Operative Management of Distal Radius Fractures: A Comprehensive Surgical Guide
Key Takeaway
Distal radius fractures require meticulous evaluation of injury mechanisms and precise anatomical restoration. Utilizing the Fernandez classification, surgeons can dictate appropriate interventions ranging from percutaneous pinning to complex open reduction and internal fixation. Adherence to strict radiographic parameters—such as restoring radial length, inclination, and volar tilt—is paramount to optimizing functional outcomes and minimizing post-traumatic arthrosis in both low-demand and high-demand patient populations.
Introduction to Distal Radius Fractures
Fractures of the distal radius are among the most common orthopedic injuries, presenting a bimodal distribution that affects both young, high-energy trauma patients and elderly, osteoporotic individuals. Historically, these fractures have been classified as either extraarticular or intraarticular, with numerous eponyms (e.g., Colles, Smith, Barton, Chauffeur) applied to specific fracture patterns. However, the reliance on eponyms has resulted in considerable confusion in the literature, particularly concerning the differentiation between Barton and Smith fractures.
Modern orthopedic practice dictates that distal radius fractures should be classified and treated based on the mechanism of injury and the resultant biomechanical instability. Achieving anatomical reduction is paramount; failure to restore articular congruity and radial length significantly alters wrist kinematics, leading to restricted range of motion, distal radioulnar joint (DRUJ) dysfunction, and early post-traumatic arthrosis.
Biomechanics and Pathoanatomy
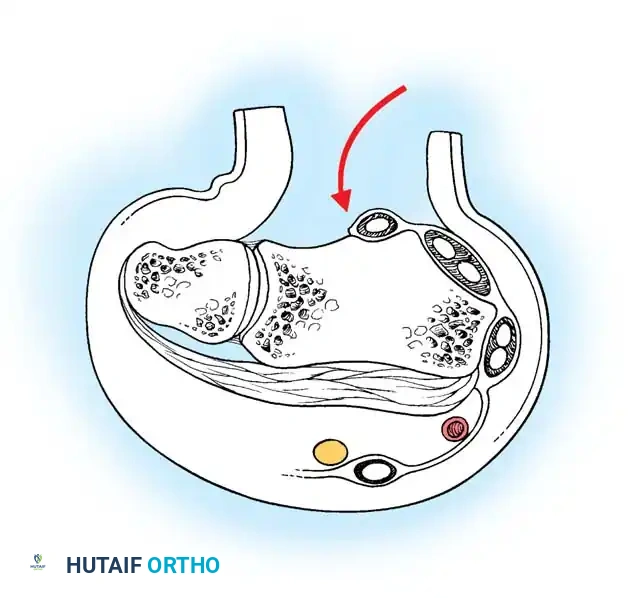
The distal radius articulates with the proximal carpal row (scaphoid and lunate) and the distal ulna. In a normal wrist, approximately 80% of the axial load is transmitted through the radiocarpal joint, and 20% through the ulnocarpal joint.
Clinical Pearl: Bronstein et al. demonstrated in a cadaveric study that a shortening of the distal radius by merely 10 mm reduces forearm pronation by almost 50% and supination by 30%. Furthermore, dorsal angulation shifts the load-bearing axis dorsally, increasing stress on the radiocarpal ligaments and the triangular fibrocartilage complex (TFCC).
Classification Systems
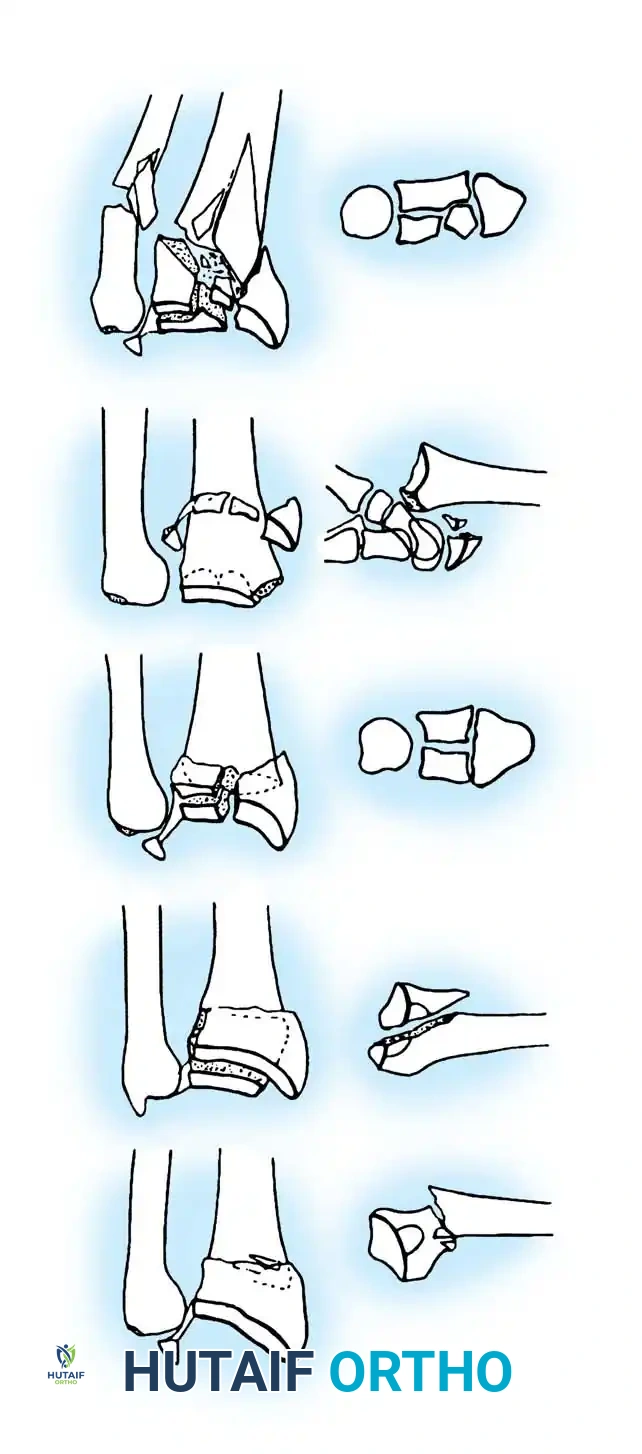
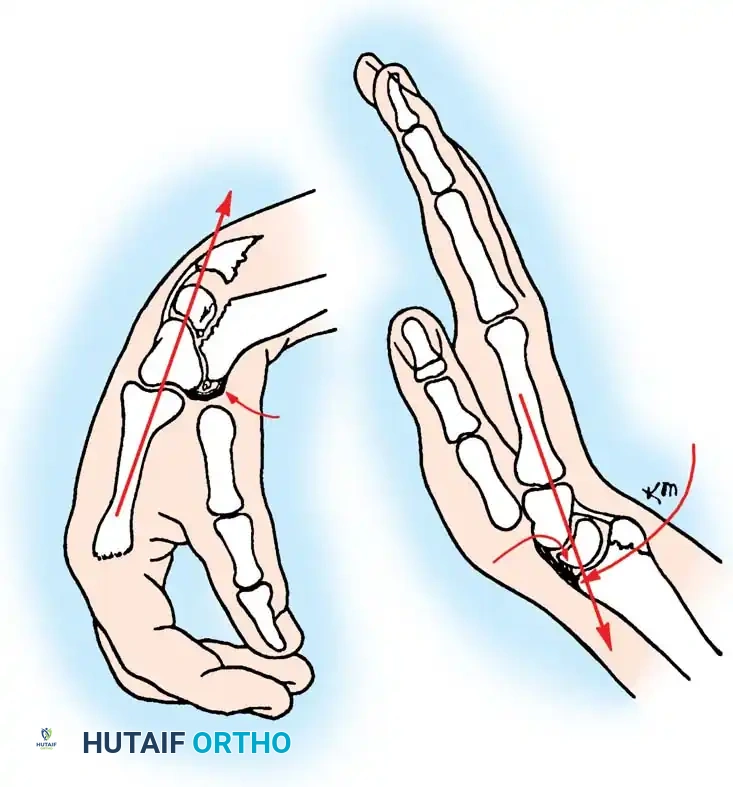
We agree with Fernandez that fractures of the distal radius should be classified on the basis of the mechanism of injury. Manual reduction techniques require the application of force in a direction opposite to the force that produced the injury. The Fernandez classification divides these fractures into five distinct types:
Fig. 54-101 Fractures of distal radius classified by mechanism of injury. I, Bending. II, Shear. III, Impaction. IV, Avulsions with fracture-dislocation. V, High velocity. (From Fernandez DL: Fractures of the distal radius: operative treatment, Instr Course Lect 42:73, 1993.)
- Type I (Bending): Extraarticular metaphyseal bending fractures. One cortex fails in tension, while the opposite cortex is comminuted and impacted. Examples include Colles (dorsal angulation) and Smith (volar angulation) fractures.
- Type II (Shearing): Intraarticular fractures produced by shearing forces. These include volar Barton, dorsal Barton, and radial styloid (Chauffeur) fractures.
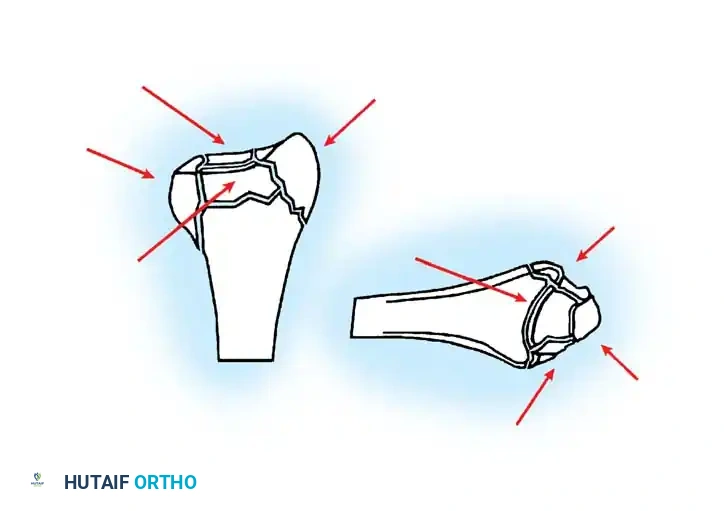
- Type III (Compression/Impaction): Intraarticular fractures resulting from axial loading that causes impaction of metaphyseal bone. These include complex articular fractures and radial pilon fractures.
- Type IV (Avulsion): Avulsion fractures of ligament attachments occurring with radiocarpal fracture-dislocations.
- Type V (High-Velocity): Complex injuries involving multiple forces, extensive comminution, and significant soft-tissue damage.
Radiographic Evaluation and Reduction Guidelines
Standard posteroanterior (PA), lateral, and oblique radiographs are mandatory. Computed Tomography (CT) is highly recommended for Type II, III, and V fractures to assess articular comminution and surgical planning.
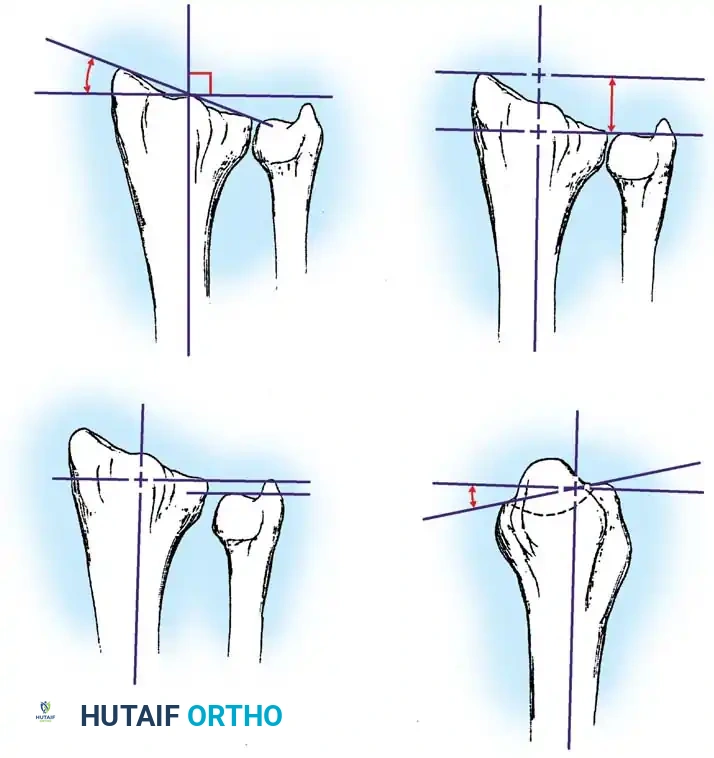
Fig. 54-102 Normal average distal radial angles. A, Radial inclination (RI; average 22 degrees). B, Radial length (RL; average 12 mm). C, Ulnar variance (UV; average 0 to − 2 mm). D, Radial tilt (RT; average 11 degrees volar). (From Graham TJ: Surgical correction of malunited fractures of the distal radius, J Am Acad Orthop Surg 5:270, 1997.)
Nana et al. and Graham recommended restoration of the distal radial anatomy within established guidelines. The patient’s functional activity level and general health dictate how closely these guidelines must be followed.
Box 54-3 • Guidelines for Reduction of Distal Radial Fractures
1. Radial shortening < 5 mm at the distal radioulnar joint.
2. Radial inclination on posteroanterior radiographs > 15 degrees.
3. Sagittal tilt on lateral projection between 15 degrees dorsal tilt and 20 degrees volar tilt.
4. Intraarticular step-off or gap < 2 mm of the radiocarpal joint.
5. Articular incongruity < 2 mm of the sigmoid notch of the distal radius.
Indications for Operative Management
Most Type I distal radial fractures can be successfully treated nonoperatively. Young and Rayan found that 92% of "low-demand" patients had satisfactory results after nonsurgical treatment of isolated distal radial fractures, regardless of the radiographic or clinical appearance of the wrist.
However, in younger, high-demand patients, near-normal function and clinical/radiographic appearance are expected. Operative intervention is indicated when:
* Maintenance of reduction requires prolonged immobilization in extreme, non-physiologic positions.
* Reduction is lost early in treatment.
* Significant metaphyseal comminution or osteopenia makes closed treatment unsuitable.
* The fracture is a Type II shear fracture (e.g., Barton type), which is almost impossible to treat by closed means.
* The fracture is a Type III compression injury with significant intraarticular damage or severe radial shortening.
Surgical Approaches and Positioning
Patient Positioning
The patient is placed supine with the affected extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Fluoroscopy (C-arm) is positioned either parallel or perpendicular to the table, depending on surgeon preference, to allow for unobstructed AP and lateral imaging.
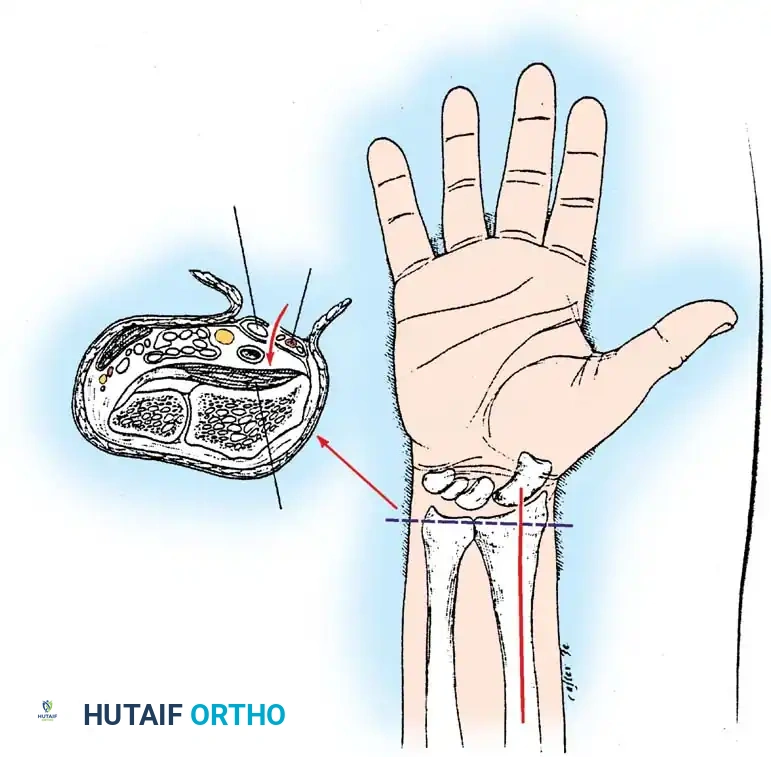
The Volar Approach (Modified Henry)
The modified Henry approach is the workhorse for volar plating. An incision is made over the flexor carpi radialis (FCR) tendon. The sheath of the FCR is incised, and the tendon is retracted ulnarly, protecting the median nerve. The floor of the FCR sheath is incised to access the pronator quadratus (PQ). The PQ is elevated from its radial and distal borders in an L-shaped fashion to expose the volar distal radius.
Operative Techniques
Percutaneous Pinning of Type I Fractures
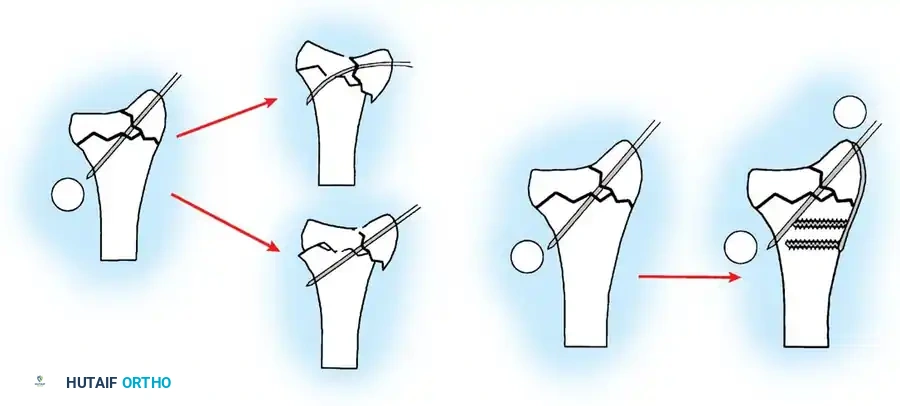
If maintenance of reduction of Colles or Smith fractures requires prolonged immobilization, or if reduction is lost early, closed reduction followed by percutaneous pinning is highly effective.
TECHNIQUE 54-18
* Manipulate and reduce the fracture using longitudinal traction and appropriate counter-forces.
* Insert two large, unthreaded Kirschner wires (K-wires) through the radial styloid across the fracture and into the opposite metaphyseal cortex using a power drill, while an assistant maintains the reduction.
* Confirm good reduction and pin placement with image intensification.
* Cut the pins off beneath the skin. This provides sufficient fixation to minimize radial collapse and shortening, allowing immobilization in a cast with the wrist in a neutral position.
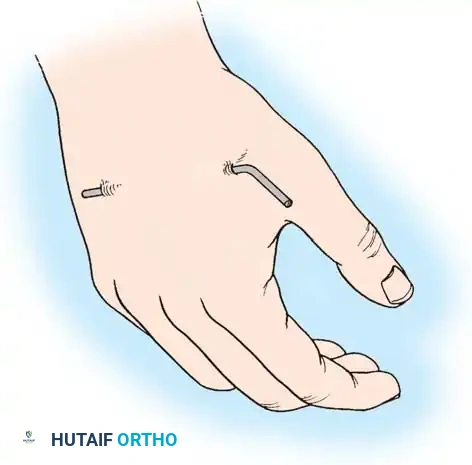
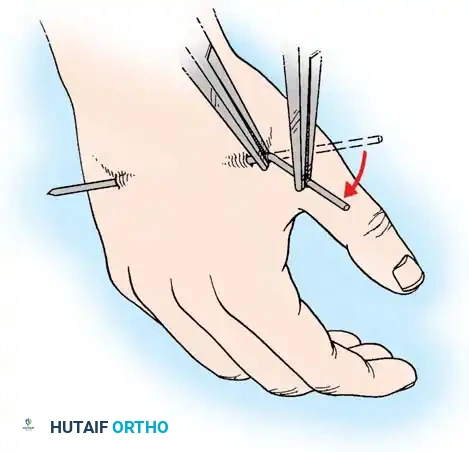
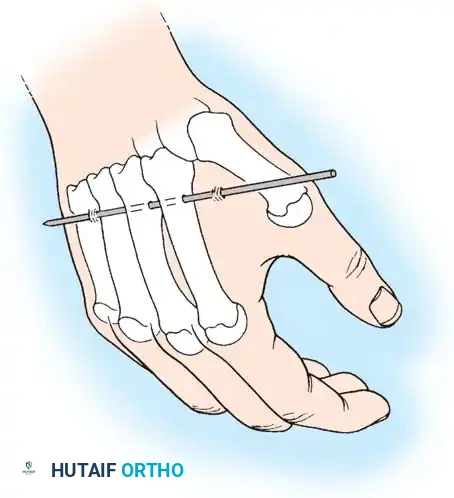
Fig. 54-104 Distal pin insertion for pins-and-plaster method of treatment of wrist fractures. A, Distal pin is inserted in second and third metacarpals only. B and C, Because pin protrudes in this position, limitation of abduction and extension of thumb result unless pin is routinely bent back at base of second metacarpal.
Aftertreatment: The arm is immobilized in a cast above the elbow with the forearm and wrist in a neutral position. The K-wires are removed at 6 weeks. The wrist is then supported with a removable splint, and gradual range-of-motion exercises are initiated.

External Fixation and Traction Casting
When significant metaphyseal comminution or osteopenia makes pinning unsuitable, external fixation utilizing the principle of ligamentotaxis is preferred. For severely comminuted fractures unsuitable for percutaneous K-wire stabilization, a pins-and-plaster traction cast often produces excellent results.
TECHNIQUE 54-19 (Traction Cast Application)
* Reduce the fracture under adequate anesthesia by suspending the forearm by the fingers in Chinese fingertraps.
* After approximately 5 minutes of traction, gently manipulate the fracture.
* Insert a 2.4-mm (3/32-inch) Steinmann pin transversely through the proximal ulna 7.5 to 10 cm distal to the olecranon.
* Insert a second pin transversely through the bases of the second and third metacarpals.
* Surgical Warning: Care must be taken to "milk" the first dorsal interosseous muscle to the volar side to prevent it from being caught as the pin is inserted into the base of the second metacarpal.
* Apply a plaster cast to above the elbow, incorporating the two pins. Cut back the palm of the cast proximal to the flexion crease to allow full active motion of the fingers.
Aftertreatment: The pins and cast (or commercial external fixator) are left in place for 8 weeks. Removing the pins earlier allows the distal radius to shorten or reimpact. Active hand and shoulder exercises are encouraged throughout.
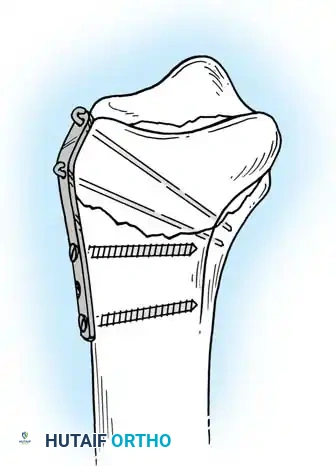
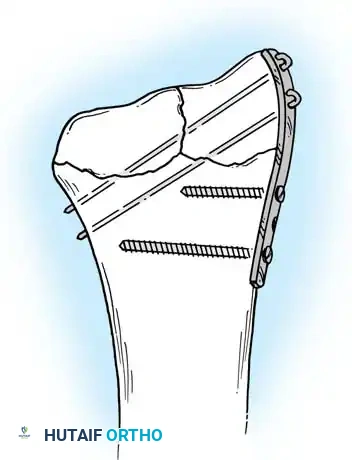
Open Reduction and Internal Fixation (ORIF)
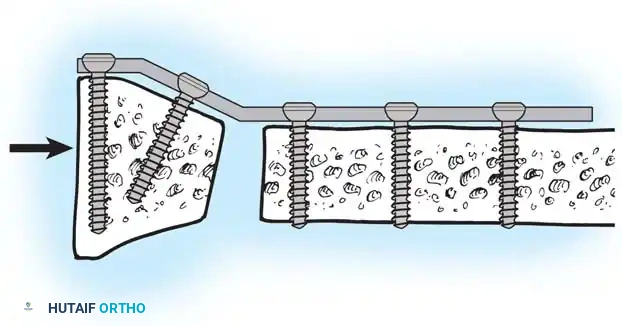
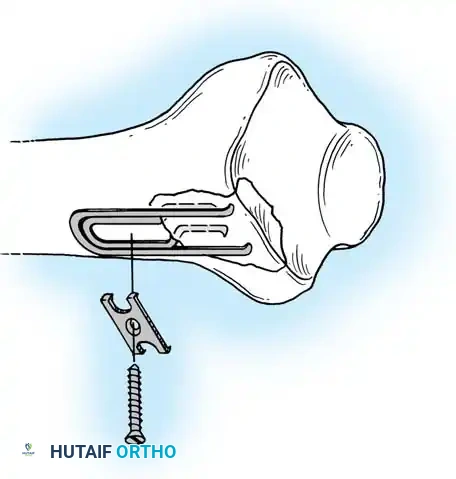
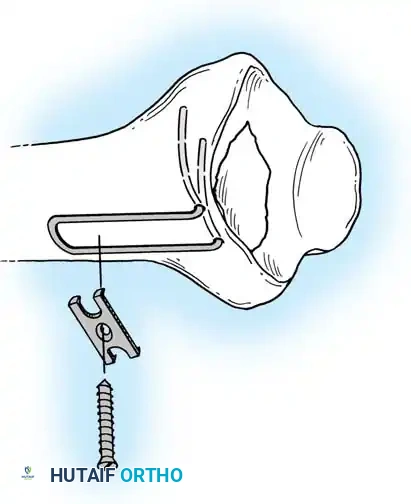
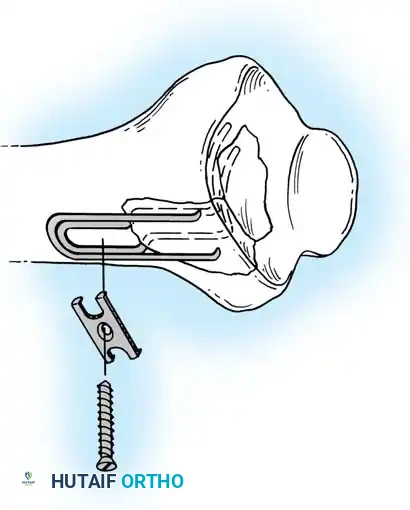
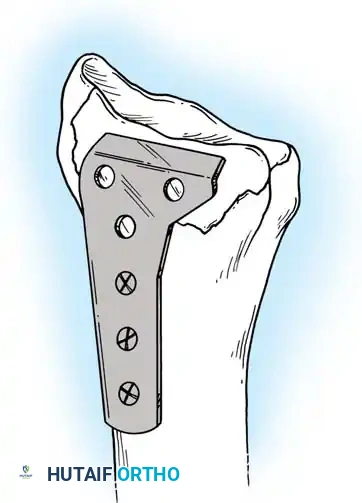
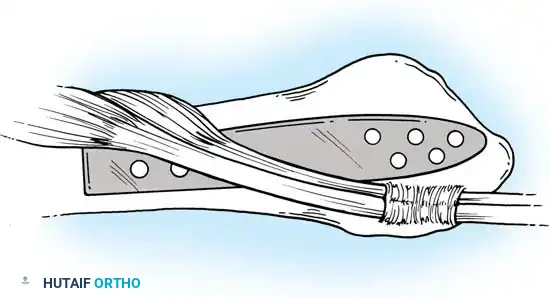
Type II distal radial shear fractures (Barton type) usually require ORIF. These fractures are almost impossible to treat by closed means. Buttress plate fixation of volar Barton fractures is the gold standard.
Type III compression injuries require operative treatment if intraarticular damage is significant or radial shortening is severe. Careful restoration of the articular surface, radial angulation, and length is crucial. Fixation with multiple K-wires or plates is often necessary, and cancellous bone grafting is frequently required to fill impacted metaphyseal voids.


Often, a combination of open and closed techniques is necessary to treat Type III fractures satisfactorily.

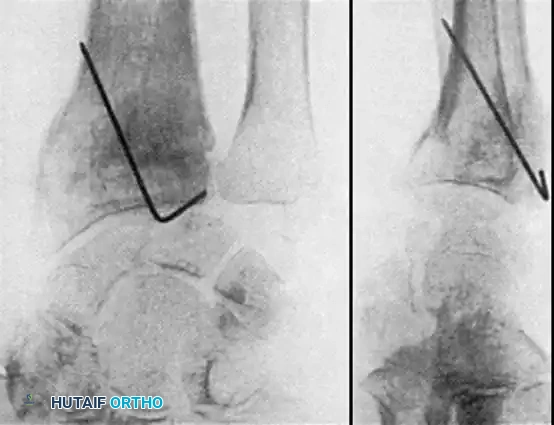
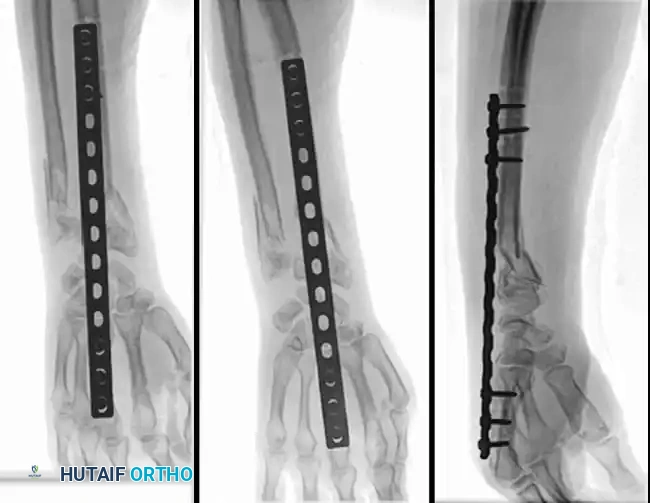
Fig. 54-103 A and B, Four-part type III distal radial fracture treated by open reduction, internal fixation of intraarticular component, iliac bone grafting, and external fixation. C and D, Follow-up radiographs at 5 weeks (C) and 3 years (D) show anatomical restoration of joint surface, maintenance of radial length, and absence of degenerative changes.
Arthroscopically Assisted Fixation
Mehta et al. reported 88% good-to-excellent results in patients with intraarticular distal radial fractures using arthroscopically assisted percutaneous fixation with K-wires. This modality allows direct visualization of the articular surface, facilitating the treatment of concomitant triangular fibrocartilage complex (TFCC) tears and intracarpal ligament injuries. The goal is to achieve an anatomical reduction with an articular step-off of less than 1 mm.
Management of Type IV and V Fractures
Type IV avulsion fractures are associated with radiocarpal fracture-dislocations and are highly unstable. The avulsed fragments are often too small for screw fixation and require suture repair or K-wire stabilization. External fixation using ligamentotaxis is inappropriate here due to extensive ligamentous disruption.
Type V high-velocity fractures are always unstable, frequently open, and notoriously difficult to treat. A combination of percutaneous pinning, external fixation, and limited open reduction is often necessary.
Management of Open Forearm and Distal Radius Fractures
The management of open fractures requires meticulous soft-tissue handling. We generally prefer not to use internal fixation initially in Gustilo Type III open fractures of the forearm. Complications are minimized if the wound is initially managed with aggressive irrigation and débridement.
If the wound is clean at 5 to 7 days, appropriate internal fixation can be performed. Anderson et al. reported excellent outcomes using this delayed method of ORIF with compression plating, noting zero infections in 38 open fractures.
Conversely, current treatment trends increasingly favor immediate ORIF for all open forearm fractures, provided radical débridement is achieved. Duncan et al. reported 90% acceptable results in Gustilo Type I, II, and IIIA open diaphyseal forearm fractures treated with immediate débridement and compression plating. However, results with Type IIIB and IIIC injuries remain poor, necessitating temporizing external fixation.
Surgical Pitfall: In single-bone fractures of the forearm, shortening from overriding resulting from a delay in internal fixation is rarely a problem. However, to prevent shortening in both-bone fractures associated with open wounds, pins through the proximal ulna and the bases of the metacarpals must be used to apply traction and restore length.


If the soft-tissue wound is massive, making skin grafting and reconstructive procedures inevitable, an intramedullary nail in the ulna or a spanning external fixator can be used to stabilize the forearm. Soft-tissue reconstruction is almost impossible unless the skeletal framework is rigidly stabilized.

📚 Medical References
- distal radius fractures, Hand Surg 5:113, 2000.
- Rehak DC, Kasper P, Boratz ME, et al: A comparison of plate and pin fixation for the rheumatoid wrist, Orthopedics 23:43, 2000.
- Richards RR, Patterson SD, Hearn TC: A special plate for arthrodesis of the wrist: design considerations and biomechanical testing, J Hand Surg 18A:476, 1993.
- Richterman I, Weiss AP: Wrist fusion, Hand Clin 13:681, 1997.
- Sauerbier M, Kluge S, Bickert B, et al: Subjective and objective outcomes after total wrist arthrodesis with radiocarpal arthrosis of Kienbock’s disease, Chir Main 19:223, 2000.
- Skak S: Arthrodesis of the wrist by the method of Mannerfelt, Acta Orthop Scand 53:557, 1982.
- Smith-Petersen MN: A new approach to the wrist joint, J Bone Joint Surg 22:122, 1940.
- Sorial R, Tonkin MA, Geschwind C: Wrist arthrodesis using a sliding radial graft and plate fixation, J Hand Surg 19B:217, 1994.
- Stanley J, Hullin M: Wrist arthrodesis as a part of composite surgery of the hand, J Hand Surg 11B:243, 1986.
- Stein I: Gill turnabout radial graft for wrist arthrodesis, Surg Gynecol Obstet 106:231, 1958.
- Taleisnik J: Rheumatoid arthritis of the wrist, Hand Clin 5:257, 1989.
- Urbaniak JR: Arthrodesis of the hand and wrist. In Evarts CM, ed: Surgery of the musculoskeletal system, New York, 1990, Churchill Livingstone. Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius, J Bone Joint Surg 75A:899, 1993.
- Viegas SF, Rimoldi R, Patterson R: Modified technique of intramedullary fixation for wrist arthrodesis, J Hand Surg 14A:618, 1989.
- Voutilainen N, Juutilainen T, Pätiälä H, et al: Arthrodesis of the wrist with bioabsorbable fixation in patients with rheumatoid arthritis, J Hand Surg 27B:563, 2002.
- Watson HK, Goodman ML, Johnson TR: Limited wrist arthrodesis: II. Intercarpal and radiocarpal combinations, J Hand Surg 6A:223, 1981.
- Watson HK, Hempton RF: Limited wrist arthrodesis: I. The triscaphoid joint, J Hand Surg 5A:320, 1980.
- Watson HK, Vendor MI: Wrist and intercarpal arthrodesis. In Chapman MW, ed: Operative orthopedics, Philadelphia, 1993, Lippincott. Weideman G, Quenzer D, Strickland J, et al: Arthrodesis for post-traumatic arthritis of the wrist: reliability and function. Paper presented at 42nd annual meeting of the American Society for Surgery of the Hand, San Antonio, Tex, Sept 11, 1987.
- Weiss AP, Hastings H II: Wrist arthrodesis for traumatic conditions: a study of plate and local bone graft application, J Hand Surg 20A:50, 1995.
- Wood M: Wrist arthrodesis using dorsal radial bone graft, J Hand Surg 12A:208, 1987.
- Wright CS, McMurtry RY: AO arthrodesis in the hand, J Hand Surg 8A:932, 1983.
- Yang RS, Liu TK: Arthrodesis of the nonrheumatoid wrist, Taiwan Yi Xue Hui Za Zhi 88:258, 1989.
- Zachary SV, Stern PJ: Complications following AO/ASIF wrist arthrodesis, J Hand Surg 20A:339, 1995.
You Might Also Like

