Surgical Management of Distal Radius Malunions: Radiographic Evaluation and Osteotomy Techniques

Key Takeaway
Distal radius malunions significantly alter wrist biomechanics, leading to pain, instability, and degenerative changes. Comprehensive radiographic evaluation, including bilateral CT and MRI, is essential for preoperative planning. Corrective osteotomy, often combined with volar locking plate fixation and bone grafting, restores anatomic alignment. Management of the distal radioulnar joint (DRUJ) is critical, dictating the need for concomitant ulnar shortening or salvage procedures to optimize functional outcomes.
RADIOGRAPHIC AND ADVANCED IMAGING EVALUATION
The foundation of successful surgical reconstruction for distal radius malunions lies in meticulous preoperative radiographic evaluation. Plain anteroposterior (AP) and lateral radiographs of both wrists in neutral rotation must be obtained. These standard views are critical to determine the nature and degree of the deformity, to detect carpal subluxation and instability patterns (such as dorsal intercalated segment instability [DISI] or volar intercalated segment instability [VISI]), and to evaluate the overall quality of the bone stock.
The uninjured contralateral wrist serves as the definitive anatomical template for surgical reconstruction when an osteotomy is chosen. By comparing the malunited radius to the normal side, the surgeon can precisely calculate the degree of correction necessary in the sagittal (volar/dorsal tilt), coronal (radial inclination), and axial (rotation) planes. Furthermore, this comparison dictates the exact size, geometry, and shape of the bone graft required to maintain the desired correction.
Clinical Pearl: Always obtain true lateral radiographs with the shoulder abducted 90 degrees, elbow flexed 90 degrees, and the wrist in neutral. Even slight pronation or supination can artificially alter the radiographic measurement of volar tilt and ulnar variance, leading to catastrophic miscalculations during preoperative templating.
While plain films are foundational, advanced imaging is indispensable for complex intraarticular malunions. Computed Tomography (CT) is highly beneficial for evaluating the potential for congruity of the distal radioulnar joint (DRUJ) using axial views. CT provides a high-resolution map of the articular surface, identifying step-offs, gap formations, and the exact location of intraarticular fracture lines that have healed in a malreduced position. Malunions of the ulnar styloid and the sigmoid notch are also exceptionally well delineated by CT reformats.
Magnetic Resonance Imaging (MRI) or MR arthrography should be utilized to evaluate the integrity of the soft-tissue envelope, specifically the triangular fibrocartilage complex (TFCC) and the intrinsic intercarpal ligaments (scapholunate and lunotriquetral ligaments). Unrecognized soft-tissue incompetence can lead to persistent pain and instability even after a perfectly executed osseous realignment.
TIMING OF SURGICAL INTERVENTION
The role of timing in the osteotomy of distal radial malunions has garnered significant attention in contemporary literature. Traditionally, corrective osteotomy was delayed until a patient proved to be persistently symptomatic after fracture healing and an exhaustive course of rehabilitation. It is well recognized that some patients, particularly those with lower functional demands, regain adequate function despite residual radiographic deformity.
However, delaying corrective surgery until a patient is chronically symptomatic may adversely affect the overall result. Prolonged angular deformity and shortening produce altered loading mechanics across the radiocarpal articular surface, leading to maladaptation of the soft tissues (capsule, ligaments) and chronic dysfunction of the DRUJ.
Surgical Warning: Chronic malalignment leads to irreversible contractures of the brachioradialis and volar extrinsic ligaments. Early intervention prevents these soft-tissue adaptations, significantly reducing the complexity of the surgical release required to mobilize the distal fragment.
Comparative studies have demonstrated no statistically significant differences in ultimate functional outcomes between early treatment groups and late treatment groups; however, the overall time of disability is significantly shorter in the early intervention cohort. Furthermore, early procedures (within 6 to 10 weeks post-injury) are technically less demanding. Fracture lines are more easily identified and taken down, congruity of the DRUJ is more easily restored, and soft tissue contractures are highly amenable to correction. Therefore, early reconstruction of distal radial malunions should be strongly considered in young patients with high functional demands who present with unacceptable radiographic parameters.
EXTRAARTICULAR MALUNION WITH DORSAL ANGULATION
Extraarticular malunions with dorsal angulation (malunited Colles fractures) represent the most common presentation requiring surgical correction. The pathoanatomy involves a loss of radial height, loss of radial inclination, and a reversal of the normal volar tilt to a dorsal tilt. This dorsal angulation shifts the radiocarpal load dorsally, increasing contact pressures on the radiolunate facet and unloading the volar radiocarpal ligaments, which can precipitate midcarpal instability.
Indications and Contraindications for Osteotomy
Osteotomy and grafting are most commonly indicated for malunited Colles fractures in patients younger than 45 years old, though physiological age and functional demand should supersede chronological age as the primary criterion. Older patients with excellent bone quality and high functional demands are also excellent candidates for corrective osteotomy.
Contraindications to radial osteotomy include:
* Active Complex Regional Pain Syndrome (CRPS) / Reflex Sympathetic Dystrophy.
* Acceptable clinical function despite radiographic deformity.
* A severely compromised soft tissue envelope.
* Severe osteopenia or osteoporosis precluding rigid internal fixation.
* Advanced radiocarpal or intercarpal degenerative arthritis (where salvage procedures like total wrist arthrodesis or proximal row carpectomy are more appropriate).
Distraction Osteogenesis
Distraction osteogenesis utilizing external fixation is a viable alternative to acute correction and plating. This technique applies the Ilizarov principle of tension-stress to gradually correct multiplanar deformities. It carries the benefit of not requiring a massive acute stretch on the median nerve and flexor tendons, and it avoids a second surgical procedure for plate removal.
Lubahn et al. reported that 17 of 20 patients healed uneventfully with this technique. However, complications are not trivial and include pin track infections, loss of pin purchase, and extensor pollicis longus (EPL) tendon rupture. Furthermore, Sammer et al., in a prospective study, found that although distraction osteogenesis was useful in improving anatomy and function in distal radial malunions requiring multiplanar correction, a substantial amount of residual impairment remained across all domains of the Michigan Hand Outcomes Questionnaire (MHQ), including activities of daily living. Patients must be counseled that function cannot be expected to return to pre-injury baselines.
Bone Grafting Strategies
The necessity and type of bone graft in corrective osteotomies remain a subject of intense academic debate. Historically, structural autograft (typically from the iliac crest) was mandatory to fill the opening wedge and provide structural support.
Recent advancements in fixed-angle volar locking plates have challenged this paradigm. Ozer found no significant differences in clinical or statistical outcomes between patients who underwent locked volar plating without bone grafting and those who received locked volar plating supplemented with allograft bone. The rigid construct of the locking plate acts as an internal fixator, maintaining the void until creeping substitution occurs.
Conversely, Abramo et al. utilized a bone graft substitute with a buttress pin and plate system and reported a minor loss of correction, suggesting that highly rigid fixation systems are absolutely necessary if structural autograft is omitted. Other authors investigating precise preoperative planning of corticocancellous bone grafts found no significant difference in alignment restoration compared to standard grafting techniques.
Innovative techniques have also been described to minimize graft site morbidity. Viegas described a modification utilizing a combined volar and dorsal approach for an angled step-cut osteotomy. The dorsally extruded fracture fragments are mobilized and utilized as a local dorsal strut graft to span the opening wedge osteotomy, eliminating the need for iliac crest harvest. Obert et al. pioneered the use of a costal cartilage graft harvested from the eighth rib, placed directly into the epiphyseal-metaphyseal defect for intraarticular malunions, reporting results comparable to traditional grafts.
Surgical Techniques: Corrective Osteotomy
The Fernandez Technique
Fernandez popularized an opening wedge metaphyseal osteotomy combined with the reinsertion of a structural graft and rigid internal fixation. This technique yields highly satisfactory results provided no degenerative changes are present in the radiocarpal and intercarpal joints, and the preoperative range of motion is adequate.
The procedure involves meticulous preoperative templating. The osteotomy site is marked, and K-wires are often used as joysticks to manipulate the distal fragment.

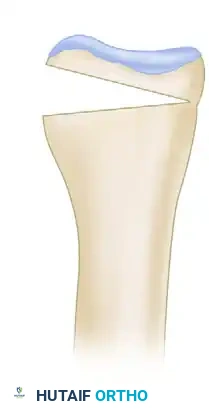
Once the osteotomy is completed, the distal fragment is mobilized. The brachioradialis insertion must be completely released to allow for restoration of radial length and volar tilt. The osteotomy is opened dorsally (or volarly, depending on the approach), and the defect is measured.

A precisely contoured structural graft (autograft or allograft) is prepared and impacted into the defect.


Rigid internal fixation is then applied. While Fernandez originally described dorsal plating, modern iterations heavily favor fixed-angle volar locking plates due to the decreased risk of extensor tendon irritation.


The Trapezoidal Graft Technique (Watson and Castle)
Watson and Castle reported success with a highly specific osteotomy technique utilizing a trapezoidal graft obtained from the dorsal radius or iliac crest. This geometric configuration is specifically designed to correct both the loss of radial length and the abnormal dorsal tilt simultaneously.
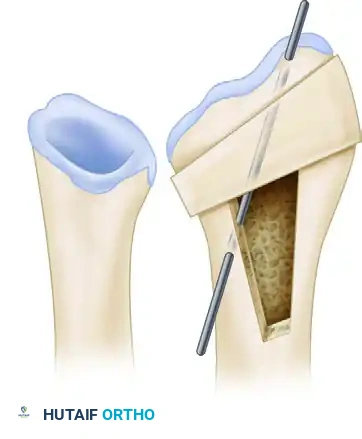
Preoperative posteroanterior view demonstrating decreased radial inclination. The osteotomy and trapezoidal graft site are carefully outlined during preoperative planning.
Postoperative posteroanterior view showing restoration of normal radial tilt, stabilized with a single "caging" pin or modern locking plate.
The biomechanical rationale for this correction is profound. Abnormal dorsal tilt of the radial articular surface reverses all physiological loads across the carpal bones. The normal volar radiocarpal ligaments are unloaded, and the dorsal capsule is stretched. This non-anatomic loading is poorly tolerated in active patients and rapidly leads to radiocarpal arthrosis.

Abnormal dorsal tilt reverses load mechanics across the carpus.
By inserting the precisely measured trapezoidal graft, the surgeon restores the normal 11 degrees of palmar tilt.

Postoperative lateral view demonstrating the restoration of 11 degrees of palmar tilt prior to the final seating of the graft.

Detail of the trapezoidal graft geometry required to achieve multiplanar correction.
Fixation Modalities
Several types of fixation methods have been evaluated with comparable results. Fixed-angle volar plating with or without bone grafting provides exceptionally stable fixation after corrective osteotomy, allowing for early postoperative mobilization. Tarng et al. utilized a 2.4-mm locking palmar plate without autologous bone grafting and noted sufficient stability to forgo cast immobilization, allowing early restoration of wrist range of motion.
Intramedullary nailing has also been reported to reliably correct deformity and produce good functional outcomes. The primary benefit of an intramedullary nail is its percutaneous insertion, which minimizes soft tissue stripping and preserves the periosteal blood supply, though it offers less control over complex multiplanar corrections compared to modern locking plates.
MANAGEMENT OF THE DISTAL RADIOULNAR JOINT (DRUJ)
Addressing the DRUJ is arguably the most complex aspect of distal radius malunion surgery. Restoration of radial length usually is impossible with a distal radial osteotomy alone if the soft tissues are severely contracted. A concomitant ulnar shortening osteotomy is often mandated in patients with more than 6 mm of radial shortening to decompress the ulnocarpal joint and allow reduction of the DRUJ.
If the DRUJ is arthritic or chronically irreducible despite adequate radial realignment, salvage procedures must be employed. A Bowers hemiresection interposition arthroplasty or a Sauvé-Kapandji procedure (distal radioulnar arthrodesis with proximal ulnar pseudarthrosis) should be performed. Long-term results after these osteotomies have shown that wrist alignment is maintained; however, patients must be counseled that some degree of instability or symptomatic wrist arthritis may persist.
An ulnar shortening osteotomy alone can be utilized to correct incongruence of the DRUJ if the primary radial deformity is minor and the patient's main complaint is ulnar-sided wrist pain secondary to ulnocarpal impaction.
Resection of the distal ulna (Darrach procedure) is another relatively simple technique useful in providing pain relief and improving pronosupination in older, lower-demand patients. This technique is technically less demanding than a formal radial osteotomy and avoids the risks of nonunion. However, the distal radial deformity is not corrected, radiocarpal symptoms may persist, and potential complications include painful instability of the distal ulnar stump and a significant loss of grip strength.
Guidelines for Treatment of the DRUJ in Radial Malunions
Surgical decision-making for the DRUJ should follow established algorithms, such as those modified from Graham TJ (Table 58-3):
- Radioulnar Length Unacceptable / DRUJ Reducible / Potential for Congruity (Yes): Distal Radial Osteotomy (DRO) alone is indicated.
- Radioulnar Length Acceptable / DRUJ Unacceptable / Potential for Congruity (Yes): Ulnar Shortening (US) alone is indicated.
- Radioulnar Length Unacceptable / DRUJ Unacceptable / DRUJ Not Reducible by DRO / Potential for Congruity (Yes): DRO combined with Ulnar Shortening, or a two-stage reconstruction.
- Radioulnar Length Unacceptable / DRUJ Unacceptable / DRUJ Not Reducible / No Potential for Congruity: DRO combined with DRUJ ablation (Bowers or Sauvé-Kapandji).
Clinical Pearl: Flinkkilä et al. strongly advise against performing a complex distal radial osteotomy for the treatment of malunion in patients with only mild symptoms. In their cohort, restoration of normal anatomy did not consistently correlate with subjectively good results, and a high percentage of patients required secondary surgeries for DRUJ instability or progressive osteoarthritis. Patient selection is paramount.
CONCOMITANT PROCEDURES: CARPAL TUNNEL RELEASE
Carpal tunnel release is frequently indicated either alone or in combination with corrective osteotomy. Dorsally displaced malunions physically decrease the volumetric space within the carpal tunnel. The prominent volar metaphysis acts as a fulcrum, impairing the excursion of the flexor tendons and directly compressing the median nerve. Division of the deep transverse carpal ligament in this situation is a low-morbidity addition that reliably improves neurological function and tendon glide in the hand and wrist.
POSTOPERATIVE PROTOCOLS
Postoperative management is dictated by the rigidity of the fixation. When fixed-angle volar locking plates are utilized, the wrist is typically immobilized in a bulky dressing and volar splint for 10 to 14 days to allow for soft tissue healing. Following suture removal, patients are transitioned to a removable thermoplastic splint and immediately begin active and active-assisted range of motion exercises under the guidance of a certified hand therapist.
Pronation and supination exercises are initiated early to prevent DRUJ stiffness, particularly if an ulnar shortening osteotomy was performed concomitantly. Strengthening exercises are generally delayed until radiographic evidence of bony union is observed, typically between 6 to 8 weeks postoperatively. Patients must be monitored closely for complications, including hardware failure, loss of correction, and extensor tendon irritation, which may necessitate hardware removal after complete osseous consolidation.
You Might Also Like
