Operative Management of Distal Femur Fractures

Key Takeaway
Distal femur fractures present complex reconstructive challenges due to intra-articular comminution, osteoporotic bone, and proximity to the knee joint. Successful management demands a thorough understanding of fracture biomechanics, precise surgical approaches, and appropriate implant selection. This guide details the indications, operative techniques, and postoperative protocols for utilizing plate and screw constructs, dynamic condylar screws, and intramedullary nailing to achieve anatomical reduction and early mobilization.
INTRODUCTION TO DISTAL FEMUR FRACTURES
Supracondylar and intercondylar fractures of the distal femur historically represent some of the most formidable challenges in orthopedic trauma surgery. These fractures are frequently unstable, highly comminuted, and tend to occur in two distinct demographic populations: elderly patients with osteoporotic bone (often following low-energy falls) and multiply-injured young adults (typically following high-energy trauma). Epidemiologically, the incidence peaks in women older than 75 years and in adolescent boys and men aged 15 to 24 years.
Because of the immediate proximity of these fractures to the knee joint, achieving anatomical reduction of the articular surface and regaining full knee motion and function are paramount, yet notoriously difficult. Historically, the incidences of malunion, nonunion, and deep infection were unacceptably high in many reported series. Furthermore, in the geriatric population, treatment is increasingly complicated by the presence of previous joint arthroplasty, necessitating complex periprosthetic fracture management strategies.
Operative treatment is universally recommended for all fractures of the distal femur, with the rare exception of truly simple, nondisplaced fractures in non-ambulatory patients. The overarching goal of surgical intervention is to restore articular congruity, re-establish mechanical alignment, and provide stable fixation that permits early, aggressive mobilization of the knee.
ANATOMY AND BIOMECHANICS
Understanding the deforming forces acting upon the distal femur is critical for successful reduction and fixation. The distal femur is uniquely shaped, transitioning from a cylindrical diaphyseal tube to a widened, trapezoidal metaphyseal flare, terminating in the medial and lateral condyles.
The muscular anatomy dictates the typical displacement patterns seen in supracondylar fractures:
* Gastrocnemius Muscle: Originating on the posterior aspect of the femoral condyles, the gastrocnemius exerts a powerful flexion force on the distal articular fragment, consistently causing apex-posterior angulation (recurvatum).
* Adductor Magnus: Inserting on the adductor tubercle, this muscle pulls the distal fragment medially, contributing to varus deformity.
* Quadriceps and Hamstrings: These powerful muscle groups cause profound axial shortening and overriding of the fracture fragments.
Surgical Warning: Failure to counteract the apex-posterior deforming force of the gastrocnemius during patient positioning and reduction will inevitably lead to a malunion in extension, severely compromising knee biomechanics and gait.
CLASSIFICATION OF DISTAL FEMUR FRACTURES
The Comprehensive Classification of Fractures of Long Bones (Müller AO/OTA Classification) remains the gold standard for categorizing distal femur fractures. It divides these injuries into three primary types based on articular involvement, which directly dictates the surgical approach and implant selection.
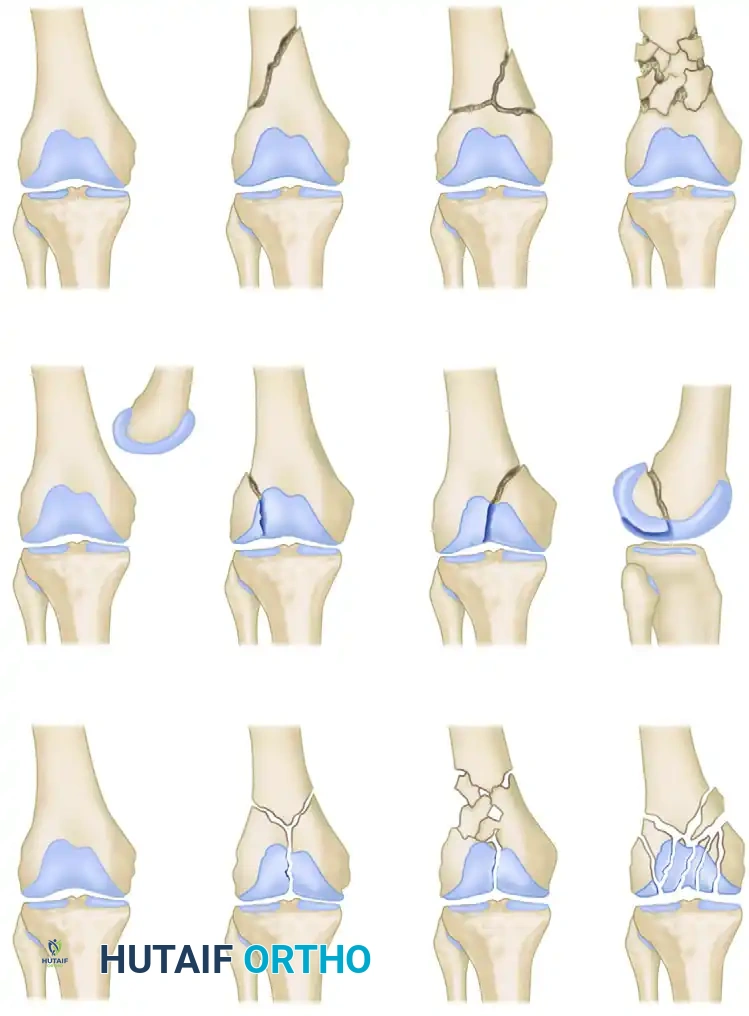
- Type A (Extra-articular): Fractures involving the supracondylar region without extension into the knee joint.
- A1: Simple extra-articular.
- A2: Metaphyseal wedge.
- A3: Metaphyseal complex/comminuted.
- Type B (Partial Articular): Fractures where a portion of the articular surface remains attached to the diaphysis. These are typically sagittal or coronal shear fractures (e.g., Hoffa fractures).
- B1: Sagittal, lateral condyle.
- B2: Sagittal, medial condyle.
- B3: Coronal shear (Hoffa).
- Type C (Complete Articular): Fractures with both supracondylar and intercondylar components, completely dissociating the articular surface from the diaphysis.
- C1: Articular simple, metaphyseal simple.
- C2: Articular simple, metaphyseal multifragmentary.
- C3: Articular multifragmentary.
PREOPERATIVE PLANNING AND POSITIONING
Meticulous preoperative planning is mandatory. High-quality orthogonal radiographs are standard, but a fine-cut Computed Tomography (CT) scan with 2D and 3D reconstructions is now considered essential for all intra-articular (Type B and C) fractures to identify coronal shear fragments (Hoffa fractures) and map articular comminution.
Patient Positioning
- Table Selection: A radiolucent flat table is preferred. A fracture table is rarely used due to the need to manipulate the knee joint.
- Positioning: The patient is placed supine. A sterile bump or a radiolucent triangle is placed under the ipsilateral knee to maintain approximately 30 to 60 degrees of knee flexion. This flexion relaxes the gastrocnemius muscle, neutralizing the apex-posterior deforming force and facilitating reduction of the distal fragment.
- Traction: For severely shortened fractures, a temporary skeletal traction pin placed anteriorly in the distal femur or proximal tibia can be utilized to regain length and prevent posterior angulation.
SURGICAL APPROACHES
The choice of surgical approach depends heavily on the fracture pattern and the planned fixation construct.
Lateral Approach
The standard lateral approach is the workhorse for most distal femur fractures, particularly when utilizing lateral locking plates or dynamic condylar screws.
* Incision: A longitudinal incision is made over the lateral aspect of the distal femur, curving slightly anteriorly toward the Gerdy tubercle if joint exposure is required.
* Deep Dissection: The iliotibial band is incised longitudinally. The vastus lateralis is elevated anteriorly off the lateral intermuscular septum. Perforating vessels must be meticulously identified and ligated.
* Articular Exposure: For Type C fractures, the approach can be extended distally into a lateral parapatellar arthrotomy to visualize the articular surface for anatomical reduction.
Minimally Invasive Plate Osteosynthesis (MIPO)
For highly comminuted metaphyseal fractures (Type A3, C2, C3) where biological preservation is paramount, a MIPO technique is employed. A small distal window is created for articular reduction and plate insertion, while the proximal diaphyseal screws are placed percutaneously through stab incisions, preserving the fracture hematoma and periosteal blood supply.
Medial Subvastus Approach
Occasionally required for dual plating of severe medial comminution or isolated medial condyle fractures. The incision is made along the medial border of the patella, elevating the vastus medialis obliquus (VMO) to expose the medial condyle.
FIXATION TECHNIQUES AND IMPLANT SELECTION
Plate and Screw Fixation (The Blade Plate)
The 95-degree angled blade plate, designed by the AO group in Switzerland, was one of the first plate-and-screw devices to gain wide acceptance for the treatment of distal femur fractures.

Although it provides exceptionally stable fixation for most fractures, the technique is highly technically demanding. It requires simultaneous perfect alignment in three planes (coronal, sagittal, and axial) during the seating of the chisel and subsequent blade insertion. Early historical problems included infection, inadequate fixation in osteoporotic bone, and refracture after plate removal.
However, as experience with AO plating techniques increased and the use of perioperative antibiotics became routine, reported results improved dramatically. Siliski, Mahring, and Hofer (1989) reported good or excellent results in 81% of fractures. Results were notably better in Type C1 fractures (92% good/excellent) compared to the highly comminuted Type C2 and C3 fractures (77%).
Today, more biological techniques of plating are advocated. Using indirect reduction techniques, minimal soft tissue stripping, and gentle retraction, femoral distractors or external fixators are used to regain length and alignment. Metaphyseal comminution is left in situ with no attempt made to anatomically reduce every fragment, thereby preserving the vital soft tissue envelope and reducing the need for primary bone grafting.
Dynamic Condylar Screw (DCS) Fixation
A less technically demanding alternative to the blade plate is the Dynamic Condylar Screw (DCS).

While the blade plate requires accurate insertion in three planes simultaneously, the DCS allows freedom in the flexion-extension (sagittal) plane, simplifying the procedure.
Indications and Limitations:
* A minimum of 4 cm of uncomminuted bone in the femoral condyles above the intercondylar notch is strictly necessary for successful DCS fixation.
* Disadvantage: The insertion of the large-diameter condylar lag screw requires the removal of a significant volume of metaphyseal bone. Should revision surgery be necessary, this bone void makes subsequent fixation highly challenging.
* Outcomes: Reported results are comparable to blade plates, with approximately 87% excellent or satisfactory outcomes. Nonunion rates range from 0% to 5.7%, and malunion from 5.3% to 11%.
Clinical Pearl: The DCS and blade plate are biomechanically similar under axial loading when the medial cortex is intact. However, if a medial cortical defect is present, the DCS construct exhibits less interfragmentary movement than the blade plate. Despite this, the DCS is generally considered unsuitable for severe osteoporotic bone or fractures with massive articular comminution.
Condylar Buttress and Locked Plating Systems
For fractures with less than 3 to 4 cm of intact femoral condylar bone, or those with extensive articular comminution, traditional fixed-angle devices fail. Historically, the condylar buttress plate was utilized, allowing multiple screws to be directed into small comminuted fragments. However, without locking technology, fractures with medial comminution often collapsed into varus due to toggle at the screw-plate interface.
The Advent of Locked Plating:
The introduction of locking plate technology, specifically the Less Invasive Stabilization System (LISS) and modern Locking Compression Plates (LCP), revolutionized distal femur fracture management.
* Biomechanics: Locked screws thread directly into the plate, creating a fixed-angle construct that does not rely on friction between the plate and bone. This mitigates varus angulation even in the presence of a medial femoral defect, often eliminating the historical need for dual (medial and lateral) plating.
* Elastic Deformation: The LISS plate allows for higher elastic deformation than rigid DCS systems, acting as an internal fixator that promotes secondary bone healing via callus formation.
* Modern Implants: Newer locking implants feature polyaxial locking capabilities, allowing the surgeon to angle screws up to 15 degrees off-axis to capture specific articular fragments or avoid existing intramedullary stems in periprosthetic fractures.
Intramedullary Nailing
Intramedullary nailing has become a highly popular and effective method for treating extra-articular (Type A) and simple intra-articular (Type C1/C2) distal femur fractures. Nails offer the biomechanical advantage of being load-sharing devices located closer to the mechanical axis of the limb.
Antegrade Nailing
Antegrade static locked intramedullary nailing is excellent for AO Type A fractures and Type C1/C2 fractures where the articular split extends no closer than 4 to 5 cm from the intercondylar notch.
* Technique: Type C1/C2 fractures with nondisplaced intercondylar splits must first be converted to Type A patterns using percutaneous 6.5-mm cannulated lag screws. Displaced intercondylar fractures require open reduction through an anterior parapatellar incision prior to nailing.
* Pitfalls: The diameter of the nail must fill the isthmus of the femoral canal; an undersized nail allows toggle and subsequent malunion. Distal locking screws must be carefully measured using oblique fluoroscopy; screws that are too long will irritate the medial soft tissues and impede knee flexion.
* Poller (Blocking) Screws: Krettek et al. strongly recommended the use of anteroposterior, medial, and lateral blocking screws placed adjacent to the nail path in the wide metaphysis to artificially narrow the canal, direct the nail, and increase the primary stability of the construct.
Retrograde Nailing
Retrograde femoral nails, inserted through the intercondylar notch, have largely superseded antegrade nails for distal-third fractures.
* Advantages: They require minimal soft tissue dissection, rarely need bone grafting, and are technically easier to insert in obese patients or pregnant women.
* Indications: Retrograde nailing is the treatment of choice for distal femoral fractures below ipsilateral hip implants, above total knee arthroplasties (provided the femoral component has an open notch design), or in the setting of an ipsilateral femoral neck fracture (allowing independent fixation of both injuries).
* Entry Point: The precise entry point is critical: strictly in the center of the intercondylar notch, immediately anterior to the origin of the posterior cruciate ligament (PCL), aligned with the anatomical axis of the femoral canal.
Surgical Warning: Preoperative radiographs and CT scans must be scrutinized for coronal shear (Hoffa) fractures. AO Type C3 fractures with extensive articular comminution are generally best treated with locked plating techniques, as retrograde nailing cannot adequately stabilize complex multifragmentary articular blocks.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The ultimate success of distal femur fracture fixation hinges on the ability to institute early range of motion.
- Immediate Postoperative Phase (0-2 Weeks): The knee is placed in a hinged knee brace. Continuous Passive Motion (CPM) machines may be utilized, though active-assisted range of motion is preferred. The goal is to achieve 90 degrees of flexion by week two to prevent intra-articular adhesions and quadriceps arthrofibrosis.
- Weight-Bearing Status: Weight-bearing is strictly protected. For locked plating and DCS constructs, patients are typically restricted to toe-touch weight-bearing (TTWB) or non-weight-bearing (NWB) for 8 to 12 weeks, depending on radiographic evidence of callus formation. Load-sharing intramedullary nails may allow for earlier partial weight-bearing, dictated by the degree of metaphyseal comminution.
- Long-Term Rehabilitation: Progressive strengthening of the quadriceps and hamstrings begins once clinical and radiographic union is confirmed. Full functional recovery may take 6 to 12 months, and patients should be counseled that some permanent loss of terminal knee flexion is common.
COMPLICATIONS
Despite advances in locking technology and biological plating, complications remain a reality in the management of distal femur fractures.
- Malunion: Varus collapse and apex-posterior angulation are the most common malunions, usually resulting from failure to recognize the deforming forces during positioning or utilizing non-locking implants in osteoporotic bone.
- Nonunion: Aseptic nonunion occurs in up to 5-10% of cases, particularly at the metaphyseal-diaphyseal junction in rigid locking plate constructs that lack sufficient working length. Treatment requires revision fixation, often with bone grafting or the addition of a medial plate.
- Infection: Deep surgical site infections occur in roughly 2-5% of closed fractures and higher in open injuries. Aggressive debridement, hardware retention (if stable), and culture-directed intravenous antibiotics are required.
- Hardware Failure: Plate breakage or screw pullout typically precedes nonunion and is a sign of mechanical failure due to delayed biological healing.
By adhering to strict biomechanical principles, respecting the soft tissue envelope, and selecting the appropriate fixation modality based on the specific fracture pattern, orthopedic surgeons can optimize outcomes and restore function in patients sustaining these complex distal femur injuries.
You Might Also Like

