Operative Management of Tendinitis and Bursitis: A Comprehensive Surgical Guide
Key Takeaway
Tendinitis and bursitis frequently result from repetitive mechanical overload, anatomic malalignment, or inflammatory arthropathies. While conservative modalities like targeted physical therapy, orthotics, and corticosteroid injections resolve most cases, refractory or septic presentations necessitate surgical intervention. Operative management ranges from minimally invasive aspiration to formal open excision and drainage. This guide details the biomechanical principles, diagnostic criteria, and step-by-step surgical techniques required for optimal outcomes in complex bursal and tendinous pathologies.
PATHOPHYSIOLOGY AND CLINICAL EVALUATION
In the comprehensive evaluation of patients presenting with tendinitis and bursitis of the lower extremity, a meticulous history detailing occupational demands, biomechanical stressors, and exercise routines is paramount. The etiology is frequently rooted in mechanical overload: overuse (repetitive, submaximal activity) or acute overload (sudden, unaccustomed increases in activity intensity). These forces induce microtearing within the tendinous architecture, leading to a cascade of mucoid degeneration, neovascularization, and chronic tendinopathy.
Mechanical abnormalities play a critical role in the pathogenesis of these conditions. Leg-length discrepancies, coronal or sagittal plane malalignment, and foot pathomechanics (e.g., excessive subtalar pronation or rigid supination) alter the kinetic chain, placing asymmetrical stress on tendinous insertions and adjacent bursae.
Conservative management remains the cornerstone of initial treatment. Most cases of aseptic tendinitis and bursitis respond favorably to relative rest, cryotherapy, compressive Neoprene sleeves, nonsteroidal anti-inflammatory drugs (NSAIDs), and ergonomic modifications. Biomechanical deficits should be addressed with properly fitted, custom orthotics to neutralize abnormal foot mechanics. Furthermore, muscular imbalances require targeted physical therapy focusing on eccentric strengthening and dynamic flexibility protocols.
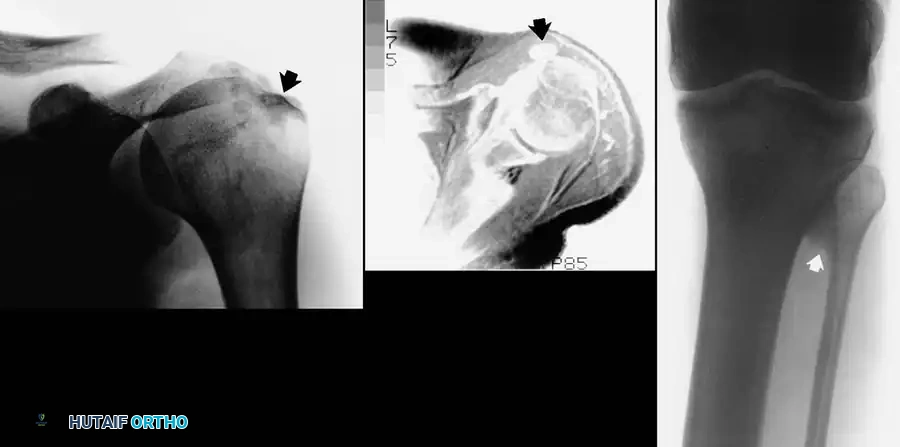
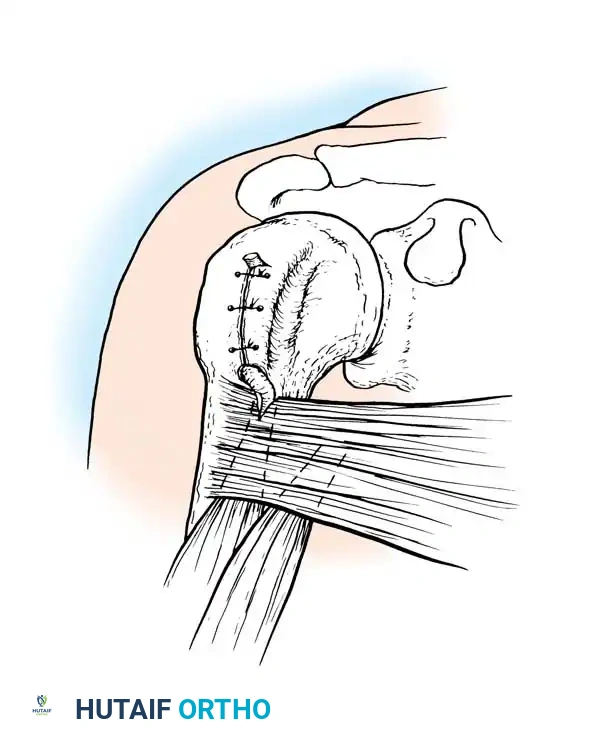
Fig. 24-7: (A) Painful calcification of the anterior deltoid. (B) MRI demonstrating localization of the calcium deposit in the deltoid muscle. (C) Calcification of the proximal tibiofibular articulation resulting in peroneal nerve entrapment in a professional athlete.
ANATOMY AND CLASSIFICATION OF BURSAE
Bursae are specialized, flattened sacs lined with a synovial-like membrane. They are strategically located throughout the musculoskeletal system—typically periarticular or where skin, tendon, or muscle glides over a bony prominence. Their primary biomechanical function is to attenuate friction and protect delicate neurovascular and tendinous structures from compressive and shear forces.
The human body contains over 140 bursae, which are broadly classified into two distinct categories:
1. Anatomical (Innate) Bursae: Naturally occurring bursae present from birth, such as the prepatellar, olecranon, and trochanteric bursae. These possess a true endothelial and synovial lining.
2. Adventitious Bursae: Acquired bursae that develop in response to chronic, repeated trauma, constant friction, or abnormal pressure. Common sites include over a hallux valgus deformity (bunion), an osteochondroma, or a spinal kyphosis.
Pathoanatomic Pearl: Histological studies by Kuhns demonstrated that adventitious bursae lack a true endothelial or synovial lining. However, they are subject to the identical pathological changes seen in innate bursae, including pyogenic infection, villous hypertrophy, fibrotic thickening, and tumorous transformation. Because adventitious bursae develop thick, fibrous walls, they are highly susceptible to chronic inflammatory changes.
Bursae and tendon sheaths share similar histological profiles and are vulnerable to the same pathological disturbances:
* Acute or Chronic Trauma: Direct contusions or repetitive microtrauma.
* Pyogenic Infection: Direct inoculation or hematogenous seeding (e.g., Staphylococcus aureus).
* Systemic Inflammatory Conditions: Gout, pseudogout, rheumatoid arthritis, tuberculosis, or syphilis.
GENERAL PRINCIPLES OF SURGICAL MANAGEMENT
Surgical intervention for bursitis is dictated primarily by the underlying etiology and secondarily by the morphological changes within the bursa. In the vast majority of cases, surgery is not required. Systemic drivers (e.g., inflammatory arthropathies) must be medically optimized, and local mechanical irritants must be eliminated.
When conservative measures—including rest, moist heat, protective padding, and immobilization—fail, or when acute suppuration is present, surgical intervention becomes necessary. The primary surgical modalities include:
1. Aspiration and Injection: Diagnostic fluid analysis and therapeutic corticosteroid injection (strictly contraindicated if infection is suspected).
2. Incision and Drainage (I&D): Indicated for acute suppurative bursitis refractory to serial aspiration and systemic antibiotics.
3. Excision (Bursectomy): Indicated for chronically infected, fibrotic, and thickened bursae that cause persistent mechanical symptoms.
4. Resection of Underlying Prominence: Removal of the mechanical trigger (e.g., exostectomy for an osteochondroma or bunionectomy) combined with bursectomy.
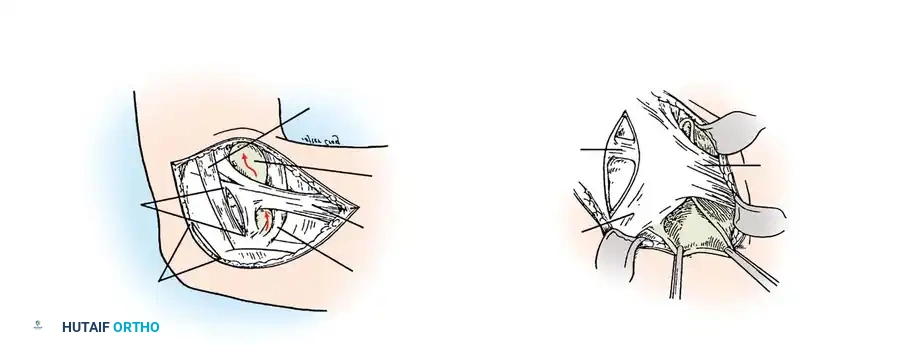
Surgical exposure demonstrating the critical neurovascular boundaries during deep bursal excision.
PATHOLOGIES OF THE KNEE
The knee joint is surrounded by a complex network of bursae, making it highly susceptible to both traumatic and inflammatory bursitis.
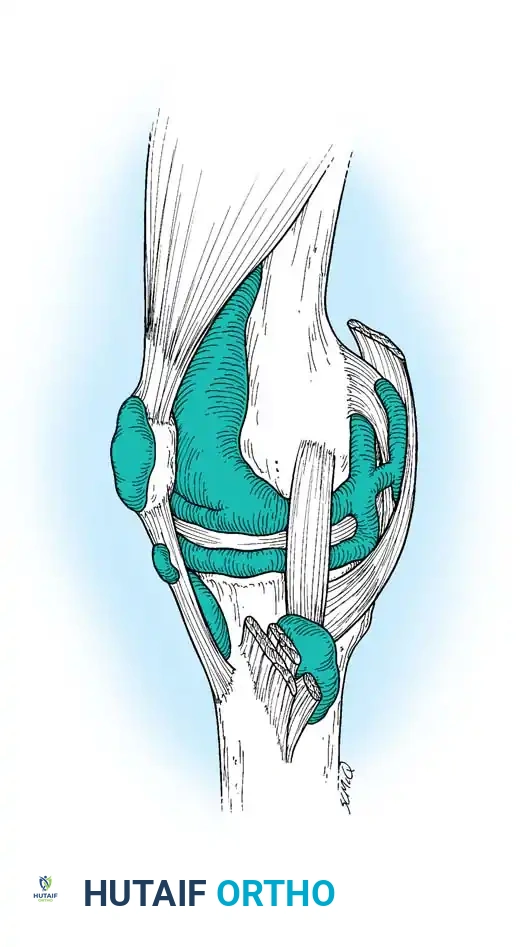
Fig. 24-8: Multiple bursae around the knee that may become acutely or chronically inflamed, including the prepatellar, superficial and deep infrapatellar, and pes anserine bursae.
Prepatellar Bursitis
Traumatic prepatellar bursitis, historically termed "housemaid’s knee," arises from acute direct trauma (e.g., a fall onto the patella) or recurrent minor frictional injuries from prolonged kneeling. While conservative management is usually successful, chronic cases may develop severe fibrosis, synovial thickening, and painful intrabursal nodules (rice bodies), necessitating formal excision.
Pyogenic prepatellar bursitis is particularly common in pediatric and immunocompromised populations. Massive bursal distension can mimic septic arthritis of the knee.
Diagnostic Warning: To differentiate septic prepatellar bursitis from septic arthritis, assess the knee's range of motion. In isolated bursitis, gentle, short-arc joint motion is relatively painless, whereas in septic arthritis, any micromotion of the joint elicits severe pain and guarding.
Septic prepatellar bursitis initially warrants daily needle aspirations, strict immobilization, and targeted intravenous antibiotics. If clinical improvement is not evident within 36 to 48 hours, prompt surgical incision and drainage are mandatory.
🔪 Surgical Technique: Drainage of Prepatellar Bursa
Indications: Acute suppurative prepatellar bursitis failing nonoperative management.
Positioning: Supine. A tourniquet may be applied but is often unnecessary for simple drainage.
- Approach: Utilize either two longitudinal incisions (one medial and one lateral to the bursa) or a single transverse incision centered over the fluctuant mass.
- Evacuation: Incise the bursal sac sharply. Evacuate all purulent material and send immediate swabs for aerobic, anaerobic, and acid-fast bacilli (AFB) cultures.
- Debridement: Break up any loculations within the bursa using a blunt hemostat or gloved finger. Copiously irrigate the cavity with sterile saline.
- Closure/Packing: Do not close the wound primarily. Pack the cavity loosely with petrolatum gauze or iodoform gauze, or place a passive drain (e.g., Penrose) to allow continuous egress of fluid.
Postoperative Protocol:
The extremity is immobilized in a posterior splint to prevent skin tension and mechanical pumping of the infection. Intravenous antibiotics are continued based on culture sensitivities. Packing is changed at least twice weekly. Immobilization is maintained until the sinus tract heals completely by secondary intention.
Intraoperative view of prepatellar bursa excision, demonstrating the thick, fibrotic walls characteristic of chronic inflammation.
🔪 Surgical Technique: Excision of Prepatellar Bursa (Bursectomy)
Indications: Chronic, fibrotic prepatellar bursitis with painful nodules or recurrent sterile effusions.
Positioning: Supine with a proximal thigh tourniquet.
- Incision: Make a transverse incision of appropriate length centered directly over the bursa. Transverse incisions heal with superior cosmesis and less tension over the extensor mechanism compared to longitudinal incisions.
- Dissection: Carefully dissect the bursal sac from the overlying skin and subcutaneous tissue. Maintain a meticulous plane to avoid devascularizing the skin flaps.
- Deep Resection: Dissect the deep surface of the bursa off the underlying patellar aponeurosis. Attempt to excise the bursa en bloc without rupturing it, though this may be impossible in acute serous effusions.
- Hemostasis and Dead Space Management: Deflate the tourniquet and obtain absolute hemostasis. The most common complication of superficial bursectomy is postoperative hematoma formation.
- Closure: Trim redundant skin. Obliterate the dead space using closed-suction drainage or by placing deep mattress sutures through the skin and underlying aponeurosis, tied over large buttons (as described by Breck and Higinbotham).
Postoperative Protocol:
Apply a bulky, compressive Jones dressing. Immobilize the knee in full extension for 2 weeks to allow skin flap adherence and prevent hematoma. Quadriceps-setting exercises are initiated on postoperative day one.
Tibial Collateral Ligament Fibrositis and Bursitis
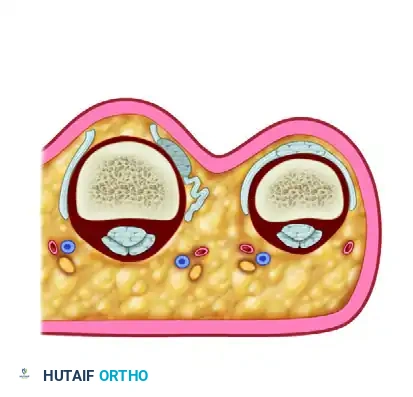
Voshell and Brantigan identified a complex of bursae located between the longitudinal fibers of the medial collateral ligament (MCL) and the deep knee capsule. Up to three distinct bursae can exist beneath the ligament in a single knee.
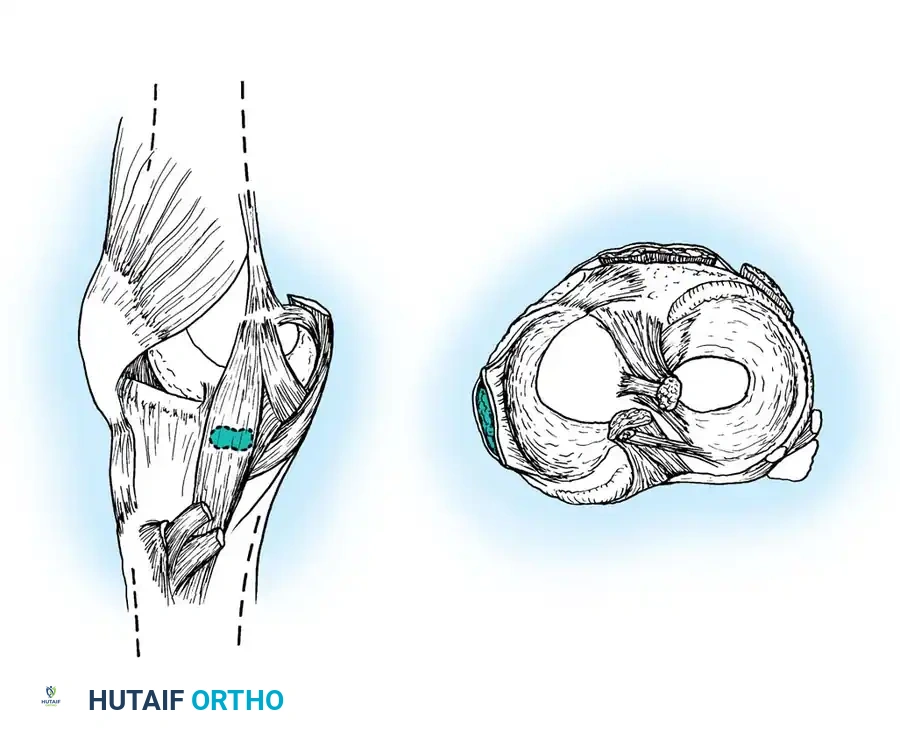
Fig. 24-9: Voshell bursa located just below the joint line, situated between the superficial tibial collateral ligament and the deep joint capsule.
Pathology in this region often presents as medial joint line pain, mimicking a medial meniscus tear. However, mechanical symptoms (catching, locking) are absent. Calcification within these bursae may be radiographically identical to Pellegrini-Stieda disease.
Diagnostic Imaging: MRI is the gold standard for refractory cases. Tibial collateral ligament bursitis presents with a characteristic fluid signal deep to the MCL, forming an inverted "U" shape.
Management: Most cases respond to localized corticosteroid injections. In a series by Kerlan and Glousman, 62% of patients achieved resolution with injection and early functional rehabilitation. If symptoms persist, arthroscopy or MRI is indicated to rule out intra-articular derangement or medial tibial plateau stress fractures.
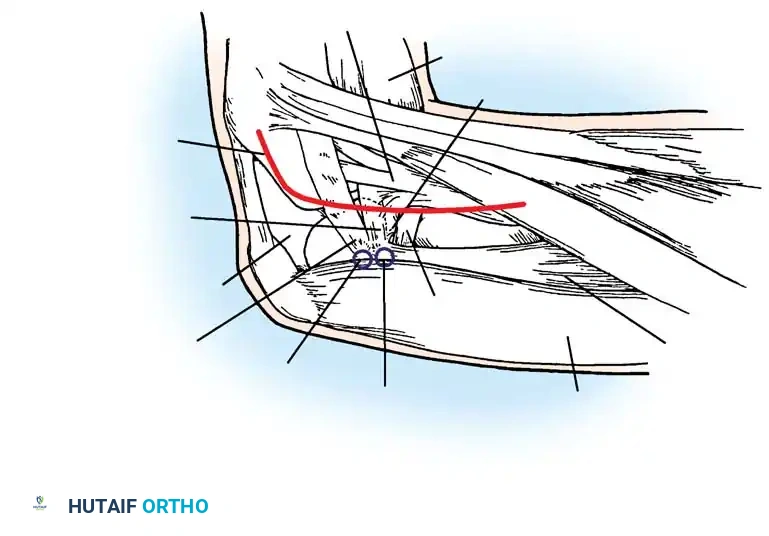
Fibular Collateral Ligament Bursitis
Described by Hendryson, this bursa lies beneath, anterior, or posterior to the fibular collateral ligament (LCL). Distension produces a localized, tender swelling on the lateral aspect of the knee, ranging from 0.6 to 2.5 cm in diameter.
Anatomical dissection highlighting the lateral ligamentous complex and the typical location of the fibular collateral ligament bursa.
Differential Diagnosis:
* Cyst of the lateral meniscus
* Biceps femoris tendinitis
* Partial biceps avulsion (presents with pain and popping at 30–45 degrees of flexion)
* Posterolateral corner instability
Management: Varus stress testing is typically painful. If no discrete mass is palpable, local anesthetic and corticosteroid injection is curative. If a distinct, persistent mass is present, formal surgical excision is required.
Infrapatellar Bursitis
The deep infrapatellar bursa is situated between the tibial tubercle and the posterior aspect of the patellar tendon, separated from the knee joint synovium by Hoffa's fat pad. Distension obliterates the normal depressions on either side of the patellar tendon.
Sagittal representation of the deep infrapatellar bursa and its relationship to the patellar tendon and Hoffa's fat pad.
Clinical Pitfall: According to Waters and Kasser, deep infrapatellar bursal infections closely mimic septic arthritis or proximal tibial osteomyelitis. Patients present with a loss of full extension, resistance to flexion, and exquisite tenderness over the patellar ligament.
Management: Careful aspiration is mandatory, ensuring the needle does not penetrate the deep capsule into the knee joint. If purulence is identified, immediate open drainage via a small medial parapatellar incision is indicated. The proximal tibial metaphysis must be evaluated radiographically for concomitant osteomyelitis.
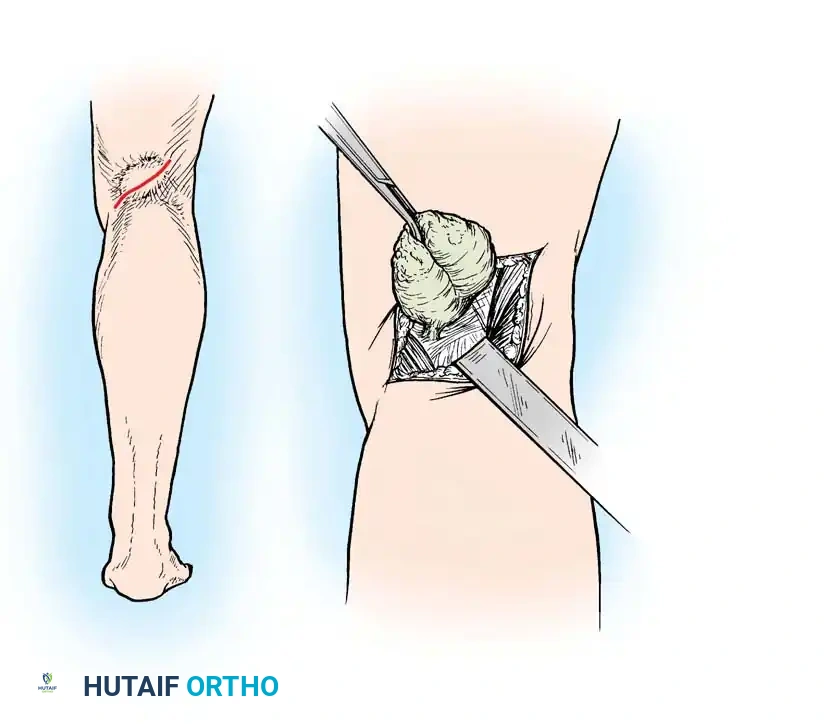
Popliteal Cyst (Baker's Cyst)
Originally described by Adams in 1840 and later popularized by Baker in 1877, a popliteal cyst is typically a distension of the gastrocnemio-semimembranosus bursa. This bursa naturally communicates with the knee joint in a significant percentage of the population.
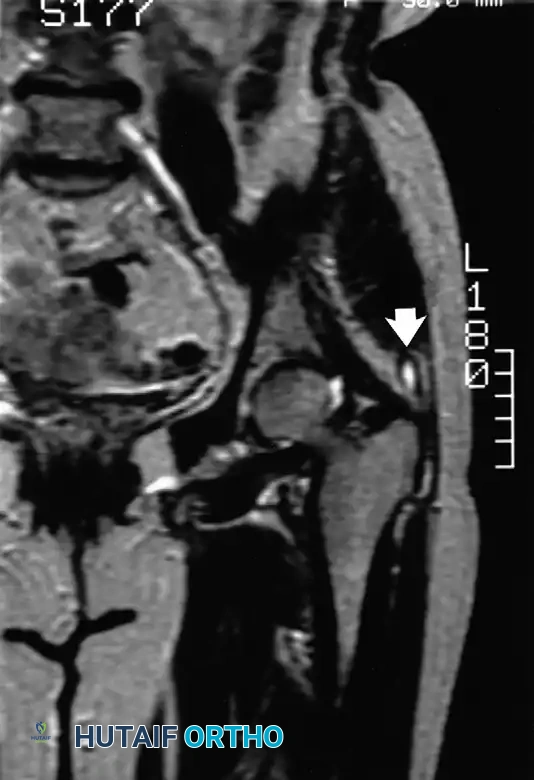
Posterior approach to the popliteal fossa for excision of a complex, multiloculated Baker's cyst.
Pathogenesis:
Meyerding and Van Demark established that these cysts arise either from direct herniation of the posterior synovial capsule or, more commonly, via a one-way valve mechanism allowing synovial fluid to escape from the knee joint into the bursa during flexion, preventing its return.
Pediatric vs. Adult Presentations:
Touloukian and Malloch highlighted critical differences in management based on patient age:
* Children: The cyst rarely communicates with the joint, and intra-articular pathology is exceptionally rare. The vast majority resolve spontaneously with benign neglect. Surgical excision is reserved for massive, symptomatic cysts causing neurovascular compression.
* Adults: Popliteal cysts in adults are almost universally (98%) secondary to intra-articular pathology, most commonly posterior horn medial meniscus tears or advanced osteoarthritis.
Surgical Management in Adults:
Treating the cyst without addressing the intra-articular pathology guarantees recurrence. Management should focus on arthroscopic debridement or repair of the offending meniscal tear and management of chondral defects. The cyst itself rarely requires open posterior excision unless it is massive, multiloculated, or causing compressive neuropathy of the tibial nerve. If open excision is performed, the stalk communicating with the joint capsule must be meticulously dissected, ligated, and the capsular defect closed to prevent synovial fluid extravasation.
===
You Might Also Like