Traumatic Extensor Tendon Dislocation Repair Guide
Key Takeaway
Traumatic dislocation of the extensor tendon at the metacarpophalangeal joint typically results from radial sagittal band rupture. Surgical management involves centralizing the tendon via direct repair, local tissue flaps, or tendon routing techniques like the Carroll procedure. Precise tensioning and postoperative dynamic splinting are critical to restore biomechanical balance, prevent ulnar subluxation, and ensure optimal functional recovery in the affected digit.
INTRODUCTION TO EXTENSOR TENDON DISLOCATION
Traumatic dislocation of the extensor tendon at the level of the metacarpophalangeal (MCP) joint is a debilitating injury that disrupts the delicate biomechanical balance of the hand. Commonly referred to as "boxer's knuckle" when sustained during closed-fist trauma, this pathology predominantly involves the rupture, attenuation, or elongation of the radial sagittal band. Because the radial sagittal band is inherently thinner and longer than its ulnar counterpart, forceful flexion or blunt trauma to the MCP joint frequently results in its failure, leading to the ulnar subluxation or frank dislocation of the extensor digitorum communis (EDC) tendon into the intermetacarpal valley.
Surgical intervention is indicated for acute dislocations that fail conservative management (extension splinting) and for chronic, symptomatic subluxations that impair active extension. The primary surgical objective is to recentralize the extensor tendon over the metacarpal head, restore the integrity of the extensor hood, and permit early protected mobilization to prevent adhesions.
SURGICAL ANATOMY AND BIOMECHANICS
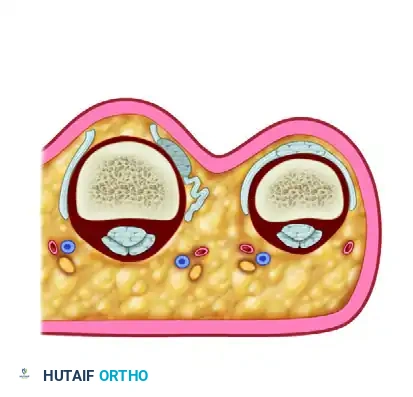
The extensor mechanism at the MCP joint is a complex aponeurotic expansion. The EDC tendon is stabilized centrally over the metacarpal head by a sling-like structure composed of the transverse sagittal bands. These bands originate from the volar plate and the deep transverse metacarpal ligament, enveloping the EDC tendon and inserting into its lateral margins.
When the radial sagittal band ruptures, the unopposed pull of the intact ulnar sagittal band, combined with the natural ulnar deviation of the digits during power grip, forces the EDC tendon to subluxate ulnarly. This mechanical shift alters the vector of the extensor tendon, converting it from an extensor of the MCP joint to a paradoxical flexor if the tendon drops below the axis of rotation.
💡 Clinical Pearl: Anesthesia and Active Testing
The use of Wide Awake Local Anesthesia No Tourniquet (WALANT) or an intravenous regional block is highly recommended. Local infiltration allows the patient to attempt active extension of the finger intraoperatively before wound closure. This dynamic testing is invaluable to ensure that the extensor tendon remains perfectly centralized under physiological tension and that the repair is robust enough to withstand early rehabilitation.
SURGICAL APPROACH AND PATHOANATOMY IDENTIFICATION
Patient Positioning and Preparation
The patient is positioned supine with the operative arm extended on a radiolucent hand table. If WALANT is not utilized, a well-padded upper arm tourniquet is applied. The hand is prepped and draped in a standard sterile fashion.
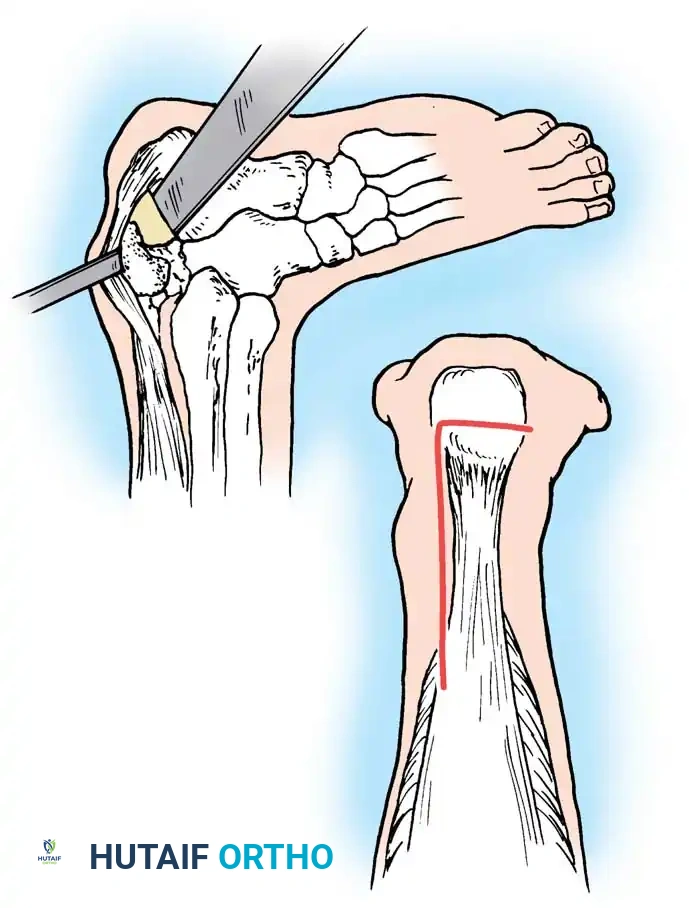
Incision and Exposure
- Make a curved or lazy-S incision on the radial side of the affected metacarpophalangeal joint. This avoids a straight dorsal scar, which is prone to contracture and can tether the underlying tendon.
- Carefully dissect through the subcutaneous tissue, preserving the dorsal sensory branches of the radial or ulnar nerves.
- Expose the dorsal apparatus, the MCP joint capsule, and the subluxating extensor tendon.
Pathoanatomy Assessment
Upon exposure, evaluate the extensor hood. The ulnar sagittal band is frequently contracted due to chronic ulnar displacement of the tendon. The radial sagittal band will appear either frankly ruptured, attenuated, or scarred down to the underlying capsule.
- Step 1: Release the ulnar sagittal band if it is contracted. This is a critical step; failure to release the ulnar tether will place excessive tension on the radial repair, leading to recurrent dislocation.
- Step 2: Assess the radial sagittal band. In some patients, the extensor tendon can be found "shucked" (delaminated) from the dorsum of the sagittal band rather than presenting with a mid-substance tear.
SURGICAL TECHNIQUES FOR TENDON CENTRALIZATION
Depending on the tissue quality and the chronicity of the injury, several methods can be employed to recentralize the extensor tendon.
Technique 1: Direct Repair
If the injury is acute and tissue quality is robust, direct repair of the radial sagittal band may be possible.
- Reapproximate the torn edges of the radial sagittal band using 4-0 nonabsorbable mattress sutures.
- If the tendon is "shucked" from the dorsum of the sagittal band, reattach it to its anatomical bed with three or four 4-0 nonabsorbable sutures.
- Note: Direct repair often requires reinforcement with local tissue flaps if the tissue is friable.
Technique 2: Sagittal Band Slip Reconstruction
When direct repair is tenuous, a local tendon slip can be fashioned to recreate the radial tether.
1. Fashion a narrow slip (3 to 4-mm wide) of the sagittal band vertical fibers.
2. Make vertical parallel incisions from dorsal to palmar on the radial side to create a strip approximately 8 mm long, based dorsally.
3. Pass this slip dorsally through a narrow slit created in the substance of the extensor tendon.
4. Suture the slip back onto itself with two or three 4-0 nonabsorbable sutures, effectively creating a lasso that pulls the tendon radially.
Technique 3: Central Tendon Loop Technique
In cases of severe attenuation, a loop can be created from the central tendon itself.
1. Create a loop by harvesting a 5-cm lateral margin of the central tendon at the level of the MCP joint, leaving the distal insertion of this segment attached.
2. Create a small window with vertical incisions in the superficial portion of the joint capsule.
3. Pass the proximal end of the harvested segment through this capsular window.
4. Suture the proximal end back to the main extensor tendon, creating a stabilizing sling.
Technique 4: The Carroll et al. Reconstruction
For chronic dislocations or severe tissue deficiency, the technique described by Carroll et al. provides a robust, biomechanically sound reconstruction.

- Ulnar Release: Begin by completely releasing the contracted ulnar sagittal band.
- Strip Elevation: Elevate a distally based tendon strip from the ulnar side of the extensor digitorum communis. Make the strip long enough to traverse the joint.
- Routing: Pass this ulnar strip beneath the radial side of the EDC, routing it dorsal to the joint capsule but deep to the radial collateral ligament.
- Fixation: Bring the strip dorsally again and suture it directly to the dorsal aspect of the EDC tendon. The radial collateral ligament acts as a pulley, providing a strong radial vector that perfectly centralizes the tendon.
- Tensioning: Adjustment of tension is essential. The tendon must remain centralized during full passive (or active, if WALANT is used) flexion of the MCP joint without restricting the arc of motion.
⚠️ Surgical Warning: Tensioning Pitfalls
Over-tensioning the radial reconstruction will cause an iatrogenic radial subluxation and severely limit MCP joint flexion. Under-tensioning will result in recurrent ulnar subluxation. Intraoperative dynamic testing is the only reliable method to confirm optimal tension.
POSTOPERATIVE CARE FOR MCP JOINT REPAIRS
Meticulous postoperative rehabilitation is as critical as the surgical execution.
- Immediate Post-Op: Close the wound and apply a volar splint to maintain the finger in slight radial deviation (to prevent ulnar drift) and the MCP joint in full extension for immediate protection and comfort.
- 10 to 14 Days: Sutures are removed.
- 3 to 4 Weeks: If a transarticular Kirschner wire was utilized for temporary stabilization (rarely needed if the repair is robust), it is removed at this stage. Protected motion is initiated.
- Splinting Protocol: A removable volar splint is applied to block MCP joint flexion while leaving the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints free to move. This splint is worn day and night, removed only for controlled exercises three to four times daily.
- 4 to 8 Weeks: Gradual improvement of motion is allowed. The affected finger is buddy-taped to the adjacent radial-side finger to protect the repair from ulnar-deviating forces. Protected motion and splinting are maintained for about 8 weeks, followed by a gradual return to full activities.
COMPREHENSIVE EXTENSOR TENDON REPAIR BY ZONE
While Zone V (MCP joint) injuries frequently involve dislocation, traumatic lacerations across the other extensor zones require specific, tailored approaches due to the varying anatomical constraints and biomechanical demands of the extensor mechanism.
Zone VI: The Metacarpal Region
Zone VI encompasses the area over the metacarpals. Injuries here are often deceptive.
- Clinical Presentation: Wounds should be meticulously explored in patients who cannot hyperextend the MCP joint, even if weak active extension is present. Intact adjacent tendons pulling through the juncturae tendinum, combined with intact extensor indicis proprius (EIP) or extensor digiti minimi (EDM) tendons, can easily conceal a complete transection of an EDC tendon.
- Surgical Technique: Adequate exposure is required, as the proximal stump often retracts. The broad size and diameter of the tendons in Zone VI permit the use of a robust 3-0 or 4-0 core suture (e.g., Becker repair or Kleinert modification of the Bunnell repair), supplemented with a running circumferential epitendinous suture. This multi-strand approach provides sufficient resistance to gap formation while permitting early motion.
- Rehabilitation: Postoperatively, continuous dynamic splinting, or static splinting followed by dynamic splinting, is utilized for 6 to 8 weeks.
Zone VII: The Extensor Retinaculum
Zone VII is located at the wrist, deep to the dorsal carpal ligament (extensor retinaculum). Here, the tendons are ensheathed in six distinct fibro-osseous synovial compartments.
- Surgical Challenges: Lacerated tendons in this zone rapidly retract proximally into the forearm. Extensive incisions may be required for retrieval.
- Retinaculum Management: Accessing the tendons requires elevation or partial resection of the extensor retinaculum. A straightforward removal of the proximal or distal portion of the retinaculum may allow sufficient exposure while preserving enough central retinaculum to prevent bowstringing. Alternatively, the retinaculum can be opened with a Z-lengthening incision, allowing it to be repaired loosely over the swollen, repaired tendons to prevent them from becoming stuck in their canals as they heal.
- Repair and Rehab: Primary repair is performed with a 3-0 or 4-0 core suture and an epitendinous stitch. Postoperatively, splinting the wrist in a position of moderate extension (rather than full hyperextension) helps limit the bowstring effect against the repaired retinaculum.
Zone VIII: The Distal Forearm
Zone VIII represents the distal forearm, proximal to the extensor retinaculum, where the musculotendinous junctions transition into distinct muscle bellies.
- Surgical Technique: Careful dissection is required to match the proximal muscle belly to its corresponding distal tendon. Because the tissue is transitional, standard core sutures will pull through the friable muscle. The tendinous portion must be sutured to the muscle belly using carefully placed 3-0 mattress or figure-of-eight sutures to distribute the load and minimize cut-out.
- Rehabilitation: A volar splint is applied from the elbow to the PIP joints, maintaining the wrist in full extension. This permits maximal relaxation of the musculotendinous unit, which is imperative because muscle-to-muscle or muscle-to-tendon repairs cannot withstand early active tension.
Zone IX: The Proximal Forearm Muscle Bellies
Lacerations in Zone IX involve the thick extensor muscle bellies of the proximal forearm and are frequently associated with major vessel and nerve injuries (e.g., posterior interosseous nerve).
- Surgical Technique: If treated early, the muscle bellies can be reapproximated using several large mattress or figure-of-eight sutures. If the muscle is severely macerated or if primary repair is under excessive tension, tendon grafts (e.g., palmaris longus) may be utilized. The graft is woven through the muscle belly from one side of the laceration to the other to act as an internal splint.
- Rehabilitation: The wrist is held in appropriate extension, and the MCP joints are splinted in approximately 30 degrees of flexion with the PIP joints left free. This static protection is maintained for about 6 weeks to allow the muscle tissue to scar and heal.
Zone T V: The Thumb Compartments
Zone T V includes the first dorsal compartment (Abductor Pollicis Longus [APL] and Extensor Pollicis Brevis [EPB]) and the third dorsal compartment (Extensor Pollicis Longus [EPL]).
- Surgical Considerations: The superficial radial nerve is highly vulnerable in this zone and must be protected. Tendons injured within the first dorsal compartment are usually mobilized and left outside the compartment post-repair to minimize restrictive adhesion formation (De Quervain-like tethering).
- Repair Techniques: Repairs are performed with 3-0 or 4-0 core sutures supplemented with an epitendinous suture.
- Tendon Transfers and Grafts: If the EPL is divided far proximally and heavily retracted, the distal end of the palmaris longus or the EIP can be transferred. Tendon transfer requires only one suture line, whereas a graft requires two. If a graft is necessary to bridge a defect, it should be rerouted subcutaneously, bypassing Lister's tubercle, to avoid mechanical abrasion and subsequent rupture of the graft.
- Rehabilitation: A thumb spica splint is applied with the wrist in near-full extension and the thumb extended and abducted. The splint extends from distal to the elbow to the thumb tip, leaving the ulnar digits free. Immobilization is maintained for 4 weeks, followed by gradual thumb mobilization while keeping the wrist splinted in extension for an additional 4 weeks.
CONCLUSION
The successful management of traumatic extensor tendon dislocations and lacerations requires a profound understanding of hand biomechanics, precise surgical execution, and rigorous adherence to zone-specific rehabilitation protocols. Whether performing a complex Carroll reconstruction for a subluxating sagittal band at the MCP joint or navigating the fibro-osseous canals of the extensor retinaculum, the surgeon's goal remains the restoration of a smooth, gliding, and biomechanically balanced extensor mechanism.
You Might Also Like