Comprehensive Physical Examination and Diagnostic Workup of Elbow Instability
Key Takeaway
The physical examination of the elbow requires a systematic approach to evaluate osseous and ligamentous stabilizers. Key assessments include the moving valgus stress test for medial ulnar collateral ligament (MUCL) competence and the lateral pivot-shift test for posterolateral rotatory instability (PLRI). Accurate diagnosis relies on correlating clinical maneuvers with advanced imaging, such as magnetic resonance arthrography, to identify capsuloligamentous disruptions and guide subsequent surgical intervention.
INTRODUCTION TO ELBOW BIOMECHANICS AND CLINICAL EVALUATION
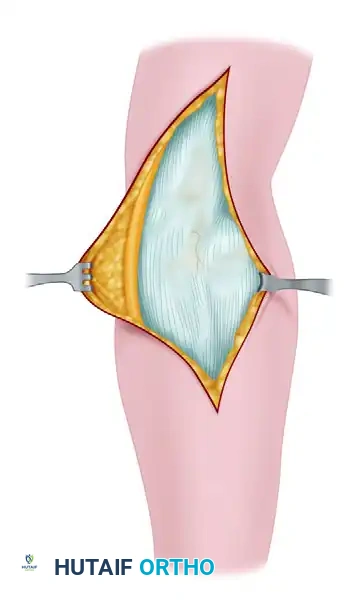
The elbow is a highly constrained, complex hinge joint comprising three distinct articulations: the ulnohumeral, radiocapitellar, and proximal radioulnar joints. Stability is conferred through a precise interplay of static and dynamic restraints. The primary static stabilizers include the ulnohumeral articulation, the medial ulnar collateral ligament (MUCL) complex, and the lateral collateral ligament (LCL) complex. Secondary stabilizers include the radial head, the joint capsule, and the dynamic compression provided by the common flexor-pronator and extensor muscle masses.
A masterful physical examination of the elbow requires a systematic, evidence-based approach to isolate these structures. For the orthopedic surgeon, correlating subtle clinical signs of microinstability or gross ligamentous incompetence with advanced imaging is paramount for formulating an effective operative or non-operative treatment algorithm.
VISUAL INSPECTION AND PALPATION
Examination of the elbow must always begin with a meticulous visual inspection, comparing the affected extremity to the contralateral side. The clinician should assess for gross deformity, muscle atrophy, localized swelling, or ecchymosis, which may indicate acute capsuloligamentous tearing or chronic disuse.
Soft Tissue and Muscle Mass Assessment
The forearm circumference is quantitatively measured exactly 7 cm distal to the medial epicondyle. This measurement is critical in overhead athletes (e.g., baseball pitchers), where hypertrophy of the dominant flexor-pronator mass is expected; an absence of this hypertrophy or measurable atrophy may indicate chronic MUCL insufficiency or a compressive neuropathy.
Joint Effusion and the "Soft Spot"
Intra-articular fluid or hemarthrosis is most reliably detected by palpating the posterolateral "soft spot." This anatomic triangle is bordered by the lateral epicondyle anteriorly, the tip of the olecranon medially, and the radial head distally. Bulging or fluctuance in this interval is a highly sensitive indicator of an elbow effusion, occult fracture (such as a non-displaced radial head fracture), or acute ligamentous injury.
Systematic palpation must then proceed to the flexor-pronator origin, the sublime tubercle (the insertion of the anterior bundle of the MUCL), the lateral epicondyle, the radiocapitellar joint line, and the posteromedial tip of the olecranon.
PATHOANATOMY OF ELBOW INSTABILITY
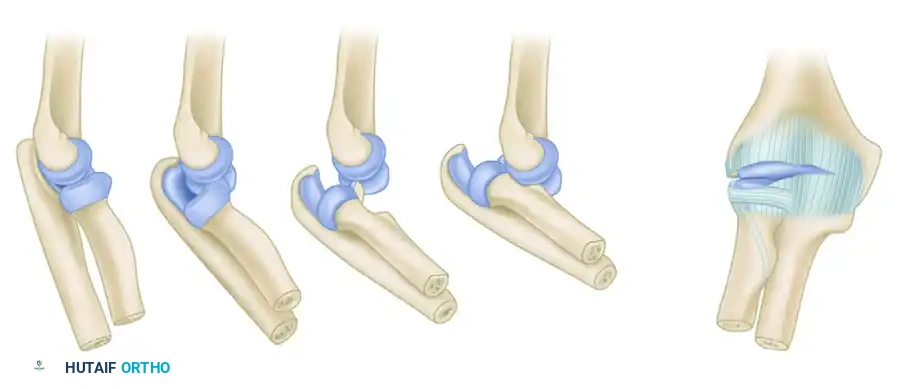
Understanding the physical examination requires a thorough grasp of the pathoanatomy of elbow dislocations. O’Driscoll et al. described a predictable, sequential pattern of soft-tissue disruption that occurs during traumatic elbow subluxation and dislocation, progressing in a circular fashion from lateral to medial.
The O'Driscoll Stages of Instability
- Stage 1 (Posterolateral Rotatory Instability): The injury initiates on the lateral side with the disruption of the ulnar part of the lateral collateral ligament (LUCL). This results in posterolateral rotatory subluxation of the elbow, where the ulna supinates away from the trochlea.
- Stage 2 (Perched Dislocation): As the deforming force continues, the disruption propagates anteriorly and posteriorly, tearing the remaining lateral ligamentous structures and the anterior/posterior joint capsule. The coronoid process becomes "perched" on the trochlea.
- Stage 3 (Complete Dislocation): The injury crosses to the medial side.
- Stage 3A: Involves partial disruption of the MUCL, specifically the posterior band, while the anterior band remains intact. The elbow is dislocated but may be stable to valgus stress in flexion.
- Stage 3B: Complete disruption of the entire MUCL complex, including the critical anterior band. The elbow is grossly unstable in all planes.
Clinical Pearl: Recognizing this lateral-to-medial progression is vital. An elbow that has suffered a traumatic dislocation and subsequently demonstrates medial instability in extension but stability in flexion likely has an intact anterior bundle of the MUCL (Stage 3A), which has profound implications for conservative versus operative management.
EVALUATION OF MEDIAL (VALGUS) INSTABILITY
Medial elbow instability is most commonly seen in overhead throwing athletes due to repetitive valgus overload, or as a sequela of acute trauma. The anterior bundle of the MUCL is the primary restraint to valgus stress from 30 to 120 degrees of flexion.
The Moving Valgus Stress Test
To isolate the MUCL, the moving valgus stress test is performed. The examiner applies a constant valgus torque to the elbow while passively extending the joint from 120 degrees of flexion down to 30 degrees, and then rapidly flexing it back.
* Positive Finding: The generation of medial pain, particularly in the "shear zone" between 70 and 120 degrees of flexion, strongly indicates MUCL incompetence.
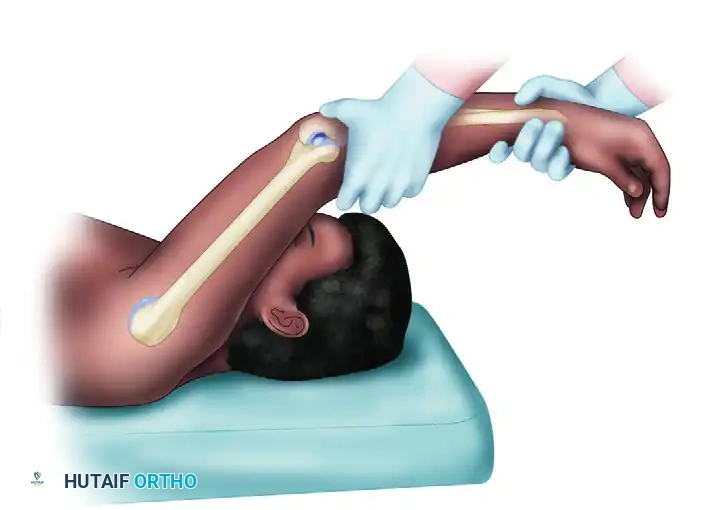
The Milking Maneuver
The milking maneuver is another highly specific test for the anterior bundle of the MUCL.
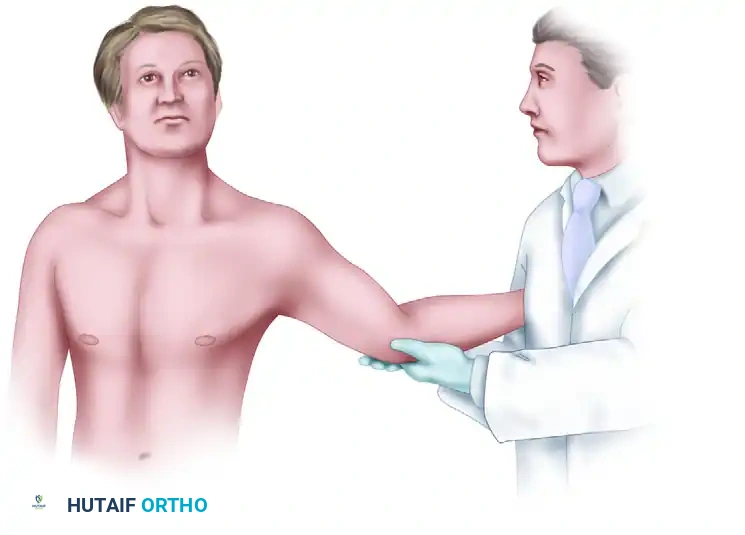
- Technique: The patient's shoulder is abducted and externally rotated. The examiner stabilizes the patient's arm and applies a valgus stress by pulling on the patient’s thumb (simulating a "milking" motion), thereby imparting a valgus vector to the elbow. The elbow is ranged between 30 and 120 degrees.
- Interpretation: Apprehension, medial joint line pain, or palpable gapping indicates a positive test.
Radiocapitellar Compression Assessment
During the evaluation of medial instability, it is crucial to assess the lateral compartment. Chronic valgus laxity often leads to radiocapitellar overload. While applying valgus stress and axial compression, the examiner pronates and supinates the forearm with the elbow in varying degrees of flexion. The production of lateral pain or palpable crepitance is indicative of radiocapitellar chondromalacia secondary to chronic medial incompetence.
EVALUATION OF POSTEROLATERAL ROTATORY INSTABILITY (PLRI)
PLRI is the most common pattern of chronic elbow instability, resulting from insufficiency of the LUCL. Patients typically present with mechanical symptoms—clicking, snapping, or a sense of the elbow "giving way" when pushing off a chair.
The Lateral Pivot-Shift Test of the Elbow
This pathognomonic test reproduces the subluxation and subsequent reduction of the radiocapitellar and ulnohumeral joints.
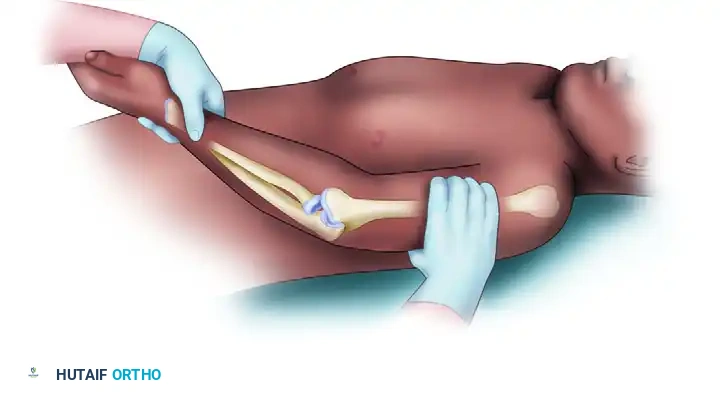
- Technique (Supine): The patient is placed supine with the arm overhead. The examiner grasps the patient's wrist and forearm. Three simultaneous forces are applied:
- Supination of the forearm.
- Valgus moment at the elbow.
- Axial compression along the forearm.
- Execution: While maintaining these forces, the elbow is slowly flexed from a position of full extension.
- Biomechanics of the Test: As the elbow flexes past 20 to 40 degrees, the radius and ulna subluxate posterolaterally away from the humerus. A visible dimple forms in the posterolateral soft spot between the radial head and the capitellum. As flexion continues past 40 degrees, the triceps tension increases, snapping the joint back into a reduced position with a palpable and visible "clunk."
The Overhead Pivot-Shift Variant
To improve mechanical advantage and patient relaxation, the overhead variant is highly effective.
- Technique: The patient's arm is brought fully overhead, and the shoulder is placed in maximum external rotation. This position utilizes the shoulder's capsular tension to provide a rigid counterforce for forearm supination, freeing one of the examiner's hands to precisely control the valgus moment and palpate the radial head. The elbow is moved from extension to flexion, reproducing the subluxation at 40 degrees and the reduction clunk at deeper flexion angles.
Surgical Warning: The pivot-shift test is often difficult to elicit in an awake patient due to muscular guarding. A positive apprehension sign (the patient resisting further movement and reporting a feeling of impending dislocation) is considered a clinically positive test. Definitive confirmation is often performed under anesthesia prior to surgical reconstruction.
Active Provocative Tests for PLRI
To reproduce functional instability in the clinic, active tests are utilized:
* Table/Seat Press-Up Test: The patient attempts to push themselves up from a chair using the armrests, with the forearms in maximum supination. This naturally applies axial load, valgus stress, and supination. Pain or a feeling of instability is a positive sign.
* Wall or Floor Push-Up Test: The patient performs a push-up against a wall or the floor with the hands positioned in supination. The examiner observes for radial head subluxation or patient apprehension.
NEUROLOGICAL EXAMINATION: THE ULNAR NERVE
The ulnar nerve is intimately associated with the medial ligamentous structures and is frequently implicated in elbow pathology, either through traction injuries (in valgus instability) or direct compression (cubital tunnel syndrome).
- Positioning: The patient is placed prone or seated. The shoulder is abducted to 90 degrees, and the elbow is flexed to 90 degrees.
- Tinel's Sign: Gentle percussion over the cubital tunnel is performed to elicit paresthesias in the ulnar nerve distribution (ring and small fingers).
- Dynamic Subluxation: The examiner passively ranges the elbow from extension to full flexion while palpating the nerve posterior to the medial epicondyle. The nerve is evaluated to determine if it subluxes or completely dislocates anteriorly over the medial epicondyle. Manual stress can also be applied to assess the stability of the nerve within its groove.
Pitfall: Failure to identify a hypermobile ulnar nerve preoperatively can lead to iatrogenic injury during MUCL reconstruction or lateral collateral ligament repairs. If the nerve is unstable, a concurrent ulnar nerve transposition may be indicated during ligamentous reconstruction.
ADVANCED DIAGNOSTIC IMAGING
While the physical examination provides the functional diagnosis, precise radiographic evaluation is mandatory to assess osseous architecture, identify avulsion fractures, and quantify ligamentous damage.
Standard Radiography
- Standard Views: Anteroposterior (AP) and lateral radiographs are standard.
- Oblique Views: Two 45-degree oblique views (internal and external rotation) are critical for evaluating the radiocapitellar joint (for occult radial head fractures or capitellar osteochondritis dissecans) and the trochlear joint.
- The Drop Sign: On a true lateral radiograph, an increase in the ulnohumeral distance (widening of the joint space >3 mm) is known as the "drop sign." This represents significant capsuloligamentous disruption and persistent subluxation, often necessitating surgical intervention.
- The Jones View: In overhead athletes with chronic medial symptoms, an acute flexion AP view (Jones view) is indicated. This view profiles the posteromedial compartment to identify posteromedial olecranon osteophytes, a hallmark of Valgus Extension Overload (VEO) syndrome.
Stress Radiography
- Gravity Stress Radiograph: This test is utilized to objectively quantify medial instability. The patient is positioned supine with the shoulder abducted 90 degrees and externally rotated. The forearm is fully supinated, and the elbow is flexed 20 to 30 degrees to unlock the olecranon from its fossa. An AP radiograph is taken. Gravity applies a valgus stress to the joint. Opening of the medial joint space compared to the contralateral side indicates significant MUCL injury. While highly specific, it is not highly sensitive for partial tears.
Advanced Cross-Sectional Imaging
- Magnetic Resonance Imaging (MRI) and MR Arthrography (MRA): Gadolinium-enhanced MRI or CT arthrography is the gold standard for evaluating the integrity of the MUCL and LUCL complexes.
- The "T-Sign": Described by Timmerman and Andrews, the T-sign is a pathognomonic finding on an MR arthrogram. It represents a leak of contrast material medial to the sublime tubercle, extending between the MUCL and the bone, without extracapsular leakage. This indicates a partial, undersurface avulsion of the MUCL from its ulnar insertion—a lesion that frequently fails conservative management in elite throwers.
- Dynamic Ultrasound: High-resolution diagnostic ultrasound is increasingly utilized in specialized centers. It allows for dynamic, real-time evaluation of the MUCL under valgus stress, measuring joint gapping in millimeters. It is also excellent for assessing ulnar nerve subluxation. However, MRI remains superior for the comprehensive visualization of concomitant intra-articular pathology, chondral defects, and bone marrow edema.
CONCLUSION
A masterful physical examination of the elbow requires a deep understanding of its complex biomechanics and the sequential nature of capsuloligamentous failure. By systematically employing provocative maneuvers—such as the moving valgus stress test for medial instability and the pivot-shift test for posterolateral rotatory instability—the orthopedic surgeon can accurately localize the pathology. Correlating these clinical findings with targeted advanced imaging ensures a precise diagnosis, forming the foundation for successful operative or non-operative management of the unstable elbow.
You Might Also Like