Distal Radius and Galeazzi Fractures: Principles of Operative Management
Key Takeaway
Distal radius fractures account for nearly 20% of all emergency department fractures. While historical management relied heavily on closed reduction, modern orthopedic surgery emphasizes precise anatomical restoration, particularly in high-demand patients. This guide details the biomechanics, radiographic parameters, and operative techniques for distal radius and Galeazzi fracture-dislocations, providing an evidence-based algorithm for rigid internal fixation and distal radioulnar joint (DRUJ) stabilization.
FRACTURES OF THE DISTAL RADIUS: HISTORICAL CONTEXT AND MODERN CONTROVERSIES
"…will at some remote period again enjoy perfect freedom in all of its motions and be completely exempt from pain."
— Abraham Colles, 1814
The management of distal radius fractures has evolved significantly since Abraham Colles’ optimistic proclamation in the early 19th century. Today, distal radius fractures account for up to 20% of all fractures treated in emergency departments. Despite Colles' assertion, modern clinical follow-ups reveal that many patients are not "completely exempt from pain" following treatment.
In recent years, more than 1,000 peer-reviewed studies have been published regarding the optimal management of these injuries. Yet, absolute consensus remains elusive. Treatment algorithms are frequently complicated by confounding variables, including the required degree of anatomical restoration, inherent bone quality, the continuous emergence of novel fixation devices, surgeon experience, and the varying functional demands of older populations.
The Bimodal Distribution and Functional Demand
The desire for precise anatomical restoration of the radiocarpal and distal radioulnar joints is the primary rationale for operative intervention. However, patient populations present in a distinctly bimodal distribution:
1. Young, High-Demand Patients: Typically sustain high-energy trauma resulting in complex, intra-articular, and comminuted fractures. In this cohort, restoration of distal radial anatomy is universally considered essential to minimize the devastating complications of post-traumatic radiocarpal arthrosis and long-term functional impairment.
2. Elderly, Low-Demand Patients: Typically sustain low-energy fragility fractures. Multiple recent reports indicate that older, lower-demand patients tend to tolerate radiographic incongruity, deformity, and malunion surprisingly well.
However, nonoperative management in the elderly is not entirely benign. Madhok et al. noted that among elderly patients treated nonoperatively, 26% still reported significant functional impairment. While it is established that elderly patients tolerate more displacement than younger cohorts, identifying precisely which elderly patients would benefit from operative anatomical restoration remains a topic of active debate.
The Role of Bone Quality
Bone quality is a critical confounding variable when determining the optimal treatment strategy. The structural integrity of the distal radius directly dictates the surgeon's ability to obtain and, more importantly, maintain a reduction. In patients with severe osteoporosis, even low-energy trauma can produce profound displacement and comminution. Recognizing this, Ketter et al. have strongly advocated that osteoporosis should be formally integrated into classification systems for distal radius fractures, as it fundamentally alters the biomechanical stability of any chosen fixation construct.
RADIOGRAPHIC CRITERIA FOR ACCEPTABLE REDUCTION
A constant theme in contemporary orthopedic literature is that the specific surgical technique (e.g., closed reduction and percutaneous pinning, external fixation, dorsal plating, volar locked plating, or intramedullary nailing) is secondary in importance to the actual attainment of anatomical reduction.
Both clinical outcome studies and biomechanical models demonstrate that the maintenance of palmar tilt, ulnar variance, and radial height are the most critical factors in securing excellent long-term outcomes. Failure to restore these parameters alters carpal kinematics, shifts load-bearing forces abnormally onto the triangular fibrocartilage complex (TFCC) and ulnar head, and accelerates degenerative joint disease.
Standard Radiographic Parameters
The following criteria dictate the thresholds for acceptable reduction in distal radius fractures:
- Ulnar Variance (Radial Length):
- Normal: ± 2 mm (comparing the level of the lunate facet to the ulnar head).
- Acceptable: No more than 2 mm of shortening relative to the ulnar head.
- Radial Height:
- Normal: 12 mm.
- Acceptable: Within 2 to 3 mm of the contralateral normal wrist (typically > 9 mm).
- Palmar (Lateral) Tilt:
- Normal: 11 degrees of volar tilt.
- Acceptable: Neutral (0 degrees). Dorsal angulation is poorly tolerated.
- Radial Inclination:
- Normal: 20 to 22 degrees (measured from the lunate facet to the radial styloid).
- Acceptable: No less than 10 degrees.
- Intra-articular Step or Gap:
- Normal: None (perfectly congruent).
- Acceptable: Less than 2 mm of either step-off or gap.
Clinical Pearl: Even 1 mm of articular incongruity in the radiocarpal joint has been associated with a significantly increased risk of post-traumatic arthrosis in high-demand patients. When closed reduction cannot achieve these strict parameters, operative intervention is strongly indicated.
GALEAZZI FRACTURE-DISLOCATIONS
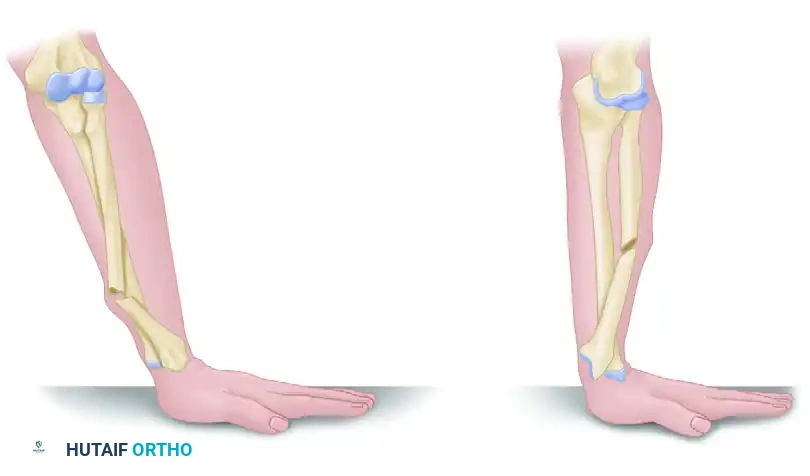
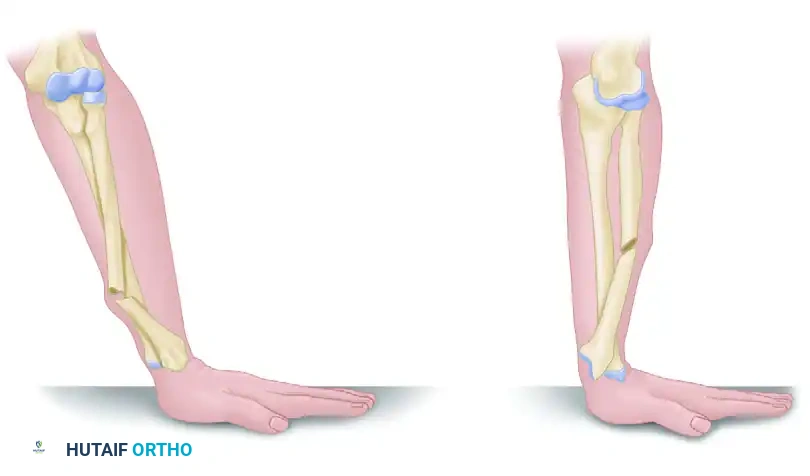
While isolated distal radius fractures are common, the surgeon must maintain a high index of suspicion for associated injuries, most notably the Galeazzi fracture-dislocation. Defined as a fracture of the distal third of the radial shaft accompanied by a disruption of the distal radioulnar joint (DRUJ), this injury is notoriously unstable and mandates operative intervention in adults.
Mechanism of Injury and Classification
Galeazzi fractures are classified based on the direction of radial displacement, which is dictated by the biomechanics of the forearm at the moment of axial loading.
Type I (Apex Volar):
Caused by axial loading of the forearm in supination. This mechanism results in the dorsal displacement of the distal radius fragment and a corresponding volar dislocation of the distal ulna.
Type II (Apex Dorsal):
Caused by axial loading of the forearm in pronation. This results in the anterior (volar) displacement of the distal radius fragment and a dorsal dislocation of the distal ulna.
Operative Management of Galeazzi Fractures
Historically termed the "fracture of necessity," adult Galeazzi fractures cannot be managed conservatively. Closed treatment inevitably leads to loss of reduction, malunion of the radius, and chronic, painful instability of the DRUJ.
1. Fixation of the Radial Shaft
The primary surgical objective is the rigid, anatomical restoration of the radial shaft. This is typically achieved via an open reduction and internal fixation (ORIF) utilizing a volar (Henry) approach.

Preoperative radiograph demonstrating a classic Galeazzi fracture-dislocation with significant displacement of the distal radial shaft and gross disruption of the DRUJ.
The radius is exposed, and the fracture is reduced anatomically. Fixation is achieved using a 3.5-mm dynamic compression plate (DCP) or locking compression plate (LCP). The plate is typically applied to the volar surface of the radius, which provides a flat surface for plate application and avoids irritation of the dorsal extensor tendons.


Postoperative anteroposterior (AP) and lateral radiographs following rigid fixation with a 3.5-mm AO dynamic compression plate and screws. In this specific case, anatomical restoration of the radius spontaneously reduced the DRUJ, rendering temporary stabilization with a transverse Kirschner wire unnecessary.
2. Intraoperative Assessment of the DRUJ
Once the radius is rigidly fixed, the surgeon's attention must immediately turn to the DRUJ. The stability of the DRUJ dictates the remainder of the surgical procedure and the postoperative rehabilitation protocol.
Surgical Warning: Never assume the DRUJ is stable simply because the radius has been plated. The DRUJ must be dynamically tested intraoperatively through a full range of pronation and supination. Ballottement of the distal ulna in neutral, full pronation, and full supination is mandatory.
Treatment Algorithm for DRUJ Management
The management of the DRUJ in Galeazzi fractures follows a strict, evidence-based algorithm:
- Assess DRUJ Stability: Following radial plating, evaluate the DRUJ.
- Reduced and Stable: If the DRUJ is anatomically reduced and stable throughout the full range of motion, no further operative intervention is required. The patient is placed in a protective splint, and early, controlled motion is initiated.
- Reduced but Unstable: If the DRUJ reduces but subluxates or dislocates during rotation, the stabilizing structures (primarily the TFCC and ulnar styloid) are compromised.
- Large Ulnar Styloid Fragment: If a large, displaced ulnar styloid fragment is present (which serves as the attachment site for the deep radioulnar ligaments of the TFCC), ORIF of the ulnar styloid is performed using tension band wiring or a small lag screw.
- No Ulnar Styloid Fragment (or small avulsion): The instability is due to a purely ligamentous TFCC tear. The surgeon must either perform an open exploration and direct repair of the TFCC or achieve temporary stabilization by pinning the ulna to the radius with a transverse K-wire (typically placed with the forearm in supination).
- Irreducible DRUJ: If the DRUJ cannot be reduced, soft tissue interposition is certain. The joint must be explored dorsally. Common offending structures blocking reduction include the extensor carpi ulnaris (ECU) tendon, the median nerve, or fragments of the torn TFCC. The interposing tissue is released, the joint is reduced, and stability is reassessed.
If K-wire fixation or TFCC repair is required, the patient is typically immobilized in an above-elbow cast in supination for 4 to 6 weeks to allow for ligamentous healing before the pins are removed and motion is commenced.
CONCLUSION
The operative management of distal radius fractures and Galeazzi fracture-dislocations requires a profound understanding of forearm biomechanics, meticulous radiographic evaluation, and precise surgical execution. Because of the heterogeneous nature of these injuries and the bimodal distribution of patients, treatment cannot be monolithic.
Surgeons must individualize their approach based on patient expectations, functional demand, bone quality, and specific fracture characteristics. Whether utilizing volar locked plating for an osteoporotic distal radius fracture or executing the complex DRUJ algorithm for a Galeazzi injury, the ultimate goal remains unchanged: anatomical restoration to ensure the patient may, as Colles hoped, "enjoy perfect freedom in all of its motions."
You Might Also Like

