Operative Management of Osteochondral and Distal Femur Fractures

Key Takeaway
Osteochondral and distal femur fractures present complex reconstructive challenges requiring meticulous surgical technique. This guide details evidence-based protocols for operative management, including anatomical approaches, biological osteosynthesis, and advanced fixation constructs such as dynamic condylar screws and locked plating. Emphasizing early mobilization and stable internal fixation, these techniques optimize functional outcomes and minimize complications in both adolescent and osteoporotic patient populations.
OSTEOCHONDRAL KNEE FRACTURES
Osteochondral fractures of the knee represent a distinct clinical entity that frequently results in the formation of intra-articular loose bodies. Historically, an extensive survey conducted by the Army Air Force of approximately 186 patients with loose bodies in the knee revealed that in 21 of these cases, the loose bodies were the direct result of osteochondral fractures originating from either the femur or the patella. Subsequent literature by Rosenberg, Ahstrom, Kennedy, Grainger, and McGraw has corroborated these findings, establishing a clear pathoanatomical pattern.
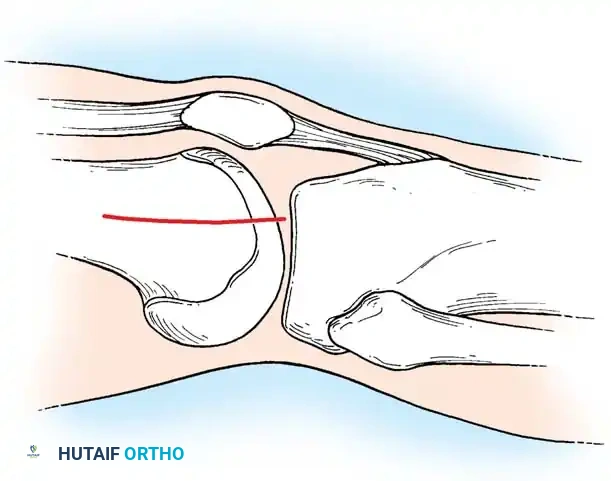
Rosenberg specifically identified that osteochondral fractures of the lateral femoral condyle are disproportionately common in adolescent boys. The primary biomechanical mechanism is often a transient lateral dislocation of the patella. As the patella relocates, it shears off a fragment of the lateral femoral condyle. Because these fragments possess a strong tendency to migrate and cause mechanical symptoms (locking, catching, and accelerated chondrolysis), surgical intervention is almost universally required.
Surgical Indications and Fixation Modalities
The primary goal of surgery is the anatomical restoration of the articular surface to prevent early-onset osteoarthritis. If the fragment involves a weight-bearing surface and possesses sufficient attached subchondral bone to allow for osseous healing, internal fixation is strictly recommended.
Surgical Warning: If diagnosis and surgery are significantly delayed, the edges of the osteochondral fragment and the donor defect will become rounded, making exact anatomical reduction impossible. In such chronic cases, the fragment must be excised. The cancellous bed of origin should be meticulously smoothed, and any detached or frayed edges of adjacent articular cartilage must be excised sharply and vertically—never beveled or shaved down—to create stable, perpendicular cartilage walls.
Investigation into resorbable fixation devices has yielded excellent clinical and experimental evidence. Resorbable polydioxanone rods provide satisfactory, low-profile fixation without the need for secondary removal. Alternatively, Pritsch et al. proposed an elegant absorbable suture fixation technique for osteochondral fractures of the patella consisting of large chondral fragments attached to thin slivers of bone.
The Pritsch Suture Technique:
1. The fragment is anatomically reduced into its donor bed.
2. Three holes are drilled using a small Kirschner wire through the fragment and the patella in a triangular configuration.
3. Three Vicryl sutures (Ethicon, Johnson & Johnson, Somerville, NJ) are passed so that each suture traverses two holes. Consequently, each drill hole contains two strands of suture material.
4. The free ends of the sutures are tied securely over the anterior border of the patella, providing broad, compressive fixation.
Intraoperative visualization of an osteochondral defect preparation prior to fixation.

Radiographic confirmation of osteochondral fragment fixation using low-profile implants.
Posterolateral Femoral Condyle Fractures: The Taitsman Approach
Taitsman et al. reported successful outcomes for osteochondral fractures of the posterolateral femoral condyles treated with open reduction and internal fixation (ORIF) using countersunk screws. Preoperative Computed Tomography (CT) is mandatory to determine the exact size, location, and site of origin of the fragment.
Surgical Technique:
1. Anteromedial Incision: Utilized first to retrieve the migrated fragment from the joint space and to repair any associated medial retinacular tears resulting from patellar dislocation.
2. Posterolateral Incision: A second incision is made extending from the lateral epicondyle of the femur distally to the fibular neck.
3. Neurological Protection: The common peroneal nerve is meticulously identified and protected.
4. Deep Dissection: The deep fascia is incised between the biceps femoris tendon anteriorly and the peroneal nerve posteriorly.
5. Capsulotomy: A longitudinal capsulotomy is performed from the meniscal attachment extending to the proximal capsular reflection.
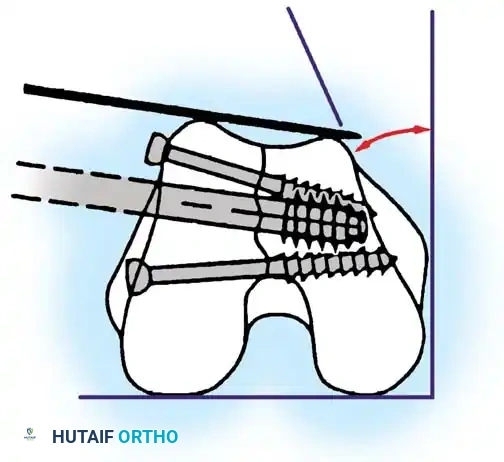
6. Fixation: The fragment is anatomically reduced and provisionally stabilized with Kirschner wires. Definitive fixation is achieved using two 2.0-mm or 2.4-mm screws.
7. Countersinking: It is critical that the screw heads are countersunk 2 to 3 mm below the articular cartilage surface to prevent iatrogenic kissing lesions on the opposing articular surface.
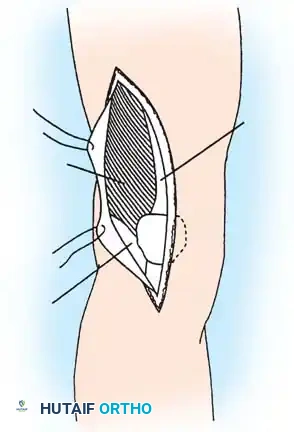
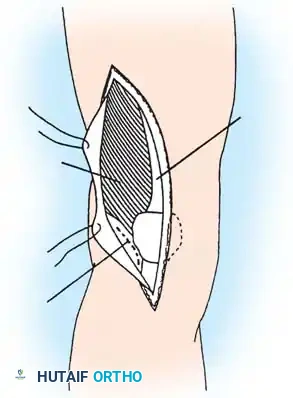
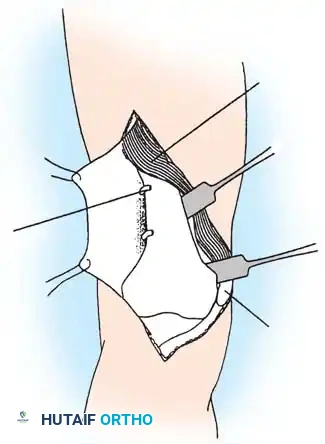
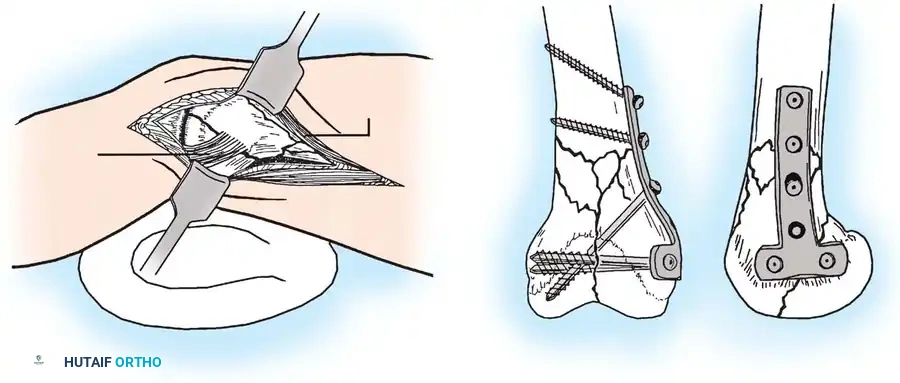
Anatomy and surgical exposure for the posterolateral approach, highlighting the relationship between the peroneal nerve, gastrocnemius muscle, and biceps femoris tendon.

Fig. 51-76 A, Anatomy and surgical exposure. B and C, Intraoperative posteroanterior and lateral radiographs demonstrating successful screw fixation of the posterolateral condyle. (From Taitsman LA, Frank JB, Mills WJ, et al: Osteochondral fracture of the distal lateral femoral condyle: a report of two cases, J Orthop Trauma 20:358, 2006.)
Postoperative Protocol for Osteochondral Fractures
Aftertreatment depends heavily on the adequacy of fixation and the anatomical location of the fracture. Generally, it consists of:
* Immobilization: 3 to 6 weeks in a hinged knee brace.
* Weight Bearing: Touchdown weight bearing only for the first 12 weeks to protect the articular reconstruction.
* Rehabilitation: Continuous Passive Motion (CPM) or active-assisted range of motion is allowed on the first postoperative day to nourish the articular cartilage and prevent arthrofibrosis.
DISTAL FEMUR FRACTURES
The management of distal femur fractures has undergone a paradigm shift over the last several decades. Historically, nonoperative management was the standard of care due to the high complication rates associated with early surgical interventions.
In 1967, Neer, Grantham, and Shelton compared operative and nonoperative treatments in 77 supracondylar and intercondylar femoral fractures. Their findings were stark: nonoperative treatment yielded 84% satisfactory results, whereas operative treatment yielded only 5% satisfactory results, plagued by a 31% malunion rate, 23% infection rate, and 14% nonunion rate. Early internal fixation devices simply lacked the biomechanical stability required to permit early motion, necessitating prolonged postoperative casting which led to severe knee stiffness.
The AO Revolution and Modern Classification
With the development of rigid internal fixation principles by the AO group in Switzerland, treatment recommendations shifted dramatically toward operative intervention. The goal became anatomical reduction of the articular surface, stable internal fixation, and immediate postoperative mobilization.
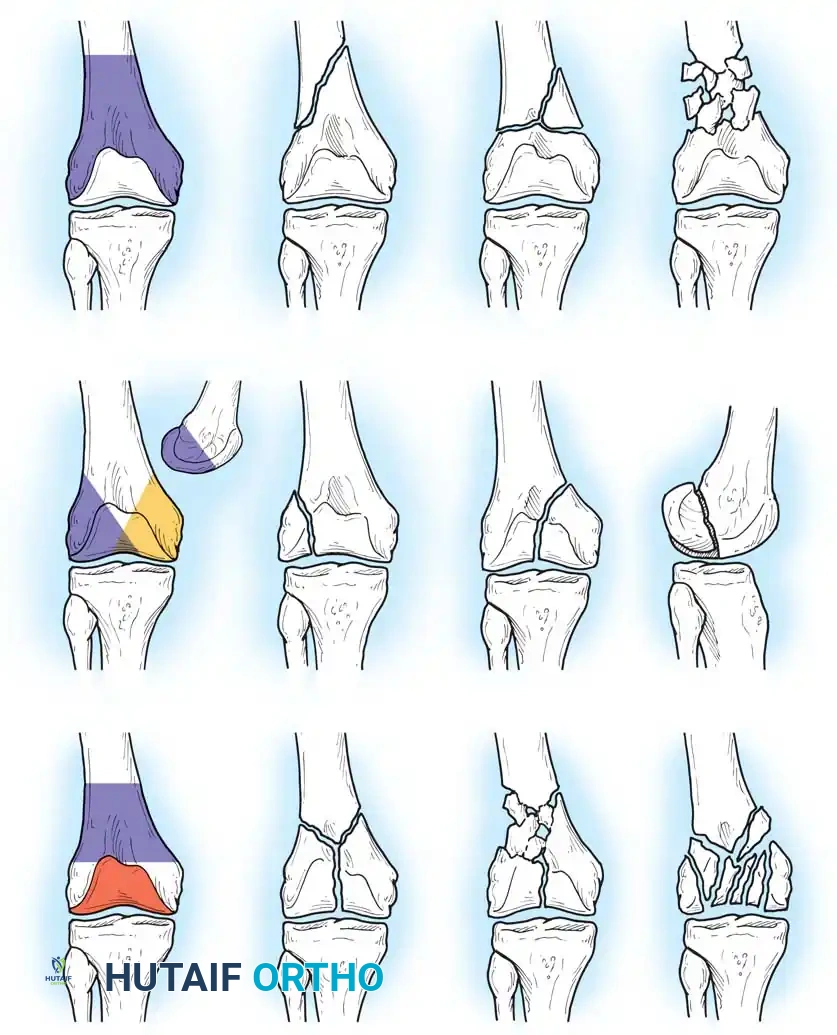
Fig. 51-77 Classification of fractures of the distal femur described by Müller et al. (Redrawn from Müller ME, Nazarian J, Koch P, Schatzker J: The comprehensive classification of fractures of long bones, Berlin, 1990, Springer-Verlag.)
Seinsheimer (1980) evaluated 84 fractures of the distal 9 cm of the femur, emphasizing the critical importance of early range-of-motion exercises. He noted that younger patients achieved better motion and recommended operative treatment for almost all intercondylar fractures (AO types B and C). Subsequent studies by Halpenny, Rorabeck, Healy, and Brooker confirmed that operative treatment with modern implants yielded vastly superior functional results (81% good results) compared to closed methods (35% good results).
Surgical Approaches to the Distal Femur
Achieving adequate exposure while respecting the soft tissue envelope is paramount. The choice of approach depends on the fracture pattern (extra-articular vs. intra-articular) and the planned implant.
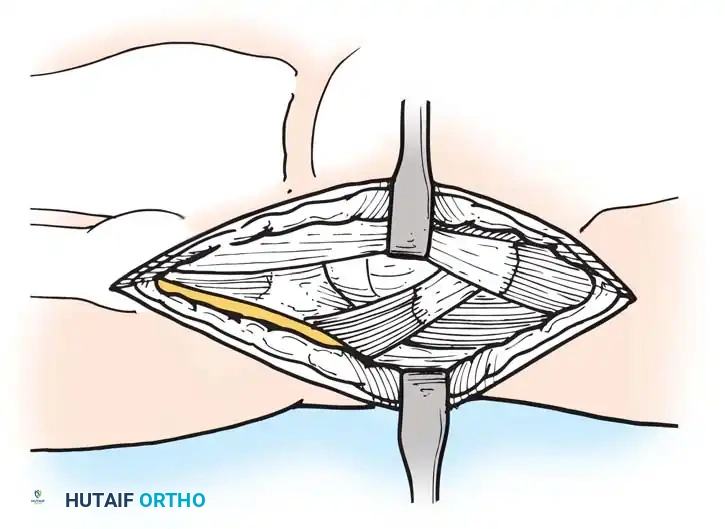
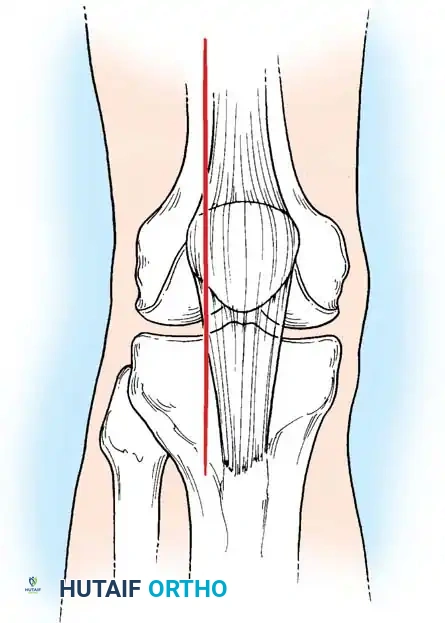
Standard lateral approach to the distal femur, allowing access to the lateral condyle and supracondylar region.

Extensile exposure techniques demonstrating the elevation of the vastus lateralis for plate application.
Anterior midline incision utilized for complex intra-articular (AO Type C) fractures requiring bilateral condylar exposure.
Deep dissection highlighting the capsulotomy and exposure of the intercondylar notch.
Plate and Screw Fixation: The AO Blade Plate
The AO supracondylar blade plate was one of the first devices to provide rigid enough fixation to allow early knee motion. While biomechanically robust, its insertion is technically unforgiving. The blade requires simultaneous accurate insertion in three planes (varus/valgus, flexion/extension, and internal/external rotation).

Fig. 51-78 Fifty-year-old patient with a displaced comminuted supracondylar fracture of the femur internally fixed with an AO supracondylar blade plate and multiple screws.
Schatzker and Lambert highlighted the technical difficulty of this implant, noting that good results were obtained in 71% of fractures with stable fixation, but plummeted to 21% if fixation was inadequate. Siliski, Mahring, and Hofer later reported 81% good or excellent results in severe Type C fractures using blade plates, though intentional shortening of 1 to 3 cm was often required in older patients to achieve bony apposition and stability.
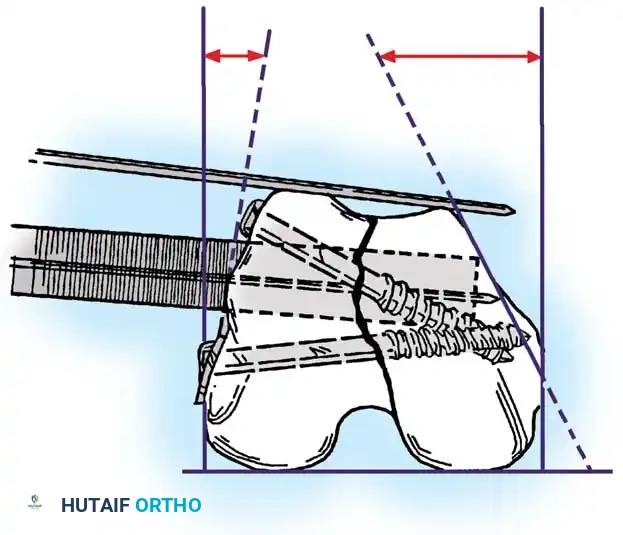
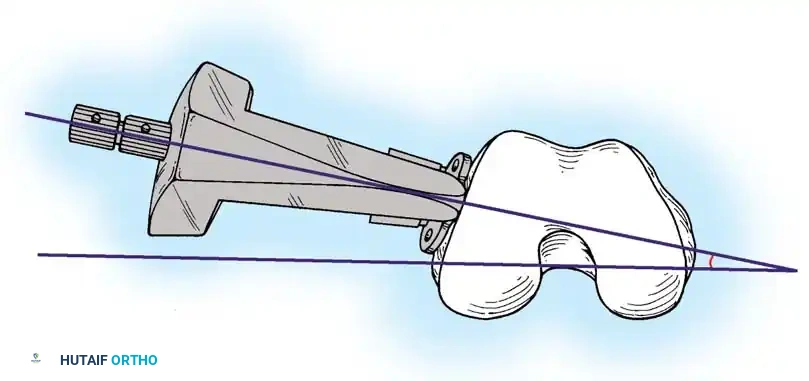
Biomechanical principles of blade plate insertion, requiring precise triplanar alignment.
Provisional K-wire fixation establishing the trajectory for the seating chisel.
Seating chisel insertion preparing the channel for the blade plate.
Final seating of the blade plate and application of interfragmentary compression.
Biological Osteosynthesis
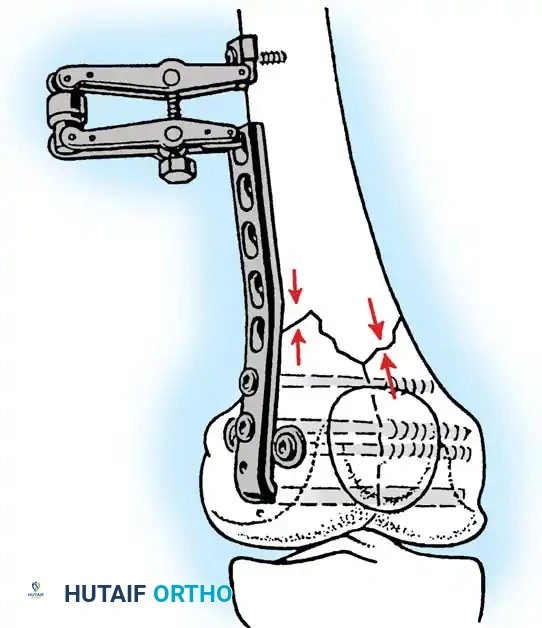
To combat the high rates of infection and nonunion associated with extensive periosteal stripping, modern trauma surgery has shifted toward "biological plating." Bolhofner et al. championed indirect reduction techniques using femoral distractors or external fixators to regain length and alignment. Metaphyseal comminution is left undisturbed in its soft-tissue envelope, and plates are slid submuscularly. This technique resulted in a 0% nonunion rate in their prospective series, drastically reducing the need for primary bone grafting.
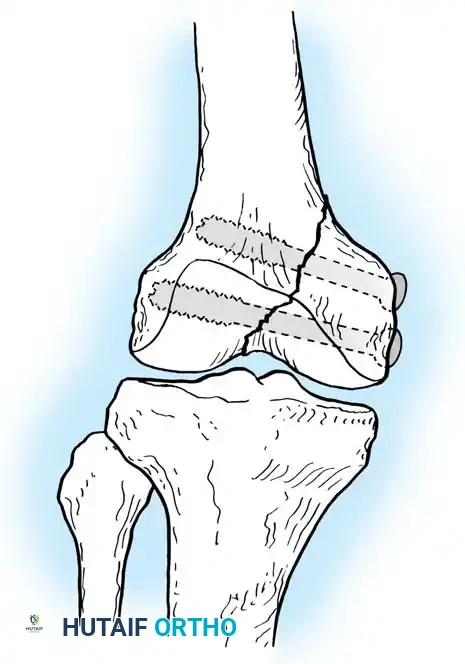
Dynamic Condylar Screw (DCS) Fixation
The Dynamic Condylar Screw (DCS) was developed as a less technically demanding alternative to the blade plate. Because the lag screw is cylindrical, it allows the surgeon freedom of rotation in the flexion-extension plane during plate application, requiring alignment in only two planes rather than three.
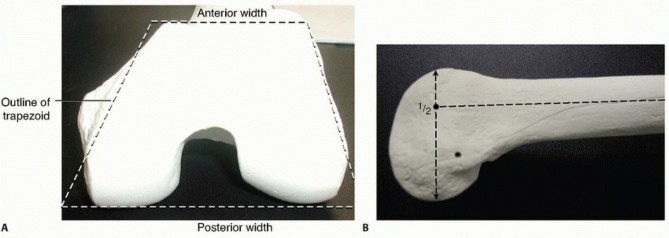
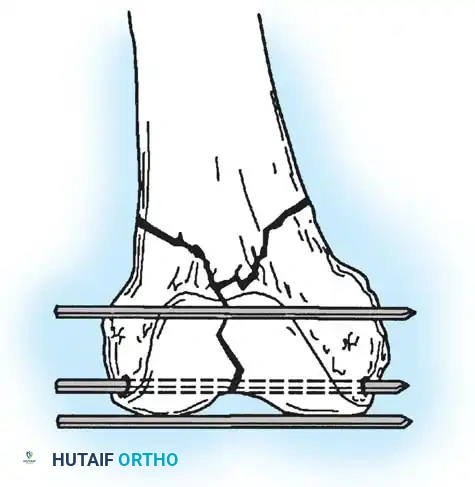
Clinical Pearl: The DCS requires a minimum of 4 cm of uncomminuted bone in the femoral condyles above the intercondylar notch to achieve adequate purchase. If the fracture is highly distal or involves severe articular comminution, the DCS is contraindicated.
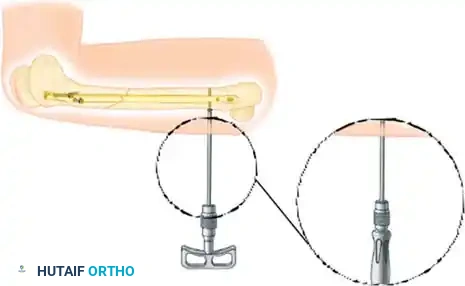
Preparation of the distal femur for DCS insertion, demonstrating the required bone stock.
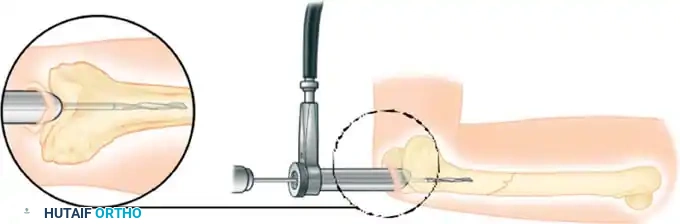
Insertion of the DCS lag screw into the condylar block.
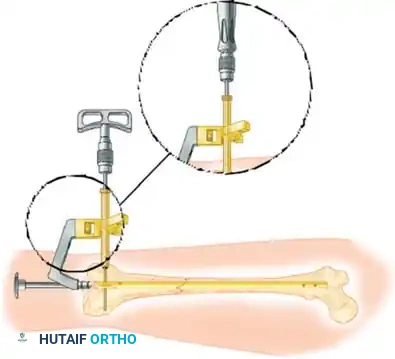
Application of the DCS side plate and compression across the fracture site.
Harder et al. demonstrated that the DCS and the blade plate have similar biomechanical properties under axial loading when the medial cortex is intact. However, in the presence of a medial cortical defect, the DCS allows less interfragmentary movement than the blade plate, making it the implant of choice when sufficient distal bone stock is present. A major disadvantage of the DCS is the large volume of bone removed during reaming, which complicates revision surgery if fixation fails.
Condylar Buttress Plates and Dual Plating
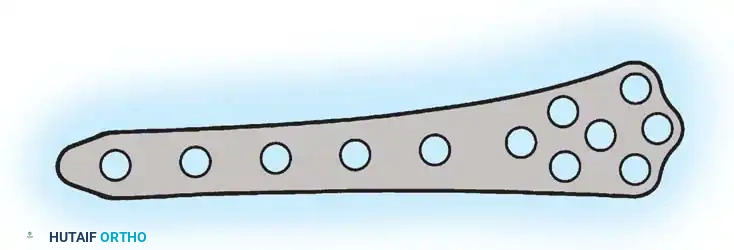
For fractures with less than 3 to 4 cm of intact condylar bone, or those with massive articular comminution, blade plates and DCS constructs are unsuitable. In these scenarios, the condylar buttress plate is utilized. Its multiple distal holes allow for targeted screw placement into small, comminuted articular fragments.
Condylar buttress plate applied to a highly comminuted distal femur fracture.
Multiple distal screws capturing independent articular fragments.
However, a lateral buttress plate alone may fail in varus collapse if there is severe medial comminution or segmental bone loss. To counteract this, dual plating is often required. Chapman and Henley advocated the addition of a medial plate (often an inverted large fragment T-plate) inserted through a separate medial subvastus incision.
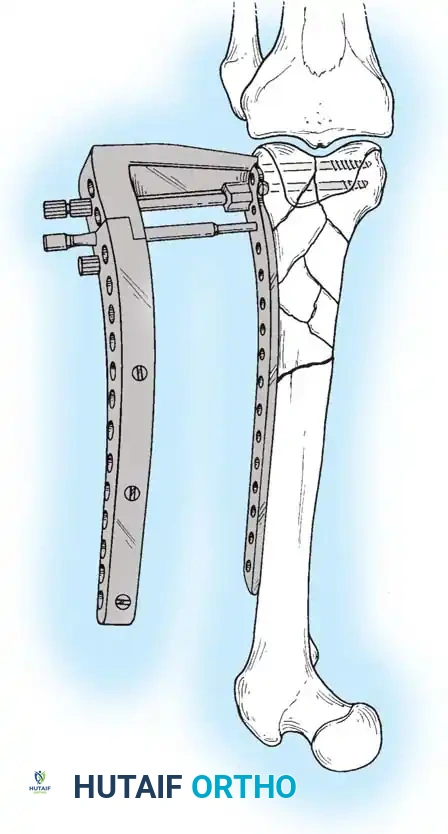
Dual plating technique utilizing a lateral buttress plate and a medial stabilization plate.
Radiographic appearance of a dual-plated distal femur, providing rigid bicolumnar support.
Jazrawi et al. further advanced this concept by describing a locked dual plating technique, which provides superior biomechanical stability in osteopenic bone. Because extensive dual approaches can lead to wound healing complications, percutaneous locked plating techniques have become the gold standard for bridging highly comminuted metaphyseal segments while preserving the vascular supply.
Postoperative Management and Complications
The ultimate success of distal femur fracture fixation relies heavily on the postoperative rehabilitation protocol.
Postoperative AP radiograph demonstrating healed supracondylar fracture with locked plating.
Postoperative Lateral radiograph confirming anatomical sagittal alignment and joint congruity.
Clinical photograph demonstrating excellent postoperative knee flexion following rigid internal fixation and early mobilization.
Standard Protocol:
1. Immediate Post-Op: Range of motion exercises (active-assisted and CPM) are initiated within 24 to 48 hours to prevent quadriceps adhesions and knee stiffness.
2. Weight Bearing: Patients are restricted to touchdown weight bearing (10-15 lbs) for the first 8 to 12 weeks. Progression to full weight bearing is strictly contingent upon radiographic evidence of bridging callus.
3. Complication Management: Nonunion and implant failure are most commonly seen in elderly, osteopenic patients with comminuted intra-articular fractures. In cases of varus collapse or hardware pullout, revision to a locked plate construct with autologous bone grafting, or in severe cases, distal femoral replacement (megaprosthesis), may be indicated.
📚 Medical References
- distal femur fractures, J Orthop Trauma 15:482, 2001.
- Marumo K, Sato Y, Suzuki H, et al: MRI study of bioabsorbable poly-L-lactic acid devices used for fi xation of fracture and osteotomies, J Orthop Sci 11:154, 2006.
- Müller ME, Allgöwer M, Schneider R, et al: Manual of internal fi xation: techniques recommended by the AO-ASIF group, 3rd ed, Berlin, 1990, Springer-Verlag. O’Brien PJ, Meek RN, Powell JN, et al: Primary intramedullary nailing of open femoral shaft fractures, J Trauma 31:113, 1991.
- Pape HC, Dwenger A, Regel G, et al: Pulmonary damage after intramedullary femoral nailing in traumatized sheep—is there an effect from different nailing methods? J Trauma 33:574, 1992.
- Rokkanen P, Böstman O, Vainionpää S, et al: Absorbable devices in the fi xation of fractures, J Trauma 40(3):S123, 1996.
- Russell TA: Biomechanical concepts of femoral intramedullary nailing, J Int Orthop Trauma 1:35, 1991.
- Russell TA, Taylor JC: Interlocking intramedullary nailing of the femur: current concepts, Semin Orthop 1:217, 1986.
- Sanders R, Jersinovich I, Anglen J, et al: The treatment of open tibial shaft fractures using an interlocked intramedullary nail without reaming, J Orthop Trauma 8:503, 1994.
- Sarmiento A, Mullis DL, Latta LL, et al: A quantitative comparative analysis of fracture healing under the infl uence of compression plating vs. closed weight-bearing treatment, Clin Orthop Relat Res 149:232, 1980.
- Sassmannshausen G, Gukay M, Mair SD: Broken or dislodged poly-L-lactic acid bioabsorbable tacks in patients after SLAP lesion surgery, Arthroscopy 22:615, 2006.
- Schatzker J, Tile M: The AO (ASIF) method of fracture care, Instr Course Lect 29:41, 1980.
- Singer RW, Kellam JF: Open tibial diaphyseal fractures: results of unreamed locked intramedullary nailing, Clin Orthop Relat Res 315:114, 1995.
- Sinisaari I, Patiala H, Böstman O, et al: Metallic or absorbable implants for
You Might Also Like