral collateral ligament complex (ATFL, CFL, PTFL), medial (deltoid) ligament, and syndesmotic ligaments (AITFL, PITFL), crucial for ankle stability.
Introduction & Epidemiology
Ankle sprains represent a spectrum of ligamentous injuries involving the talocrural and subtalar joints, ranging from mild ligamentous stretch to complete rupture. These injuries are among the most prevalent musculoskeletal pathologies encountered in orthopedics, affecting both athletic and general populations. Understanding the mechanistic, anatomical, and rehabilitative nuances of ankle sprains is critical for guiding appropriate management strategies, from conservative care to surgical intervention for chronic instability.
Epidemiologically, ankle sprains account for an estimated 1.5 to 2.0 million injuries annually in the United States, with an incidence rate of approximately 2.15 per 1,000 person-years in the general population. This figure dramatically escalates in athletic cohorts, particularly in sports involving jumping, cutting, and pivoting, such as basketball, soccer, volleyball, and football. Recurrence rates are substantial, with up to 70% of individuals experiencing a subsequent sprain, often within the first year following the initial injury. This propensity for recurrence frequently leads to the development of chronic ankle instability (CAI), a multifactorial condition characterized by recurrent symptomatic episodes of instability, giving way, and persistent pain, which affects approximately 20-40% of patients following an initial acute sprain. The economic burden associated with ankle sprains and CAI, encompassing direct healthcare costs, lost productivity, and long-term disability, is considerable.
Classification systems for acute ankle sprains typically grade the severity based on the degree of ligamentous injury and functional impairment:
*
Grade I:
Mild stretch of the ligament with microscopic tearing, minimal pain, swelling, and no functional loss or instability.
*
Grade II:
Partial macroscopic tear of the ligament, moderate pain, swelling, ecchymosis, mild-to-moderate functional impairment, and mild-to-moderate instability on examination.
*
Grade III:
Complete rupture of one or more ligaments, severe pain, swelling, ecchymosis, significant functional loss, and gross mechanical instability.
While acute management often focuses on symptomatic relief and early mobilization, persistent symptoms and recurrent instability necessitate a thorough evaluation to identify underlying mechanical or functional deficits that may warrant surgical consideration.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the intricate ligamentous and bony architecture of the ankle is paramount for diagnosing and surgically treating ankle instability. The ankle joint complex comprises the talocrural (tibiotalar) joint, primarily responsible for dorsiflexion and plantarflexion, and the subtalar (talocalcaneal) joint, facilitating inversion and eversion.
Lateral Collateral Ligament Complex
The lateral collateral ligament (LCL) complex is the most frequently injured ligamentous structure, particularly during inversion injuries. It consists of three distinct ligaments:
1.
Anterior Talofibular Ligament (ATFL):
Originates from the anterior border of the distal fibula and inserts onto the lateral talar neck. It is the weakest and most commonly injured component. The ATFL resists anterior translation of the talus on the tibia and excessive inversion, especially when the ankle is in plantarflexion. Its fan-like shape allows it to resist internal rotation of the talus.
2.
Calcaneofibular Ligament (CFL):
Originates from the tip of the fibula and courses inferiorly and posteriorly to insert onto the lateral calcaneal surface. The CFL is extra-articular and resists inversion of the talus, particularly when the ankle is in a neutral or dorsiflexed position. Its relationship to the peroneal tendons (superficial to the ligament) is clinically significant during surgical dissection.
3.
Posterior Talofibular Ligament (PTFL):
Originates from the posterior border of the fibula and inserts onto the posterior aspect of the talus. It is the strongest component of the LCL complex and primarily resists posterior talar translation and extreme dorsiflexion. It is rarely injured in isolation but can be affected in severe inversion injuries or fracture-dislocations.
Medial (Deltoid) Ligament Complex
The deltoid ligament is a robust triangular structure on the medial aspect of the ankle, comprising superficial and deep layers. It provides significant stability against eversion and valgus forces and is less commonly injured in isolation due to its strength. Isolated deltoid ligament injury often suggests an associated fracture or syndesmotic injury.
*
Superficial Layer:
Includes the tibionavicular, tibiospring, and superficial tibiotalar ligaments. These fan out from the medial malleolus to the navicular, spring ligament, and talus, respectively.
*
Deep Layer:
Consists of the anterior and posterior tibiotalar ligaments. These attach directly from the medial malleolus to the talus, providing the primary restraint to talar external rotation and valgus stress.
Syndesmotic Ligament Complex
The distal tibiofibular syndesmosis is a fibrous joint held together by four primary components:
1.
Anterior Inferior Tibiofibular Ligament (AITFL):
Connects the anterior border of the distal tibia to the anterior aspect of the distal fibula.
2.
Posterior Inferior Tibiofibular Ligament (PITFL):
Connects the posterior border of the distal tibia to the posterior aspect of the distal fibula.
3.
Interosseous Ligament (IOL):
A continuation of the interosseous membrane, providing significant stability.
4.
Inferior Transverse Ligament (ITL):
A deep portion of the PITFL, contributing to posterior stability.
These ligaments work collectively to maintain the integrity of the tibiofibular mortise, preventing excessive widening and rotation, which are crucial for normal ankle kinematics. Syndesmotic injuries ("high ankle sprains") often involve greater force and have a longer recovery trajectory compared to isolated lateral ankle sprains.
Bony Anatomy & Kinematics
The bony anatomy, including the distal tibia, fibula, talus, and calcaneus, defines the ankle joint's stability. The mortise created by the tibia and fibula articulates with the dome of the talus. The shape of the talus, wider anteriorly, contributes to ankle stability in dorsiflexion. Ankle sprains primarily result from a sudden, uncontrolled inversion or eversion movement, often combined with plantarflexion or dorsiflexion, causing excessive strain on the ligaments. Inversion and plantarflexion typically stress the ATFL and CFL. Proprioceptive deficits following injury contribute significantly to the development and perpetuation of functional ankle instability.
Indications & Contraindications
The decision for operative versus non-operative management of ankle sprains, particularly in the context of chronic ankle instability, is guided by a comprehensive evaluation of the patient's symptoms, activity level, objective instability, and the presence of concomitant pathologies.
Non-Operative Indications
- Acute Grade I and II ankle sprains: The vast majority of acute lateral ankle sprains are successfully managed non-operatively with a phased rehabilitation protocol (e.g., RICE, early protected mobilization, progressive strengthening, proprioceptive training).
- Absence of significant mechanical instability: Clinical examination and stress radiographs do not demonstrate gross instability.
- Good functional outcome with conservative care: Patients who achieve satisfactory stability and return to desired activity levels without recurrent episodes after a trial of appropriate non-operative management (typically 3-6 months).
- Patient preference: For patients who decline surgery or have low functional demands.
- Contraindications to surgery: As listed below.
Operative Indications
Surgical intervention is primarily indicated for chronic ankle instability (CAI) that has failed a comprehensive course of non-operative treatment, or for specific acute injuries with significant mechanical disruption or concomitant pathologies.
*
Chronic Lateral Ankle Instability (CAI):
Persistent symptomatic instability (recurrent sprains, giving way episodes, pain) despite a minimum of 3-6 months of high-quality conservative management, especially in active individuals or athletes. Objective evidence of mechanical instability via stress radiographs (anterior drawer >10 mm or >3 mm difference compared to contralateral side; talar tilt >10-15 degrees or >5 degrees difference) supports this indication.
*
High-Grade Acute Ankle Sprains with Gross Instability:
While rare, acute Grade III sprains with significant displacement or associated pathologies might be considered for early repair, particularly in elite athletes. However, evidence supporting superior outcomes of acute repair over conservative management is limited for isolated ligamentous injuries.
*
Concomitant Pathologies:
The presence of co-existing conditions that contribute to symptoms or instability and require surgical address. These may include:
* Osteochondral lesions of the talus (OCL/OCD).
* Peroneal tendon pathology (e.g., subluxation, tears, tendinopathy).
* Anterolateral impingement (soft tissue or osseous).
* Loose bodies.
* Synovitis.
*
Syndesmotic Instability:
Significant diastasis of the distal tibiofibular syndesmosis, often associated with fractures (e.g., Weber C fibula fracture, Maisonneuve fracture) or in isolated syndesmotic sprains unresponsive to conservative care.
*
Revision Surgery:
For failed previous ligamentous repair or reconstruction.
Contraindications
- Acute injury that meets criteria for non-operative management: Unnecessary surgery increases risk without clear benefit.
- Unrealistic patient expectations: Especially regarding return to sport or complete symptom resolution.
- Significant peripheral vascular disease: Compromises healing.
- Active local or systemic infection.
- Neuropathic arthropathy (Charcot joint): Contraindicates reconstructive surgery due to high failure rates.
- Severe systemic comorbidities: Increasing anesthetic and surgical risks.
- Lack of patient compliance: For demanding post-operative rehabilitation protocols.
- Advanced ankle arthritis: In such cases, reconstructive surgery is unlikely to provide benefit and an ankle fusion or arthroplasty may be more appropriate.
Operative vs. Non-Operative Indications: A Summary
| Feature | Non-Operative Management | Operative Management |
|---|---|---|
| Acute Sprains | Grade I/II, isolated, no gross instability, no associated injuries | Rare for isolated ligamentous injury; considered for Grade III with gross instability in elite athletes (controversial) |
| Chronic Instability | Successful conservative trial (3-6 months), no recurrent symptoms, no mechanical instability | Failed conservative management (3-6 months), recurrent sprains/giving way, objective mechanical instability (stress views) |
| Associated Pathology | None or managed conservatively | Osteochondral lesions, peroneal tendon pathology, impingement, loose bodies |
| Syndesmosis | Isolated stable syndesmotic injury | Unstable syndesmosis (diastasis), often with fracture |
| Patient Profile | Low functional demands, unwilling/unfit for surgery | High functional demands, athlete, compliant with rehab |
| Imaging | Minimal findings, no significant instability on stress views | Significant instability on stress views, MRI showing severe ligament disruption or associated lesions |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential to ensure a successful outcome and minimize complications in ankle ligament surgery.
Clinical Assessment
- History: Detailed history of injury mechanism, frequency, and severity of sprains; nature of instability (mechanical vs. functional); impact on activities of daily living and sports; prior treatments and their efficacy. Assess for generalized ligamentous laxity (e.g., Beighton score).
-
Physical Examination:
- Inspection: Swelling, ecchymosis, deformities.
- Palpation: Tenderness over ligamentous structures, fibula, talar dome, peroneal tendons.
- Range of Motion (ROM): Active and passive, comparing to contralateral side. Assess for mechanical blocks or stiffness.
- Strength: Assessment of dorsiflexors, plantarflexors, invertors, and evertors.
-
Stability Tests:
- Anterior Drawer Test: Assesses ATFL integrity. Performed with the ankle in 10-20 degrees plantarflexion. A positive test indicates excessive anterior translation of the talus.
- Talar Tilt Test: Assesses CFL (and ATFL, deltoid) integrity. Performed in neutral dorsiflexion (for CFL) and plantarflexion (for ATFL). Positive if excessive inversion (lateral ligaments) or eversion (deltoid) compared to the contralateral side.
- Cotton Test: Assesses syndesmotic instability (lateral translation of talus).
- External Rotation Stress Test: For syndesmotic injury.
- Proprioception: Single leg stance, star excursion balance test.
- Neurological Examination: Assess integrity of superficial peroneal and sural nerves.
Imaging
- Plain Radiographs: Anteroposterior (AP), lateral, and mortise views of the ankle are mandatory to rule out fractures (e.g., occult fibula, talus, or calcaneus fractures), assess joint alignment, and look for signs of impingement or early arthrosis.
-
Stress Radiographs:
Essential for objective quantification of mechanical instability.
- Anterior Drawer Stress Radiograph: Measures anterior talar translation. Significant if >10 mm or >3 mm difference compared to the contralateral side.
- Talar Tilt Stress Radiograph: Measures talar tilt. Significant if >10-15 degrees or >5 degrees difference compared to the contralateral side.
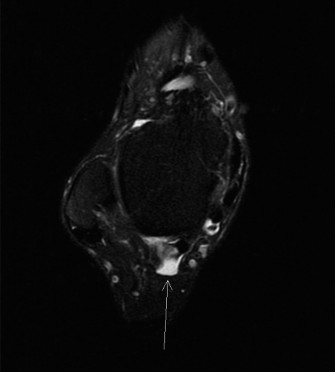
- Magnetic Resonance Imaging (MRI): The gold standard for assessing soft tissue structures. Highly valuable for evaluating ligamentous integrity (ATFL, CFL, deltoid, syndesmosis), identifying associated pathologies such as osteochondral lesions of the talus, peroneal tendon tears or subluxation, synovitis, and impingement. An MRI is often crucial for surgical planning, especially when considering reconstruction.
- Computed Tomography (CT): Useful for detailed assessment of bony morphology, osteochondral lesions, coalition, or impingement. CT arthrogram can provide additional detail for chondral surface abnormalities.
Pre-operative Counseling
Thorough discussion with the patient regarding the diagnosis, rationale for surgery, surgical options (repair vs. reconstruction), potential risks and benefits, expected recovery timeline, and the critical role of post-operative rehabilitation.
Anesthesia
Typically, general anesthesia combined with a regional anesthetic block (e.g., popliteal block or ankle block) for superior post-operative pain control.
Patient Positioning
The patient is usually positioned supine on the operating table.
* A small bump or pillow is placed under the ipsilateral hip to allow internal rotation of the leg, ensuring optimal access to the lateral ankle.
* A pneumatic tourniquet is applied to the proximal thigh to provide a bloodless field, typically inflated to 250-300 mmHg, or 100 mmHg above systolic pressure.
* The limb is prepped and draped from the knee to the toes, ensuring sterile field.
* An image intensifier (C-arm) should be available for intraoperative fluoroscopy, particularly if concomitant osteochondral lesions or syndesmotic stabilization are anticipated.
* For arthroscopic procedures, a distraction tower may be used to facilitate joint visualization.
Detailed Surgical Approach / Technique
Surgical techniques for ankle instability are broadly categorized into anatomic repairs (e.g., modified Broström-Gould) and anatomic/non-anatomic reconstructions (e.g., tendon autograft/allograft). The choice depends on tissue quality, degree of instability, and patient factors. Arthroscopic assessment of the joint often precedes open repair/reconstruction to address intra-articular pathologies.
1. Ankle Arthroscopy (Diagnostic & Therapeutic)
Prior to open repair, arthroscopy is routinely performed to identify and address intra-articular pathologies that may mimic or contribute to instability symptoms.
*
Portals:
Anteromedial (medial to tibialis anterior, lateral to saphenous nerve and vein) and anterolateral (lateral to peroneus tertius, medial to superficial peroneal nerve). Additional portals (e.g., posterolateral) may be used for posterior pathology.
*
Procedure:
Systematically evaluate the entire talocrural joint, including the talar dome (chondral surfaces), distal tibia, lateral and medial gutters, and anterior joint capsule.
*
Debridement:
Remove synovitis, scar tissue, or loose bodies that contribute to impingement or pain.
*
Microfracture/OATS:
For osteochondral lesions of the talus.
*
Impaction Fractures:
Address with internal fixation if needed.
2. Lateral Ankle Ligament Repair: Modified Broström-Gould Technique
This is the most common and gold standard open anatomic repair for chronic lateral ankle instability with good quality native ligament tissue.
- Incision: A curvilinear or oblique incision (typically 4-6 cm) centered over the distal fibula, extending from approximately 1 cm proximal to the fibular tip, distally and slightly anteriorly towards the base of the 4th metatarsal. Care is taken to avoid the superficial peroneal nerve (medial) and sural nerve (posterior).
-
Dissection & Internervous Plane:
- Skin and Subcutaneous Tissue: Carefully incise. Identify and protect subcutaneous nerves and veins. The superficial peroneal nerve typically crosses the incision anteriorly, while the sural nerve runs more posteriorly.
- Fascia: Incise the crural fascia. Identify the peroneus brevis and longus tendons lying posterior to the fibula.
- Ligament Exposure: The inferior extensor retinaculum is often identified and can be used for reinforcement. The ATFL and CFL stumps are identified. The ATFL originates from the anterior border of the fibula and inserts on the talar neck. The CFL originates from the fibular tip and passes deep to the peroneal tendons to insert on the calcaneus. The internervous plane is generally between the peroneal tendons posteriorly and the extensor digitorum longus/peroneus tertius anteriorly.
-
Ligament Preparation:
- Debride attenuated or scarred ligamentous tissue from the anterior edge and tip of the fibula. Freshen the fibular attachment site using a burr or rasp to promote healing.
- The ATFL and CFL remnants are identified and mobilized.
-
Repair:
- Anchor Placement: Place two to three suture anchors (e.g., 2.4 mm to 3.5 mm bioabsorbable or titanium) into the anterior aspect and tip of the distal fibula. The anterior anchor is typically for the ATFL, and the distal anchor for the CFL, though placement varies based on tear pattern.
- Suture Passage: Pass the sutures from the anchors through the remnants of the ATFL and CFL.
- Tensioning & Knot Tying: The ankle is held in approximately 5-10 degrees of dorsiflexion and slight eversion (to prevent overtightening and varus deformity). The sutures are then progressively tied, imbricating the torn ligament stumps back to their anatomic origin on the fibula. This restores tension and stability.
-
Gould Modification (Inferior Extensor Retinaculum Reinforcement):
- The inferior extensor retinaculum (IER) is a strong fascial structure located anterior to the ankle joint. A flap of the IER is carefully undermined from its attachments, leaving it attached medially.
- This flap is then advanced proximally and posteriorly, sutured to the repaired ligaments and the periosteum of the distal fibula. This provides an additional layer of reinforcement, significantly augmenting the primary repair. Some surgeons also incorporate a portion of the peroneus brevis tendon or a strip of periosteum.
- Closure: Layered closure of the subcutaneous tissue and skin.
3. Anatomical Lateral Ankle Ligament Reconstruction
Indicated when native tissue quality is poor (e.g., revision surgery, generalized ligamentous laxity, severe chronic instability). Autografts (gracilis, semitendinosus, plantaris) or allografts are typically used.
- Incision & Exposure: Similar to the Broström approach.
- Graft Harvest & Preparation: If autograft is used, it is harvested (e.g., ipsilateral gracilis or semitendinosus) and prepared on the back table.
-
Tunnel Creation:
- Fibular Tunnel: A tunnel is drilled obliquely through the distal fibula from anterior-inferior to posterior-superior, or two separate tunnels for ATFL and CFL limbs.
- Talar Tunnel: A tunnel is drilled into the lateral talar neck, simulating the ATFL origin.
- Calcaneal Tunnel: A tunnel is drilled into the lateral calcaneus, simulating the CFL origin.
-
Graft Passage & Fixation:
- The graft is passed through the fibular tunnel.
- One limb of the graft is passed into the talar tunnel and fixed (e.g., with an interference screw) to reconstruct the ATFL.
- The second limb is passed into the calcaneal tunnel and fixed to reconstruct the CFL.
- The ankle is held in slight dorsiflexion and neutral rotation during tensioning and fixation to avoid overtightening.
- Tensioning: Critical step to restore anatomic tension without overtightening or creating impingement.
- Closure: Layered closure.
4. Syndesmotic Fixation (for unstable syndesmotic injuries)
Often performed in conjunction with fibular fracture fixation.
- Reduction: The tibiofibular syndesmosis must be anatomically reduced. This often requires an assistant to apply posterior-anterior compression and external rotation of the foot to close the syndesmotic diastasis. Proper reduction is critical and verified with intraoperative fluoroscopy (e.g., true mortise view, lateral view, check for parallel relationship between tibia and fibula).
-
Fixation:
- Screw Fixation: One or two tricortical screws (typically 3.5 or 4.5 mm cortical screws) are placed from the fibula, through the tibia, usually 2-4 cm proximal to the tibiotalar joint line. The screws are often placed at a 30-degree angle anteriorly from the perpendicular relative to the fibula shaft. The ankle is typically in neutral dorsiflexion for screw insertion, though some prefer slight dorsiflexion to prevent over-compression in plantarflexion.
- Suture Button Fixation (e.g., TightRope®): Becoming increasingly popular, especially for isolated syndesmotic injuries or in athletes due to its dynamic nature. A small button is passed through the medial tibia and another through the lateral fibula (often using drill holes from fibula to tibia). The sutures connecting the buttons are then tensioned and tied, reducing the syndesmosis. This allows for some physiological motion and may negate the need for hardware removal.
- Intraoperative Assessment: Confirm reduction and stability with fluoroscopy and manual stress testing.
Complications & Management
Despite meticulous surgical technique, complications can occur following ankle ligament repair or reconstruction. Proactive identification and appropriate management are crucial for salvage and optimizing patient outcomes.
Common Complications & Management Strategies
| Complication | Incidence (Approx.) | Salvage / Management Strategy |
|
1. Chronic Ankle Instability (CAI)
| 20-40% of patients after acute sprain |
Management:
Non-surgical management for CAI involves a combination of activity modification, physical therapy focusing on proprioception, muscle strengthening (especially evertors), and neuromuscular control. Bracing or taping for stability.
Failure to improve after 3-6 months
of comprehensive, supervised rehabilitation, indicated by recurrent sprains, persistent "giving way" sensations, and functional limitations, points toward surgical intervention (e.g., modified Broström-Gould repair, anatomic reconstruction). |
|
2. Peroneal Tendon Pathology
| 10-20% (often subtle) |
Management:
Initial non-operative treatment with rest, NSAIDs, physical therapy, and bracing. If symptoms persist (pain, instability, locking) or there's clear evidence of tendon tear/subluxation on MRI, surgical intervention is indicated (e.g., tenosynovectomy, debridement, repair of longitudinal tears, groove deepening, superior peroneal retinaculum repair). |
| Complication | Incidence (Approx.) | Salvage / Management Strategy |
|---|---|---|
| **1. Recurrence of Instability (Failure of Repair/Reconstruction)** |
5-15% (Broström-Gould)
Higher for poor tissue quality or non-compliance |
**Management:** Re-evaluate mechanical vs. functional instability. Conservative management (PT, bracing) if functional. If mechanical failure is confirmed, revision surgery with an anatomical reconstruction (autograft/allograft) is often indicated. Address underlying causes (e.g., inadequate rehabilitation, untreated concomitant pathology). |
| **2. Stiffness / Arthrofibrosis** | 5-10% | **Management:** Early and aggressive physiotherapy focusing on range of motion (ROM) exercises. Manual therapy, joint mobilizations. NSAIDs. If refractory, consider manipulation under anesthesia (MUA) or arthroscopic debridement/arthrolysis. Prevention involves strict adherence to post-operative protocols. |
| **3. Nerve Injury (Superficial Peroneal, Sural)** |
2-10% (transient paresthesia)
<1% (permanent neurological deficit) |
**Management:** Most are neurapraxias and resolve spontaneously within weeks to months. Protection from further irritation. Neuropathic pain management (gabapentin, pregabalin). If persistent and debilitating, consider nerve block, surgical neurolysis, or rarely, nerve grafting/transfer. Careful surgical dissection to identify and protect nerves. |
| **4. Wound Complications (Infection, Dehiscence, Delayed Healing)** |
Superficial: 2-5%
Deep: <1% |
**Management:**
* **Superficial Infection:** Oral antibiotics, local wound care. * **Deep Infection:** Urgent surgical debridement, intravenous antibiotics, potentially hardware removal (if present and infected). * **Dehiscence:** Local wound care, secondary closure, or skin grafting depending on severity. Prevention with meticulous soft tissue handling, appropriate closure, and infection prophylaxis. |
| **5. Complex Regional Pain Syndrome (CRPS)** | <1% | **Management:** Early recognition is key. Multidisciplinary approach: regional nerve blocks, physical therapy (desensitization), pharmacotherapy (NSAIDs, gabapentinoids, tricyclic antidepressants), pain management specialist referral. Aggressive pain control post-operatively. |
| **6. Persistent Pain (Non-Instability Related)** | Variable (e.g., impingement, neuroma, unaddressed concomitant pathology) |
**Management:** Thorough diagnostic workup (repeat imaging, diagnostic injections) to identify source.
* **Anterior Impingement:** Arthroscopic debridement. * **Neuroma:** Surgical excision. * **Unaddressed Pathology:** Targeted surgical intervention. * **Psychological factors:** Pain psychology referral. |
| **7. Hardware Complications (Syndesmotic Screws/Buttons)** |
Screws: 10-30% (breakage, loosening, pain)
Suture buttons: <5% (button migration/cut-out) |
**Management:**
* **Painful Hardware:** Elective removal after radiographic evidence of syndesmotic healing (typically 8-12 weeks for screws, suture buttons often left in situ unless symptomatic). * **Screw Breakage:** If asymptomatic, may leave. If symptomatic or loss of reduction, removal of fragments and revision fixation. * **Loss of Reduction/Migration:** Revision surgery with careful re-reduction and new fixation. |
| **8. Peroneal Tendon Issues (Tendinitis, Subluxation, Rupture)** | Occasional, particularly with reconstruction involving tendon grafts near the fibular groove |
**Management:**
* **Tendinitis:** Rest, NSAIDs, physical therapy. * **Subluxation/Rupture:** Surgical repair/reconstruction of the superior peroneal retinaculum, groove deepening, or tendon repair/debridement. Avoid over-tensioning of the lateral repair that might impinge the peroneal tendons. |
| **9. Over-Constriction / Varus Deformity** | Rare, due to excessive tightening of repair/reconstruction | **Management:** Can lead to stiffness and pain. Prevention is key: position ankle in slight dorsiflexion and neutral/slight eversion during tensioning. Revision surgery for loosening the repair/reconstruction may be necessary if severe. |
| **10. Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE)** | <1% (low risk in foot/ankle surgery, but serious) | **Management:** Standard DVT prophylaxis (pharmacologic, mechanical) according to institutional guidelines. Early mobilization. Diagnosis with ultrasound/CT angiogram. Treatment with anticoagulation. |
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is paramount for optimizing outcomes, restoring function, and minimizing recurrence after ankle ligament surgery. The protocol must be tailored to the specific surgical procedure, individual patient factors (age, activity level, tissue healing potential), and the presence of concomitant procedures. The following outlines a general framework for a modified Broström-Gould repair.
Phase I: Protection & Early Motion (Weeks 0-2/3)
Goals: Protect the repair, reduce pain and swelling, initiate gentle ROM, maintain strength in uninvolved joints.
-
Immobilization:
- Week 0-1: Posterior splint or bulky soft dressing, non-weight bearing (NWB) with crutches.
- Week 1-2/3: Transition to a removable walking boot (CAM walker) or hinged ankle brace. Continue NWB or touch-down weight bearing (TDWB) initially.
- Pain & Swelling Management: RICE protocol (Rest, Ice, Compression, Elevation). NSAIDs.
-
Range of Motion (ROM):
- Gentle, pain-free active and passive dorsiflexion and plantarflexion (within protective range).
- Avoid inversion and eversion stress on the repair.
- Toe flexion/extension exercises.
-
Strength:
- Isometric exercises for quadriceps, hamstrings, and gluteal muscles.
- Core strengthening.
- Ankle pumping (calf muscle activation without stressing repair) to promote circulation and reduce swelling.
- Weight Bearing: Progression from NWB to TDWB/partial weight bearing (PWB) as tolerated, typically starting around week 2-3, depending on surgeon preference and healing status.
Phase II: Progressive Loading & Strengthening (Weeks 3-6/8)
Goals: Restore full pain-free ROM, progressive weight bearing, initiate strengthening and proprioceptive training.
- Immobilization: Continue use of walking boot or hinged ankle brace for protection during ambulation. Gradually decrease reliance on crutches as weight bearing progresses.
- Weight Bearing: Progress from PWB to full weight bearing (FWB) over 2-3 weeks, guided by pain and swelling.
-
Range of Motion (ROM):
- Continue active and passive dorsiflexion/plantarflexion.
- Gentle, progressive inversion/eversion ROM, ensuring no stress on the repair site.
- Manual therapy (joint mobilizations) by a physical therapist to address any stiffness.
-
Strength:
- Begin isometric exercises for ankle invertors, evertors, dorsiflexors, and plantarflexors in pain-free ranges.
- Progress to resisted exercises using resistance bands (e.g., Theraband) for all ankle musculature.
- Calf raises (bilateral, then unilateral) when FWB is achieved.
-
Proprioception:
- Begin basic balance exercises in a protected environment (e.g., seated on a wobble board, single-leg stance with support).
- Gradually progress to unsupported single-leg stance.
- Gait Training: Focus on normal heel-to-toe gait pattern.
Phase III: Advanced Strengthening & Return to Activity (Weeks 6/8 - 12+)
Goals: Achieve full strength and ROM, advanced proprioception, initiation of sport-specific drills, preparing for return to sport/activity.
- Bracing: Discontinue walking boot. Transition to a lace-up ankle brace or supportive athletic shoe for activity.
-
Strength:
- Continue progressive resistance exercises.
- Introduce functional strength exercises: step-ups, lunges, squats.
- Plyometric exercises (light hopping, jumping) when adequate strength is achieved and pain-free.
-
Proprioception:
- Advanced balance training: dynamic balance board, bosu ball, single-leg stance with perturbations.
- Agility drills: cone drills, figure-8s, carioca.
- Sport-specific drills (e.g., throwing, catching while balancing).
- Cardiovascular Fitness: Swimming, cycling, elliptical.
- Return to Activity: Gradual introduction of impact activities and sport-specific training.
Phase IV: Maintenance & Prevention (Months 3-6+)
Goals: Maintain strength and stability, gradual return to full competitive activity, injury prevention.
- Training: Continue strengthening and proprioceptive exercises regularly.
- Sport-Specific Training: Full integration into sport-specific training, emphasizing cutting, jumping, and landing mechanics.
- Bracing/Taping: Consider prophylactic bracing or taping for high-risk activities or competitive sports, especially during the initial return.
-
Return to Sport Criteria:
- Full pain-free ROM.
- Strength symmetrical to contralateral side (isokinetic testing if available).
- Excellent balance and proprioceptive control.
- Successful completion of sport-specific functional testing.
- Patient confidence.
- Typical return to competitive sports 4-6 months post-surgery, though this can vary.
Key Considerations for Rehabilitation:
*
Individualization:
Protocols should be customized.
*
Pain as a Guide:
Progress should be pain-free.
*
Supervised PT:
Essential for proper technique, progression, and early identification of issues.
*
Home Exercise Program:
Critical for consistency.
*
Concomitant Procedures:
Protocols must be modified for osteochondral lesions (more protected weight bearing), syndesmotic repairs, or peroneal tendon repairs.
Summary of Key Literature / Guidelines
The evidence base for the management of ankle sprains and chronic ankle instability has evolved significantly, guiding clinical practice towards evidence-based decision-making.
Conservative vs. Surgical Management for Acute Ankle Sprains
- Literature Consensus: The overwhelming majority of acute ankle sprains (Grade I and II) are successfully managed non-operatively with early functional rehabilitation. Randomized controlled trials (RCTs) and systematic reviews have generally shown no long-term benefit of acute surgical repair over comprehensive non-operative treatment for isolated Grade I or II lateral ankle sprains regarding pain, stability, or return to activity.
- Grade III Sprains: For acute Grade III lateral ankle sprains, while some surgeons may advocate for primary repair in elite athletes to potentially accelerate return to sport or reduce recurrence, high-quality evidence supporting superior outcomes over structured conservative care remains limited and controversial. Non-operative management with immobilization followed by progressive rehabilitation is typically recommended.
Management of Chronic Ankle Instability (CAI)
- Initial Non-Operative Management: A cornerstone of CAI management. Studies consistently demonstrate that a structured physical therapy program, emphasizing neuromuscular control, proprioceptive training, and strengthening of evertor muscles, should be the first line of treatment. A 3-6 month trial is typically recommended.
-
Surgical Indications for CAI:
Failure of comprehensive non-operative management is the primary indication for surgery.
- Modified Broström-Gould Repair: This remains the gold standard for anatomical repair of lateral ankle instability when good quality native ligament tissue is present. Numerous studies report excellent short-to-mid-term outcomes, with high rates of patient satisfaction (85-95% good-to-excellent results) and return to sport. Recurrence rates are generally low (5-15%).
- Anatomic Ligament Reconstruction (Autograft/Allograft): Indicated for cases with poor tissue quality, generalized ligamentous laxity, failed previous repair, or revision surgery. Studies have shown comparable outcomes to Broström repair in appropriate patient populations, providing robust stability. While longer follow-up and larger comparative studies are always beneficial, the use of hamstring autografts (gracilis, semitendinosus) has gained favor due to their strength and reduced donor site morbidity compared to other historical non-anatomical reconstructions (e.g., Watson-Jones, Chrisman-Snook, Elmslie).
- Arthroscopic-Assisted Repair/Reconstruction: Increasingly utilized, allowing for simultaneous treatment of concomitant intra-articular pathologies (osteochondral lesions, impingement) and potentially reducing surgical morbidity. Outcomes appear comparable to open techniques, but the learning curve and technical demands are higher.
Role of Associated Pathologies
- Concomitant Lesions: The prevalence of associated intra-articular pathologies (e.g., osteochondral lesions of the talus, synovitis, impingement, peroneal tendon tears) in patients with CAI is significant (up to 50-70%). The literature strongly supports addressing these lesions concurrently during instability surgery, as they can be a source of persistent pain or contribute to functional limitations. Pre-operative MRI is crucial for identifying these pathologies.
Syndesmotic Injuries
- Acute Unstable Syndesmosis: Surgical stabilization (with screw or suture button fixation) is generally indicated for unstable syndesmotic injuries, particularly when associated with ankle fractures requiring fixation. The use of a suture button device (e.g., TightRope) has gained popularity due to its dynamic nature, potentially allowing for earlier weight bearing and potentially negating hardware removal, with emerging literature supporting non-inferior outcomes to screw fixation.
- Isolated Syndesmotic Sprains: Stable injuries are managed conservatively. Unstable injuries, especially those refractory to conservative care or with persistent diastasis on stress radiographs, may benefit from stabilization.
Outcome Measures
- Functional Scores: Validated outcome measures such as the American Orthopaedic Foot & Ankle Society (AOFAS) Ankle-Hindfoot Score, Foot and Ankle Ability Measure (FAAM), and the Chronic Ankle Instability Tool (CAIT) are commonly used to assess patient-reported outcomes, function, and stability post-operatively.
- Return to Sport: High rates of return to sport (80-90%) are generally reported after successful surgical stabilization for CAI, though return to pre-injury performance levels may vary.
Future Directions
Research continues to focus on refining minimally invasive techniques, exploring biologic augmentation (e.g., PRP, bone marrow aspirate), optimizing graft choices and fixation methods for reconstruction, and improving long-term outcomes and prevention strategies. The role of dynamic assessment of instability and personalized rehabilitation approaches are also areas of ongoing investigation.
You Might Also Like